An Unusual Course and Termination of Small Saphenous Vein: A Case Report
Prakashchandra Shetty1, Melanie Rose D’Souza2, Satheesha B. Nayak3
1 Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Karnataka, India.
2 Associate Professor, Department of Anatomy, Melaka Manipal Medical Collegee (Manipal Campus), Manipal University, Karnataka, India.
3 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Satheesha B. Nayak, Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Madav Nagar, Manipal, Karnataka-567104, India.
E-mail: nayaksathish@gmail.com
The superficial veins of the lower limb can vary in their course and termination. We report a relatively rare type of variation in the course and termination of small saphenous vein. The small saphenous vein had normal origin and course in the leg. However, instead of terminating into the popliteal vein, it continued up in the posterior compartment of the thigh and terminated into the femoral vein after piercing the fleshy part of the adductor magnus muscle. This course might lead to varicosity of the small saphenous vein due to the compression by the fleshy fibres of adductor magus near its termination. The case may be of interest to general and plastic surgeons and even cardiothoracic surgeons.
Lower limb veins, Variation, Varicose veins
Case Report
The present case was observed during the routine dissection of the right lower limb in an approximately 50-year-old male cadaver. The variation was unilateral. The vein on the contralateral limb had a course and termination as mentioned in the anatomy text books. The small saphenous vein had its normal origin and course until it reached popliteal fossa. Upon reaching popliteal fossa, it continued further in the posterior compartment of the thigh gradually becoming deeper in position and thicker in size. Just above the midpoint of the thigh, it pierced the fleshy part of the adductor magnus muscle to enter the anterior compartment of the thigh. The vein was superficial to the tibial nerve behind the knee joint. After crossing the knee, it crossed the tibial nerve from lateral to medial side on the deeper aspect of the nerve. In the posterior compartment of the thigh it ascended on the anteromedial aspect of the sciatic nerve. In the lower third of the thigh the vein was situated behind the popliteal artery. It terminated by opening into the posterior surface of the femoral vein near the apex of the femoral triangle. On its way to femoral vein, it received muscular veins from the posterior compartment of the thigh and also communicated with the popliteal vein through a thick communicating vein [Table/Fig-1,2].
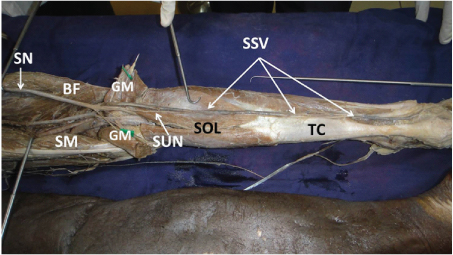
Photograph of dissection of right lower limb showing the course of small saphenous vein.
SSV – small saphenous vein; TC – tendocalcaneus; SOL – soleus; SUN – sural nerve; GM – gastrocnemius; SM – semimembranosus; BF – biceps femoris; SN – sciatic nerve
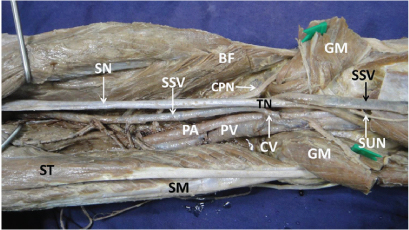
Closer view of the course of the small saphenous vein.
SSV – small saphenous vein; CV – communicating vein; SUN – sural nerve; GM – gastrocnemius; ST – semitendinosus; SM – semimembranosus; BF – biceps femoris; SN – sciatic nerve; CPN – common peroneal nerve; TN – tibial nerve; PA – popliteal artery; PV – popliteal vein
Discussion
Usually, the short (small) saphenous vein arises as a continuation of the lateral marginal vein posterior to the lateral malleolus. It ascends lateral to the calcaneal tendon, inclining medially to reach the midline of calf, emerges at the lower limit of popliteal fossa before terminating into the popliteal vein about 3-7.5 centimetre above the knee joint [1].
Variations in the veins of the lower limb are very common. This may be due to the anomalous involvement of the main trunks of the veins or their tributaries alone. Detailed knowledge regarding the anatomical variations such as reduplication of vein and unusual course and termination of the vein is a prerequisite in the diagnosis and management of vascular diseases.
Embryologically the small saphenous vein represents the post-axial vein of the hind limb bud. During development, it has a direct communication with the posterior cardinal vein, and accompanies the developing ischiadic artery and nerve, as the main vein (ischiadic vein) of the lower limb bud. At the end of its complete development, its proximal part persists as inferior gluteal vein. The subsequent transformation into a short vein opening into the popliteal vein may be an adaptation to the elongation and relative rigidity of the hind limb [2]. In the current case, the vein terminated into the femoral vein. Hence the proximal part of the saphenous vein in this case would have developed from one of the local venous channels of the thigh that persisted later on during development.
Though variations in the course and termination of small saphenous vein are uncommon, a few variant course and terminations have been reported in the literature. Nayak SB has reported an anomalous course of the vein through the gastrocnemius and its possible entrapment in the muscle [3]. In a few cases, the small saphenous vein travels up in the thigh instead of terminating in the popliteal vein. In most of such cases it terminates into the great saphenous vein at variable levels. One such case where it opened into great saphenous vein about one centimetre below sapheno-femoral junction has been reported recently [4]. In some cases, the small saphenous vein terminates into the popliteal vein, but communicates with great saphenous vein through a communicating channel called ‘vein of Giacomini’. This vein is found in 35-90% of the cases as reported in two of the earlier studies [5,6]. The vein being reported here is not Giacomini vein since it terminated into femoral vein. A report on terminal bifurcation of small saphenous vein has also been published [7].
Clinically, the knowledge of small saphenous vein variations is useful during coronary artery bypass grafts as it is increasingly being used as the graft vein [8]. The treatment of varicose veins of lower limb involves ligation of great or small saphenous veins at sapheno-femoral junction and sapheno-popliteal junction [9]. The knowledge of current case is important since the small saphenous vein was opening into the lower part of femoral vein. It may be useful in diagnosis and treatment of small saphenous vein varicosity [10]. Venous congestion is one of the major problems associated with distally based sural artery flap. Intermittent small saphenous vein phlebotomy is performed to reduce venous congestion [11]. Hence plastic surgeons must be aware of variant course and termination of the small saphenous vein.
Conclusion
The unusual course and termination of small saphenous vein in the current case might lead to venous congestion in the lower part of the small saphenous vein since the upper part of it passed through the fleshy part of adductor magnus. The knowledge of variant course and termination might be of use to general surgeons, plastic surgeons and cardiothoracic surgeons.
[1]. Standering S, Grays anatomy: the anatomical basis of clinical practice 2005 39th edLondonElsevier Churchill Livingstone:1452-1487. [Google Scholar]
[2]. Barberini F, Cavallini A, Caggiati A, The thigh extension of the small saphenous vein: a hypothesis about its significance, based on morphological, embryological and anatomo-comparative reportsItal J Anat Embryol 2006 111(4):187-98. [Google Scholar]
[3]. Nayak SB, Sural nerve and short saphenous vein entrapment – a case reportIndian J Plast Surg 2005 38(2):172 [Google Scholar]
[4]. Abhinitha P, Mohandas Rao KG, Satheesha Nayak B, Surekha Shetty D, Kumar N, Anomalous termination of small (short) saphenous vein associated with its abnormal course in the thigh: A case reportOA Case Reports 2013 2(7):63 [Google Scholar]
[5]. Delis KT, Knaggs AL, Khodabakhsh P, Prevalence, anatomic patterns, valvular competence, and clinical significance of the Giacomini veinJ Vasc Surg 2004 40(6):1174-83. [Google Scholar]
[6]. Prakash, Kumari J, Nishanth Reddy N, Kalyani Rao P, Preethi Ramya T, Singh G, A review of literature along with a cadaveric study of the prevalence of the Giacomini vein (the thigh extension of the small saphenous vein) in the Indian populationRom J Morphol Embryol 2008 49(4):537-39. [Google Scholar]
[7]. Krupa Daniel D, Mano A, Nagaveni Bharathi N, Sundarji Valarmathi A case report on abnormal course of vena saphena parvaInt J Anat Res 2015 3(3):1395-98.DOI: 10.16965/ijar.2015.245 [Google Scholar]
[8]. Brandt CP, Greene GC, Maggart ML, Hall WC, Harville LE, Pollard TR, Stouffer CW, Endoscopic vein harvest of the lesser saphenous vein in the supine position: a unique approach to an old problemInteract Cardiovasc Thorac Surg 2013 16(1):1-4.doi: 10.1093/icvts/ivs414. Epub 2012 Oct 9 [Google Scholar]
[9]. Sarwar U, Chetty G, Sarkar P, The Short Saphenous Vein: A Viable Alternative Conduit for Coronary Artery Bypass Grafts Harvested Using a Novel Technical ApproachJ Surg Tech Case Rep 2012 4(1):61-63.doi: 10.4103/2006-8808.100359 PMCID: PMC3461784 [Google Scholar]
[10]. Winterborn RJ, Campbell WB, Heather BP, Earnshaw JJ, The management of short saphenous varicose veins: a survey of the members of the vascular surgical society of Great Britain and IrelandEur J Vasc Endovasc Surg 2004 28(4):400-03. [Google Scholar]
[11]. Wong CH, Tan BK, Intermittent short saphenous vein phlebotomy: an effective technique of relieving venous congestion in the distally based sural artery flapAnn Plast Surg 2007 58(3):303-07. [Google Scholar]