Introduction
Anti-Mullerian Hormone (AMH) is a glycoprotein of the transforming growth factor-β (TGF-β) family that seems to reflect the continuous non-cyclical growth of small follicles and can be considered an indirect index of the size of the resting primordial follicle pool. Accordingly, AMH represents a marker of Ovarian Reserve (OR) and is particularly useful in demonstrating ovarian tissue damage induced by chemotherapy.
Aim
To evaluate and compare the levels of AMH in Breast Carcinoma patients before and after chemotherapy with age matched healthy controls and to assess whether AMH as a biochemical marker of the OR might improve prediction of chemotherapy related outcomes in these patients.
Materials and Methods
The present study was conducted in the Department of Biochemistry in collaboration with Department of Radiotherapy, Pt. B.D. Sharma, University of Health Sciences, Rohtak between June 2013 and June 2014. The subjects were divided into two groups. A total of 30 female patients of confirmed diagnosis of breast carcinoma were enrolled in the study group (Group I). The enrolled breast cancer cases were further divided into subgroups (Group-IA=Prechemotherapy & Group-IB= Postchemotherapy). Thirty healthy age matched female volunteers were enrolled as controls (Group II). Serum levels of AMH were determined by the ultrasensitive anti-müllerian hormone/ müllerian inhibiting substance (US AMH/MIS) Enzyme Linked Immuno Sorbent Assay (ELISA).
Results
There was a significant decrease in serum AMH levels in the both study group-IA and study group-IB as compared to control group-II (p<0.05 and p<0.001 respectively). The prechemotherapy (group-IA) serum AMH levels dropped significantly after chemotherapy (group-IB) (p<0.001).
Conclusion
AMH levels declined after chemotherapy indicates direct chemotherapy induced damage to the granulosa cells and growing follicles, reflecting decrease ovarian reserve and fertility.
FEC, Females, Fertility, Granulosa cells, Ovarian reserve
Introduction
Chemotherapy is well known for causing deleterious effects on reproductive function in females. Chemotherapy causes acute loss of growing follicles resulting in premature ovarian failure, shortened reproductive life span and hormone deficiency [1,2].
About 1 million primordial ovarian follicles are present in females at birth which declines to 180,000 at menarche and to 1,000 at menopause [3]. The number of oocytes containing both primordial follicles and the relatively small number of maturing, growing follicles in a woman’s reproductive life is called as Ovarian Reserve (OR).
Young women with more primordial oocytes, showed a sharp reduction of their OR following chemotherapy [4]. The destructive effect on the primordial follicles is dose-dependent and varies with the age, type and the dose of cytotoxic agents used and developmental maturity of the patient at the time of the therapy, with older women more likely to be left infertile later on [5,6]. Alkylating agents covalently bind an alkyl group to the DNA molecule and inhibit it from replicating [7]. They also damage the ovarian vasculature so that the follicles cannot grow [8]. Use of cyclophosphamide an alkylating agent leads to premature ovarian failure and infertility [9].
Follicle Stimulating Hormone (FSH) and Antimüllerian Hormone (AMH) are the hormones that are secreted from anterior pituitary gland and ovaries, are important for the development of follicles. Women with abnormal levels of these hormones shows decreased ability or inability of conception [10].
Serum FSH levels in the early follicular phase and age of the women are most commonly used parameters for assessing ovarian function [11,12]. Most investigators during their studies prior to ovulation induction in assisted reproduction used ultrasound markers such as ovarian volume [13,14] and antral follicle count (AFC) [15,16]. Developing antral follicles in ovaries secrets E2 and inhibin B. Increased levels of these hormones signals the gonadotropins in the pituitary gland to discontinue the release of FSH resulting in variability in FSH levels during menstrual cycle [10].
AMH is a glycoprotein hormone belonging to transforming growth factor b family. It’s levels reflect the continuous non-cyclical growth of small follicles [17]. AMH is produced by the granulosa cells (GC) of primary follicles is distinct from ovulation being able to measure true OR [18]. AMH accurately measure the active follicle pool being produced by them and hence the basis of assessing OR [19].
AMH levels does not change significantly throughout the menstrual cycle unlike the other markers of OR [20]. Hence serum AMH level seems to be the more convenient and effective than other serum OR tests like FSH, inhibin B or E2 [21].
For assessing post-chemotherapy ovarian function the primary and gold standard tool used commonly is presence or absence of menstruation. There is a need for valid tools for measuring and predicting reproductive function in this population [22].
Aim
Hence the present study was planned to evaluate and compare the levels of AMH in breast cancer patients before and after chemotherapy and to assess whether AMH as a biochemical marker of the OR might improve prediction of chemotherapy related outcomes.
Materials and Methods
This observational study was approved by the Ethics Review Committee of the institute in which the study was carried out. All patients were recruited after obtaining informed consent. The present study was conducted in the Department of Biochemistry in collaboration with Department of Radiotherapy, Pt. B.D. Sharma, University of Health Sciences, Rohtak between June 2013 and June 2014. The study included purposive sampling.
The subjects were divided into two groups.
Group I: A total of 30 female patients of confirmed diagnosis of breast carcinoma after TNM staging from the department of radiotherapy were enrolled in the study group. The enrolled breast cancer cases were further divided into subgroups (Group-IA= Prechemotherapy & Group-IB= Postchemotherapy).
Group II: A total of 30 healthy age matched female volunteers from Out Patient Department were enrolled as controls.
Anticancer regimen- 5-FU, Epirubicin, Cyclophosphamide (FEC) given for four cycles followed by four cycles of docitaxel to each patient. The same patients were followed postchemotherapy for estimation of AMH levels. Each cycle is followed by the next after a period of 3 weeks. Estimation of serum AMH was done by a sandwich Enzyme Linked-Immuno-Sorbent Assay (ELISA) [23].
Principle: An antibody specific for human AMH is coated onto the wells of the microtiter plate. Samples and standards of human AMH are pipetted into the wells for binding to the coated antibody. The unbound antibodies are removed by washing. The substrate solution is added to the wells and colour develops in proportion to the amount of human AMH bound to antibody in the initial step. The intensity of the colour is measured and the absorbance is proportional to the amount of human AMH.
Results
[Table/Fig-1] mentions about the serum AMH levels- The study group-IA (prechemotherapy) AMH value ranged between 0.82- 2.76 ng/mL (mean ± SD=1.67 ± 0.44) as compared to 1.24 - 2.68 ng/mL of control group (group II) (mean± SD=1.9 ± 0.37) and this difference was statistically significant (p<0.05).
Serum AMH levels in study group-IA (Prechemotherapy) and control group-II. (S= Significant)
| GROUP | AMH (ng/mL) |
|---|
| Study Group (IA) | 1.67 ± 0.44 |
| Control Group (II) | 1.9 ± 0.37 |
| p-value | <0.05 |
| Significance | S |
The study group-IB (postchemotherapy) AMH value ranged between 0.54 - 1.78 ng/mL (mean ± SD=1.03 ± 0.25) as compared to 1.24-2.68 ng/mL control group (group II) (mean ± SD=1.9 + 0.37) and was found to be statistically highly significant (p<0.001) [Table/Fig-2].
Serum AMH levels in study group-IB (postchemotherapy) and control group-II. (HS= Highly Significant)
| GROUP | AMH (ng/mL) |
|---|
| Study Group (IB) | 1.03 ± 0.25 |
| Control Group (II) | 1.9 ± 0.37 |
| p-value | <0.001 |
| Significance | HS |
The group-IB (postchemotherapy) AMH mean ± SD value was 1.03 ± 0.25ng/mL and that of prechemoherapy group (group-IA) was mean ± SD=1.67 ± 0.44ng/mL and p<0.001 which was statistically highly significant [Table/Fig-3].
Serum AMH levels in study group-IA (Prechemotherapy) and study group-IB (Postchemotherapy). (HS= Highly Significant)
| GROUP | AMH (ng/mL) |
|---|
| Study Group (IA) | 1.67 ± 0.44 |
| Study Group (IB) | 1.03 ± 0.25 |
| p-value | <0.001 |
| Significance | HS |
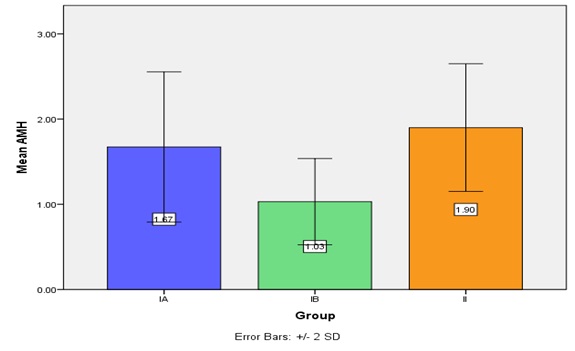
[Table/Fig-4] depicts mean + SD serum AMH levels in study group (group-IA & IB) and control group-II.
Showing mean + SD serum AMH levels in study group (group-IA & IB) and control group-II.
Discussion
In the present study we found that there is significant decrease in serum AMH levels in study group as compared to control group both before and after chemotherapy. [Table/Fig-1,2] showed that there was a significant decrease in serum AMH levels in the both study group-IA and study group-IB as compared to control group-II (p<0.05 and p<0.001 respectively).
The prechemotherapy (group-IA) serum AMH levels dropped significantly after chemotherapy (group-IB) (p<0.001) (as shown in [Table/Fig-3]). Our study supports the common opinion was that chemotherapy affects the OR by their toxicity on gonads in breast cancer as evidenced by the decrease AMH levels after chemotherapy [24,25].
Similar results were also reported by previous studies on breast cancer patients with decreased serum AMH levels in young breast cancer survivors who continued menstruation following chemotherapy when compared with their healthy controls [26]. Studies has also found that women who resumed regular menstrual cycle after chemotherapy may have decreased OR [24,25]. Serum AMH concentrations was decreased in these women after chemotherapeutic drugs administration as compared with their age matched healthy controls [26,27].
Decreased serum AMH levels was seen immediately after the initiation of chemotherapeutic drugs. Hence, AMH seems to be an early and sensitive plasma marker of gonadal damage giving a prediction of chemotherapy related outcomes in these patients. Another study also assayed AMH and other hormonal markers before, during and after chemotherapy administration and reported the decreased serum AMH levels after chemotherapy indicating direct chemotherapy induced damage to the GC and hence growing follicles and ultimately the follicle pool resulting in decreased OR. Higher serum AMH levels in these patients before chemotherapy were predictive of higher levels after chemotherapy [19].
Anderson et al., conducted a study in which different markers of OR like AMH, E2, FSH, inhibin B, AFC were studied in patients who received adjuvant treatment. They observed significantly decreased or undetectable serum AMH levels after chemotherapy similar to other previous studies [28]. Among these markers serum AMH demonstrated its role as an early indicator of chemotherapy-induced ovarian follicle loss. Authors suggested that FSH and AMH concentration measurements would be useful for the comparison of ovarian toxicity of different chemotherapy drugs [29]. Researchers concluded that AMH levels before chemotherapy was a useful predictor of loss of ovarian function following chemotherapy in women with breast cancer [25].
Dillon et al., reported that prechemotherapy serum AMH levels above 2 ng/mL were predictive of better recovery after chemotherapy [30]. In the similar study researchers found that pre-treatment serum AMH concentration was lower in women treated for breast cancer who were amenorrheic one year after chemotherapy, although Yu et al., does not observed such difference in serum AMH levels [28,31].
Women’s who resumed menstruation after adjuvant treatment reported to have decreased fertility and early menopause in later life. The probability of early menopause and infertility in these patients depends on their age at diagnosis, type of cancer and the drug regimen they were given as chemotherapy, being more with alkylating agents [32].
Limitations
The present study has a number of limitations. Firstly, in present study we had collected just single serum sample of AMH only after complete course of chemotherapy. This could be done at more frequent intervals at first, third, sixth and after last cycle of chemotherapy to see the more exact results after chemotherapy administration. It was not performed so frequently because it was not available in our laboratory and is very costly. Second limitation is that ovarian reserve was not measured by other serum and ultrasound markers. AMH correlation with ovarian reserve marker would have broaden our aspects of understanding.
Conclusion
While treating patients with chemotherapy, knowledge of the precise time point by which the OR is depleted is of great importance for the decision regarding the optimal adjuvant hormonal treatment. Presently, data is insufficient to support routine assessment of this biomarker priorto chemotherapy. The results of the present study support the diagnostic value of AMH as a reliable marker of OR in breast cancer patients. Prechemotherapy AMH could be a predictive marker of long term postchemotherapy loss of ovarian function along with previously established individualising predictor, i.e. age. Serum AMH levels before chemotherapy may guide clinicians and women being a valuable marker of OR, which may facilitate reproductive planning in these women and taking decision regarding adjuvant endocrine therapy. Further studies are required to establish the use of this hormone as OR marker in appropriate stages of the disease before, after and up to at least one year after finishing adjuvant chemotherapy.
[1]. Meirow D, Biederman H, Anderson RA, Wallace WH, Toxicity of chemotherapy and radiation on female reproductionClin Obstet Gynecol 2010 53:727-39. [Google Scholar]
[2]. Oktem O, Oktay K, Quantitative assessment of the impact of chemotherapy on ovarian follicle reserve and stromal functionCancer 2007 110:2222-29. [Google Scholar]
[3]. Wallace WH, Kelsey TW, Human ovarian reserve from conception to the menopausePLOS One 2010 5:e8772 [Google Scholar]
[4]. Partridge AH, Ruddy KJ, Gelber S, Ovarian reserve in women who remain premenopausal after chemotherapy for early stage breast cancerFertilSteril 2010 94:638-44. [Google Scholar]
[5]. Aubard Y, Piver P, Pech JC, Galinat S, Teissier MP, Ovarian tissue cryopreservation and gynecologic oncology: a reviewEur J Obstet Gynecol Reprod Biol 2001 97:5-14. [Google Scholar]
[6]. Lee SJ, Schover LR, Partridge AH, Patrizio P, Wallace WH, Hagerty K, American Society of Clinical Oncology. American Society of Clinical Oncology recommendations on fertility preservation in cancer patientsJ Clin Oncol 2006 24:2917-31. [Google Scholar]
[7]. Familiari G, Caggiati A, Nottola SA, Ermini M, Di Benedetto MR, Motta PM, Ultrastructure of human ovarian primordial follicles after combination chemotherapy for Hodgkin’s diseaseHum Reprod 1993 8:2080-87. [Google Scholar]
[8]. Wulff C, Wilson H, Wiegand SJ, Rudge JS, Fraser HM, Prevention of thecal angiogenesis, antral follicular growth, and ovulation in the primate by treatment with vascular endothelial growth factor Trap R1R2Endocrinology 2002 143:2797-807. [Google Scholar]
[9]. Elizur SE, Chian RC, Pineau CA, Son WY, Holzer HEG, Huang JYJ, Fertility preservation treatmentfor young women with autoimmune diseases facing treatment with gonadotoxic agentsRheumatology (Oxford) 2008 47:1506-09. [Google Scholar]
[10]. Iverson A, Younis A, William J, Butler Roudebush WE, Inverse Correspondence of AMH and FSH levels in Women Presenting for Infertility TreatmentJournal of the South Carolina Academy of Science 2011 9(2):1-4. [Google Scholar]
[11]. Tan SL, Royston P, Campbell S, Jacobs HS, Betts J, Mason B, Cumulative conception and live birth rates after in vitro fertilizationLancet 1992 339:1390-94. [Google Scholar]
[12]. Toner JP, Philput CB, Jones JS, Mushaer SJ, Basal follicle-stimulating hormone is a better predictor of in vitro fertilization performance than ageFertilSteril 1991 55(4):784-91. [Google Scholar]
[13]. Lass A, Skull J, McVeigh E, Margara R, Winston RM, Measurement of ovarian volume by transvaginalsonography before ovulation induction with human menopausal gonadotrophin for in-vitro fertilization can predict poor responseHum Reprod 1997 12(2):294-97. [Google Scholar]
[14]. Syrop CH, Willhoite A, Van Voorhis BJ, Ovarian volume: a novel outcome predictor for assisted reproductionFertilSteril 1995 64(6):1167-71. [Google Scholar]
[15]. Nahum R, Shifren JL, Chang Y, Leykin L, Isaacson K, Toth TL, Antral follicle assessment as a tool for predicting outcome in IVF—is it a better predictor than age and FSH?J Assist Reprod Genet 2001 18(3):151-55. [Google Scholar]
[16]. Bancsi LF, Broekmans FJ, Eijkemans MJ, de Jong FH, Habbema JD, teVelde ER, Predictors of poor ovarian response in in vitro fertilization: a prospective study comparing basal markers of ovarian reserveFertilSteril 2002 77(2):328-36. [Google Scholar]
[17]. Massague’ J, The transforming growth factor-b familyAnnual Review of Cell Biology 1990 6:597-641. [Google Scholar]
[18]. Anderson RA, What does anti-Müllerian hormone tell you about ovarian function?Clin Endocrinol 2012 77(5):652-55. [Google Scholar]
[19]. Visser JA, de Jong FH, Laven JS, Themmen AP, Anti-Müllerianhormone: a new marker for ovarian functionReproduction 2006 131(1):1-9. [Google Scholar]
[20]. La Marca A, Stabile G, Artenisio AC, Volpe A, Serum anti-Müllerian hormone throughout the human menstrual cycleHum Reprod 2006 21:3103-07. [Google Scholar]
[21]. Broer SL, Eijkemans MJ, Scheffer GJ, van Rooij IA, de Vet A, Themmen AP, Anti-mullerian hormone predicts menopause: a long-term follow-up study in normoovulatory womenJ Clin Endocrinol Metab 2011 96(8):2532-39. [Google Scholar]
[22]. Lie Fong S, Laven JS, Hakvoort-Cammel FG, Schipper I, Visser JA, Themmen AP, Assessment of ovarian reserve in adult childhood cancer survivors using anti-Müllerian hormoneHum Reprod 2009 24:982-90. [Google Scholar]
[23]. Wallace AM, Faye SA, Fleming R, Nelson SM, A multicentre evaluation of the new Beckman Coulter anti-Mullerian hormone immunoassay (AMH Gen II)Ann Clin Biochem 2011 48:370-73. [Google Scholar]
[24]. Anderson RA, Cameron DA, Pretreatment serum anti-müllerian hormone predicts long-term ovarian function and bone mass after chemotherapy for early breast cancerJ Clin Endocrinol Metab 2011 96(5):1336-43. [Google Scholar]
[25]. Anderson RA, Rosendahl M, Kelsey TW, Cameron DA, Pretreatment anti-Müllerian hormone predicts for loss of ovarian function after chemotherapy for early breast cancerEur J Cancer 2013 49(16):3404-11. [Google Scholar]
[26]. Partridge AH, Ruddy KJ, Gelber S, Schapira L, Abusief M, Meyer M, Ovarian reserve in women who remain premenopausal after chemotherapy for early stage breast cancerFertilSteril 2010 94:638-44. [Google Scholar]
[27]. Su HI, Sammel MD, Green J, Velders L, Gracia CR, Matro J, Anti-mullerian hormone and inhibin B are hormone measures of ovarian function in late reproductive-aged breast cancer survivorsCancer 2010 116:592-99. [Google Scholar]
[28]. Anders C, Marcom PK, Peterson B, Gu L, Unruhe S, Welch R, A pilot study of predictive markers of chemotherapy-related amenorrhea among premenopausal women with early stage breast cancerCancer Invest 2008 26(3):286-95. [Google Scholar]
[29]. Anderson RA, Themmen AP, Al-Qahtani A, Groome NP, Cameron DA, The effects of chemotherapy and long-term gonadotrophin suppression on the ovarian reserve in premenopausal women with breast cancerHum Reprod 2006 21(10):2583-92. [Google Scholar]
[30]. Dillon KE, Sammel MD, Prewitt M, Ginsberg JP, Walker D, Mersereau JE, Pretreatment antimüllerian hormone levels determine rate of posttherapy ovarian reserve recovery: acute changes in ovarian reserve during and after chemotherapyFertilSteril 2013 99(2):477-83. [Google Scholar]
[31]. Yu B, Douglas N, Ferin MJ, Nakhuda GS, Crew K, Lobo RA, Changes in markers of ovarian reserve and endocrine function in young women with breast cancer undergoing adjuvant chemotherapyCancer 2010 116(9):2099-105. [Google Scholar]
[32]. Letourneau JM, Ebbel EE, Katz PP, Oktay KH, McCulloch CE, Ai WZ, Acute ovarian failure underestimates age-specific reproductive impairment for young women undergoing chemotherapy for cancerCancer 2012 118:1933-39. [Google Scholar]