Imperforate Anus with Fistula Exiting at the Penile Skin
Dimitrios Sfoungaris1, Vassilios Mouravas2, Vassilios Lambropoulos3, Chrysostomos Kepertis4, Ioannis Spyridakis5
1 Assistant Professor, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital “G. Gennimatas”, Thessaloniki, Greece.
2 Pediatric Surgeon, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital "Papageorgiou".
3 Pediatric Surgeon, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital "Papageorgiou".
4 Pediatric Surgeon, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital "Papageorgiou".
5 Assistant Professor, Department of Pediatric Surgery, Aristotle University of Thessaloniki, General Hospital "Papageorgiou".
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dimitrios Sfoungaris, General Hospital “G. Gennimatas”, 41, Ethnikis Aminis Str. 54124, Thessaloniki, Greece. E-mail : surgicalpediatrics@gmail.com
We present the case of a male neonate with imperforate anus and a fistula exiting on the penile skin. Anorectal malformations in boys often present themselves with an entero-perineal or entero-urinary tract fistula, the type of which is a key feature for the classification and the treatment plan. A fistula exiting in front of the scrotum, such as described in our case, is very rare and is not incorporated in the current classification and treatment algorithms. Scarce reports on misjudgment concerning the position of the blind rectal pouch in similar cases, led us to perform a colostomy instead of a one-stage correction. A posterior sagittal anorectoplasty was performed eight months later and the rectal pouch was found inside the levator sling, justifying the cautious approach. The colostomy was closed three months later and after six months the distal part of the fistula was excised. We believe that in cases with a rare fistula presentation, the position of the rectal pouch is not predictable and the surgeon should proceed with caution.
Anal atresia, Anorectal malformations, Bifid scrotum, Penile curvature, Penile fistula
Case Report
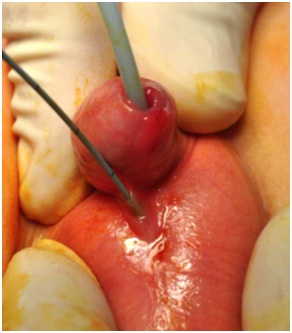
A 3420 g male infant was born after uncomplicated gestation and normal delivery at term. A prenatal ultrasonogram on the 23rd gestational week did not reveal any pathology. Family history was unremarkable. The infant was referred to our facility 8 hours after his birth, in good general status and with slightly distended abdomen. An imperforate anus was evident, with a normally placed anal dimple and a well-formed midline bottom cleft [Table/Fig-1]. The penis was curved ventrally over the midline of a bifid scrotum with bilaterally palpable testes [Table/Fig-2]. The perianal muscles reacted to local scratching. No perineal fistula opening was found. The infant’s urine did not contain meconium. Routine laboratory findings were normal. A thorough ultrasound examination did not reveal any associated anomalies. On 16 hours after birth, traces of meconium appeared at the penile skin where a fistular orifice was found and probed [Table/Fig-3], causing the exit of more meconium.
Imperforate anus with well-formed anal dimple and bottom cleft.


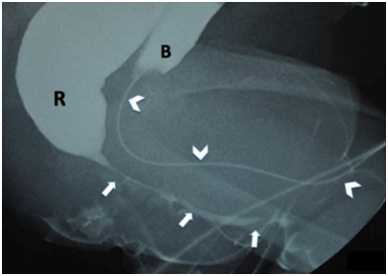
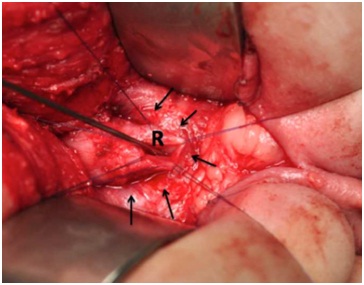
After obtaining parental consent a diverting colostomy was created a couple of hours later. A colostogram under pressure performed in the following days, simultaneously with urethrography, delineated a fistulous tract starting from the rectal pouch, coursing parallel to the urethra and finally exiting through the skin [Table/Fig-4]. We proceeded with posterior sagittal anorectoplasty (PSARP) and ligation of the fistula at the age of 8 months. The rectal pouch was found inside the levator complex [Table/Fig-5]. The peripheral part of the fistula was left in place. The colostomy was closed after 3 months, following a course of anal dilatations, twice daily, increasing the bougie size every week, until a size of 15F was reached. The fistula was excised 6 months later because it contributed to the penile curvature. At that time a barium enema was obtained with normal findings and no rectal dilatation. The child was followed up every three months for a year and once a year for 4 consecutive years. He remains fully continent. He suffered two episodes of constipation for which he visited our service 14 and 18 months after colostomy closure, which were promptly resolved with enema.
Colostogram and urethrography. Course of recto-penoscrotal fistula (arrows) and urethra (arrowheads). R: rectum, B: urinary bladder.
Levator complex (arrows) and rectum (R).
Discussion
Anorectal malformations (ARMs) have been reported from about 1 to 5 per 10,000 live births, with a slight preponderance in males [1–3]. They represent a vast spectrum of lesions which have been described to stem from defective partition of the cloaca and mal-development of the perineal mound and genital folds [4] or from a defect of the dorsal part of the cloacal membrane, allowing the growth of mesenchyme, which diverts the anal opening at a perineal or urogenital site [5]. In the male, the fast and extensive growth of the perineum causes the extinction of the would-be fistulas exiting in front of the scrotum, the homologue of which in females (anovestibular fistula) is very common and which is considered to accompany low type anomalies [5].
ARMs are termed as “high”, “intermediate” and “low” according to the position of the blind rectal pouch in relation to the muscle complex of the pelvic floor [2]. A diagnosis must be reached on this matter in the neonate because this determines whether a colostomy is necessary before the anorectopasty [2]. Typically, a low (infralevator) type of ARM is accompanied by a formed anal dimple reacting to local stimuli and a well-formed midline bottom cleft [2,6], such as was present in our case.
The majority of male patients (80-90%) have evidence of a fistula [2,7]. The location of the fistular exit correlates in general with the position of the blind rectal pouch and with prognosis [2,6,7]. An anoperineal fistula, exiting between the scrotum and the anal dimple is usually present in low cases. A rectourethral or rectovescical fistula accompanies high type of ARMs and is revealed by meconium in the urine. In our case, meconium appeared discharging from an opening on the penile skin several hours after birth, revealing a type of fistula (rectopenile) which is not incorporated in the current classification and treatment algorithms for ARMs [2].
Our case’s morphological findings advocate for a low type of anomaly, which can be corrected by either a cutback procedure or a minimal PSARP [2,8]. However, the fistula was not typical for a low ARM. Our decision to manage the case as a high type of ARM was reached by consulting the few relevant suggestions in literature.
We have found reports on 19 ARM cases with fistulas exiting in front of the scrotum, [1,9–11], four of which were observed among 1,183 boys with ARMs, during a 20-year period in Japan [1]. These reports are mainly registrations in statistical surveys and give little and diverse information about the cases themselves, which were treated either as low or high type anomalies, without any justification being mentioned in the publications. In only one report [9] was the case directly reported, thoroughly described and treated as a high type ARM, which case we used as a paradigm for our treatment plan. Even among children with fistulas exiting in the perineum, there have been described cases with a high type anomaly [12,13]. During the PSARP procedure in this case, the rectal pouch was found inside the levator complex, justifying our the choice to perform initially a colostomy.
The long-term results in ARMs, considered initially of favourble prognosis, are impaired in 15% up to one- half of the patients [7,8]. In these cases, constipation and occasional soiling have been related to neurological damage and mental retardation, insufficient long term follow-up and care, and to the presence of a tethered cord [6,8]. Also, some of these children have growth and motor impairment [14].
ARMs with perineal fistulas are associated in more than 70% with enteric nervous system abnormalities in the terminal intestine and minimal approaches, without resecting the terminal part, could lead to a significant persistence of abnormally innervated neoanorectal canal. Additionally, no “internal sphincter” has been found in the terminal part of the intestine or the fistula in these cases that could contribute to reduced soiling. We believe that in cases with even more aberrant fistulas, one should be even more discouraged to preserve the most distal enteric tissue [15].
Conclusion
In case of atypical presentation of an otherwise looking like “low” ARM, we think that the surgeon should proceed with a colostomy deferring the definitive procedure. Atypical presentations do not necessary fit under general treatment guidelines and there is an increased possibility for important rectal mobilization and PSARP to be needed for the correction. A more restricted type of operation might leave behind a dysfunctional enteric tissue and will not offer the space for a good anatomical reconstruction.
[1]. Endo M, Hayashi A, Ishihara M, Maie M, Nagasaki A, Nishi T, Analysis of 1,992 patients with anorectal malformations over the past two decades in Japan. Steering Committee of Japanese Study Group of Anorectal AnomaliesJ Pediatr Surg 1999 34(3):435-41. [Google Scholar]
[2]. Levitt MA, Peña A, Anorectal malformationsOrphanet J Rare Dis 2007 2:33 [Google Scholar]
[3]. Cuschieri A, EUROCAT Working Group Descriptive epidemiology of isolated anal anomalies: a survey of 4.6 million births in EuropeAm J Med Genet 2001 103(3):207-15. [Google Scholar]
[4]. Douglas Stephens F, Durham Smith E, John Hutson, Congenital Anomalies of the Kidney, Urinary and Genital Tracts 2002 2nd ednMartin Dunitz:3-37. [Google Scholar]
[5]. van der Putte SC, Normal and abnormal development of the anorectumJ Pediatr Surg 1986 21(5):434-40. [Google Scholar]
[6]. Arnoldi R, Macchini F, Gentilino V, Farris G, Morandi A, Brisighelli G, Anorectal malformations with good prognosis: variables affecting the functional outcomeJ Pediatr Surg 2014 49(8):1232-36.doi: 10.1016/j.jpedsurg.2014.01.051 [Google Scholar]
[7]. Nam SH, Kim DY, Kim SC, Can we expect a favourable outcome after surgical treatment for an anorectal malformation?J Pediatr Surg 2015 pii: S0022-3468(15)00562-X. doi: 10.1016/j.jpedsurg.2015.08.048 [Google Scholar]
[8]. Pakarinen MP, Rintala RJ, Management and outcome of low anorectal malformationsPediatr Surg Int 2010 26(11):1057-63.doi: 10.1007/s00383-010-2697-z [Google Scholar]
[9]. Shah AA, Shah AV, Imperforate anus with rectopenile fistulaPediatr Surg Int 2003 19(7):559-61. [Google Scholar]
[10]. Currarino G, The various types of anorectal fistula in male imperforate anusPediatr Radiol 1996 26(8):512-22. [Google Scholar]
[11]. Fitzgerald RJ, Watters K, Bissett WH, Bjordal R, Monclair T, Translevator anal anomalies with cutaneous fistulae passing deep to the scrotumJ Pediatr Surg 2002 37(9):1326-29. [Google Scholar]
[12]. Shanbhogue LK, Langemeijer RA, Madern GC, Molenaar JC, Rectoperineal fistula in newborn boysJ Pediatr Surg 1994 29(4):536-37. [Google Scholar]
[13]. Kumaran N, Kirby CP, Cusick E, Anorectal malformation with recto-perineal fistula: case report and clues to diagnosisJ Pediatr Surg 2003 38(9):E4-5. [Google Scholar]
[14]. van den Hondel D, Sloots CE, Gischler SJ, Meeussen CJ, Wijnen RM, IJsselstijn H, Surgical Long-term Follow Up team. Prospective long-term follow up of children with anorectal malformation: growth and development until 5years of ageJ Pediatr Surg 2013 48(4):818-25.doi: 10.1016/j.jpedsurg.2012.09.068 [Google Scholar]
[15]. Lombardi L, Bruder E, Caravaggi F, Del Rossi C, Martucciello G, Abnormalities in "low" anorectal malformations (ARMs) and functional results resecting the distal 3 cmJ Pediatr Surg 2013 48(6):1294-300.doi: 10.1016/j.jpedsurg.2013.03.026 [Google Scholar]