Biliary Cystadenoma: A Case Report
Johnsy Merla Joel1, Suresh Durai Jeyasingh2, Shantaraman Kalyanaraman3
1 Assistant Professor, Department of Pathology, Tirunelveli Medical College, Tirunelveli, Tamil Nadu, India.
2 Professor, Department of Pathology, Tirunelveli Medical College, Tirunelveli, Tamil Nadu, India.
3 Professor and HOD, Department of Pathology, Tirunelveli Medical College, Tirunelveli, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Johnsy Merla Joel, Assistant Professor, Department of Pathology Tirunelveli Medical College, Tirunelveli-627011, Tamil Nadu, India.
E-mail: drjohnsymerla@gmail.com
Biliary cystadenoma is a rare cystic neoplasms of liver that usually occurs in middle-aged women characterized by multiloculated cysts with internal septae and mural nodules. Unilocular biliary cystadenomas are rare and are difficult to differentiate from other cysts by radiology. Biliary cystadenomas are slow growing benign lesions that are easily resectable with a reported recurrence rate of 90% when the resection is incomplete. We present a case of 65-year-old male with unilocular biliary cystadenoma with mesenchymal stroma who presented with abdominal pain and distension. Laparotomy followed by cystectomy was done and postoperative period was uneventful with no abnormal biochemical, heamatological or imaging findings. Preoperative radio-imaging techniques may not always be helpful in arriving at a specific diagnosis in such cases. Hence thorough sampling and a careful histopathological examination is considered gold standard for specific diagnosis.
Benign liver lesion, Mesenchymal stroma, Unilocular
Case Report
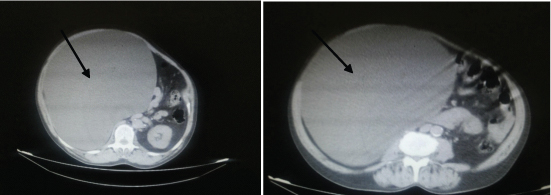
We report here a 65-year-old man who presented in the General Surgery outpatient department of the hospital with pain abdomen since 2 weeks and abdominal distension since one year. He was examined as per standard clinical protocols. On general examination he was moderately built and moderately nourished with a huge firm abdominal mass in the right hypochondrium extending into the epigastrium, right lumbar region and extending down to a point 5cm above the anterior superior iliac spine. The other systemic examinations were normal. Ultrasound (USG) examination of the abdomen revealed a cystic lesion in right hypochondrium extending into the epigastrium causing displacement of liver and the right kidney laterally for which a clinical diagnosis of Hydatid cyst or cystic hemangioma was made. Computerized tomography (CT) scan of abdomen revealed a large 25 x 23 cm cystic mass filling the right hypochondrium, epigastric, right flank upto the right iliac fossa and a radiological diagnosis of mesenteric cyst or retroperitoneal cyst of undetermined origin was offered [Table/Fig-1]. The patient was investigated for his Liver function and full blood count, which were within normal limits. The patient underwent a laparotomy that revealed a large cyst attached to the inferior surface of liver which was followed by a cystectomy and the fully resected cyst was sent for histopathological examination.
Abdominal CT showing an unilocular cystic mass filling the right hypochondrium, epigastric region causing displacement of right kidney.
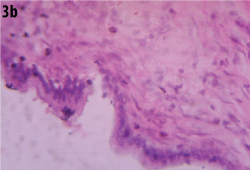
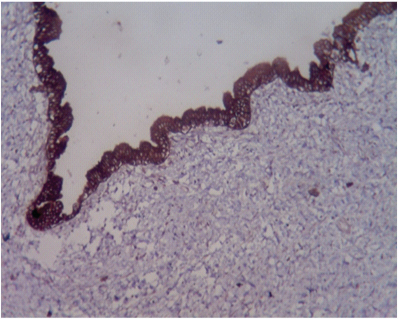
Gross examination showed an unilocular cystic lesion measuring 17 x 10 cm with a pale grey smooth cyst wall. [Table/Fig-2] of thickness that varied from 0.2 cm to 0.8 cm. On histology of the lesion showed a cyst wall internally lined by an epithelium of biliary type of columnar epithelium with focal pseudostratification and basally oriented nuclei with foci of apical mucin, no nuclear or cellular atypia and an underlying mesenchymal stroma that was resemblent of the ovarian stroma. Hence a diagnosis of biliary cystadenoma was offered [Table/Fig-3a,b] Immunohistochemistry of the tumour was positive for Cytokeratin in the epithelial cells [Table/Fig-4]. A final diagnosis of biliary cystadenoma was made.
Gross photograph revealing a unilocular cystic lesion with a smooth wall lining.

Lesion composed of biliary type of epithelium with underlying mesenchymal stroma resembling ovarian stroma. (H&E, 100X).
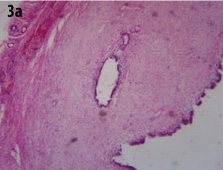
Lesion composed of biliary type of columnar epithelium with focally pseudostratified areas and basally oriented nuclei and apical mucin with no atypia with mesenchymal stroma. (H&E, 400X).
Photomicrograph showing cytokeratin positivity in epithelial cells.
Pancytokeratin (100X).
The postoperative course of the patient was uneventful and he was discharged one week later. Six months after surgical resection the patient is in excellent clinical health with no indication for abnormal biochemical, heamatological or imaging findings.
Discussion
Biliary cystadenoma of the liver are rare benign lesions of the liver that account for less than 5% of solitary cysts [1] of the liver and occur commonly in middle-aged women (40-50years) with preponderance of 4:1 among males [2]. These tumours present commonly as multiloculated cysts while unilocular biliary cystadenomas are rare [3]. These biliary cystadenomas are easily resectable tumours with rare reports of recurrences after complete resection [4] and are best diagnosed by histopathology. Hence it is important to differentiate these tumours from other common cystic lesions of the liver.
Biliary cystadenomas are potentially malignant multilocular cystic neoplasms of the billiary ductal system accounting for less than 5% of cystic neoplasms of the liver [5]. Unilocular biliary cystadenomas are rare and have been reported as intra-hepatic biliary cystadenomas [3]. These neoplasms are reported in middle-aged women as true proliferative epithelial tumours that are large multiloculated with internal septations and surrounded by a dense cellular fibrostroma [2,4]. The cyst is lined by a single layer of biliary-type epithelium, that is usually columnar, but may be focally flattened, denuded, or pseudostratified, and show areas of squamous metaplasia [1] with basally oriented nuclei and apical mucin. These cysts usually contain clear mucinous fluid while bloody fluid signifies a malignant transformation [2]. Rarely, the fluid within the cyst may be bilious, purulent, proteinaceous or gelatinous [4].
The cystadenomas are divided into two subgroups that are distinguished by presence or absence of mesenchymal (ovarian like) stroma [6]. Biliary cystadenomas with mesenchymal stroma occuring exclusively in women [1]. Rarely biliary cystadenomas may present as unilocular cystic lesions as in this patient [3].
On CT scan and Ultrasonography, it is hard to differentiate unilocular biliary cystadenoma from other cysts. Under CT scan, cystadenomas are usually seen as well demarcated lesions with contrast enhanced walls or septae, low density well defined, lobulated, multilocular thick walled cystic masses and rarely coarse calcification along the wall of septa in a multilocular cystic mass that indicates a more likely diagnosis of cystadenocarcinoma [7]. All these features are essential for differentiating cystadenoma from other cystic liver lesions, but due to the rarity of the disease a preoperative diagnosis is rarely suspected [5]. In many patients a differential diagnosis of hydatid cyst is thought of due to curtained shared radiological features. Similarly there are no significant differences in the imaging findings between intrahepatic and extrahepatic biliary cystadenomas [3].
In a clinical study of a series of 13 cases of biliary cystadenoma by Sastha Ahanatha Pillai et al., there were eleven women and two men. The median age of the patients was 46 years (range 23–65 years). The most common symptom was abdominal pain (92%), followed by abdominal distension [8]. Ju- Hyn Park-et al., reported a case of unilocular extrahepatic biliary cystadenoma in 42-year-old women which was erroneously diagnosed as choledochal cyst by preoperative radiological investigations [9].
Patients with cystadenoma with mesenchymal stroma have a good prognosis when compared to cystadenomas without mesenchymal stroma, especially in men. Histopathologic examination of the resected specimens constitutes an important diagnostic modality for biliary cystadenomas and can detect malignant degeneration of a cystadenoma. The prognosis of a completely resected billiary cystadenomas is good and recurrence is reportedly rare [4].
Conclusion
Although most of the biliary cystadenomas occur in middle aged women and manifest as a multilocular cystic mass, this case occurred in an old aged male as an unilocular cystic lesion with mesenchymal stroma. The differential diagnosis of any cystic lesion in the liver should always include biliary cystadenoma.
[1]. Mills Stacey E, Carter Darryl, Sternbergs Diagnostic Surgical Pathology 2010 5 edWolter Kiuwer, Lippincott Williams & Wilkins [Google Scholar]
[2]. Florman SS, Slakey DP, Giant biliary cystadenoma: case report and literature reviewAm Surg 2001 67:727-32. [Google Scholar]
[3]. Choi BI, Lim JH, Han MC, Biliary cystadenoma and cystadenocarcinoma: CT and sonographic findingsRadiology 1989 171:57-61. [Google Scholar]
[4]. Manouras A, Markogiannakis H, Lagoudianakis E, Atergiannakis K, Biliary cystadenoma with mesenchymal stroma: report of a case and review of the literatureWorld J Gastroenterology 2006 12:6062-69. [Google Scholar]
[5]. Tsepelaki A, Kirkilesis I, Katsiva V, Triantafillidis JK, Vagianos C, Biliary Cystadenoma of the Liver: Case report and systematic review of the literatureAnnals of gastroenterology 2009 22(4):278-83. [Google Scholar]
[6]. Dixon E, Sutherland FR, Mitchell P, McKinnon G, Nayak V, Cystadenomas of the liver: a spectrum of diseaseCan J Surg 2001 44:371-76. [Google Scholar]
[7]. Koroglu M, Akhan O, Akpinar E, Oto A, Gumus B, Biliarycystadenoma and cystadenocarcinoma: two rare cystic liver lesionsJBR-BTR 2006 :89261-63. [Google Scholar]
[8]. Sastha Vimalraj Senthilkumar Srinivasan Anand Sukumar Biliary Cystadenomas: A Case for Complete ResectionHPB Surgery 2012 2012:501705 [Google Scholar]
[9]. Park JH, Lee DH, Kim HJ, Ko YT, Lim JW, Yang MH, Unilocular Extrahepatic Biliary Cystadenoma Mimicking Choledochal Cyst: A Case ReportKorean J Radiol 2004 5(4):287-90. [Google Scholar]