Accuracy of Common Femoral Artery Doppler Waveform Analysis in Predicting Haemodynamically Significant Aortoiliac Lesions
Varsha P. Rangankar1, Kishor B. Taori2, Rajesh G. Mundhada3, Atul D. Rewatkar4
1 Associate Professor, Department of Radiology, Smt. Kashibai Navale Medical College, Pune, India.
2 Professor and Head, Department of Radiology, Government Medical College, Nagpur, India.
3 Consultant, Department of Radiodiagnosis, Pulse Clinic and Hospital, Nagpur, India.
4 Consultant, Department of Radiodiagnosis, Pulse Clinic and Hospital, Nagpur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Varsha P. Rangankar, Associate Professor, Department of Radiology, SKN Medical College and GH, Pune-411 041, India.
E-mail: varsharangankar@gmail.com
Introduction
Doppler ultrasound is cost-effective and accurate noninvasive method for evaluation of peripheral arterial disease. However, there is difficulty in detection of aortoiliac lesions due to inadequate visualization of aortoiliac arteries in many patients. The Doppler waveform changes occurring distal to significant stenosis or occlusion are well documented. Accordingly, common femoral artery (CFA) Doppler waveform analysis may be used to predict haemodynamically significant proximal aortoiliac lesions.
Aim
To evaluate the accuracy of Doppler waveform analysis at the CFA for diagnosing haemodynamically significant aortoiliac stenosis or occlusion in patients of peripheral arterial disease.
Materials and Methods
A total of 67 patients (114 aortoiliac segments) with suspected peripheral arterial disease were retrospectively evaluated and labeled as normal or abnormal by analysing the Doppler waveform of CFA. The triphasic waveform with normal reversal pattern was categorized as normal, while low velocity biphasic or monophasic waveform were labeled as abnormal and indirect diagnosis of normal or diseased (>50% stenosis or occlusion) aortoiliac segment was made. The results were compared to intra-arterial angiography, considered as the gold standard.
Results
The Doppler waveform analysis of CFA was abnormal in 41 out of 114 common femoral arteries, while intra-arterial angiography showed significant stenosis (21 arteries) or occlusion (26 arteries) in 47 (41%) of 114 aortoiliac segments in 67 patients. Out of 67 normal aortoiliac segments seen on angiography, the CFA waveform analysis was interpreted as normal in 62 segments. An abnormal CFA waveform could diagnose significant aortoiliac lesion with 87% sensitivity, 92% specificity, 89% Positive Predictive Value (PPV), 91% Negative Predictive Value (NPV) and 90% accuracy using angiography as the gold standard. The low velocity monophasic waveform which was seen in 38 (33%) of 114 segments was reliable predictor of significant aortoiliac disease with 93% positive predictive value.
Conclusion
CFA Doppler waveform pattern analysis is a sensitive and accurate technique for the prediction of haemodynamically significant aortoiliac stenosis or occlusion.
Monophasic, Stenosis, Occlusion
Introduction
Doppler ultrasound is a noninvasive method used for quick and cost-effective evaluation of peripheral arterial disease. It is used as first line investigation in these patients and has been proven to accurately provide information about peripheral circulation [1–3]. However, there is difficulty in detection of aortoiliac lesions in many patients due to inadequate visualization of aortoiliac arteries. Ramaswami G et al., reported non visualization of 20% aortoiliac segments by color duplex sonography because of factors like obesity, bowel gases, use of higher frequency transducer and severe atherosclerotic disease arterial wall changes and calcification [4]. The Common Femoral Artery (CFA) Doppler waveform analysis may be used in such cases to predict the presence of significant aortoiliac disease and has been reported as an accurate indicator of proximal obstructive disease [5]. The purpose of this study was to evaluate accuracy of CFA Doppler waveform analysis in predicting haemodynamically significant aortoiliac lesions.
Materials and Methods
The patients of peripheral arterial disease investigated with Doppler and angiography in Government Medical College and Hospital, Nagpur during February 2001 and June 2007 were included in this retrospective study. Sixty- seven patients (114 aortoiliac segments) were identified from the database and their Doppler and angiography images were assessed by two separate radiologists. The patients with haemodynamically significant lesions in CFA were excluded from the study. These patients were evaluated by Doppler ultrasound using high resolution, 6-10 MHz linear pulsed wave Doppler transducer. Proper probe position was done to obtain correct spectral waveform and avoid artifacts. The CFA spectral waveforms were analysed and labeled as normal or abnormal. The triphasic waveform with normal reversal pattern and clear spectral window was categorized as normal, while low velocity biphasic or monophasic waveforms were labeled as abnormal and indirect diagnosis of normal or diseased (>50% stenosis or occlusion) aortoiliac segment was made. All patients were subjected to intra-arterial angiography, used as “gold standard”, within five days of Doppler examination. Significant stenosis was diagnosed on angiography when there was arterial diameter reduction of more than 50%, while non contrast filling of artery was diagnosed as occlusion. Normal arterial diameter and mild stenosis were considered as nonsignificant lesions. Doppler and angiographic results were compared and the values for sensitivity, specificity, Positive Predictive Value (PPV), Negative Predictive Value (NPV) and accuracy were calculated. Approval was obtained for the study from institutional ethical committee.
Results
The Doppler waveforms of total 114 common femoral arteries in 67 patients of peripheral arterial disease in the age group of 41 to 70 years were retrospectively evaluated. Spectral Doppler waveforms were classified into normal triphasic pattern and abnormal biphasic or monophasic pattern [Table/Fig-1]. In presence of abnormal CFA waveform, indirect diagnosis of diseased (>50% stenosis or occlusion) aortoiliac segment was made. The intra-arterial angiography images of all patients were analysed and results were compared to Doppler analysis interpretation [Table/Fig-2]. Angiography demonstrated 47 abnormal aortoiliac arteries with significant stenosis seen in 21 (55%) and occlusion in 26 (55%) segments. Out of these, 41 (87%) segments showed abnormal monophasic or biphasic Doppler waveforms and 6 had normal triphasic waveform. Angiography revealed 67 normal aortoiliac segments out of which 62 (92%) had normal triphasic waveform and 5 had abnormal waveforms. An abnormal CFA waveform could diagnose significant aortoiliac lesion with 87% sensitivity, 92% specificity, 89% Positive Predictive Value (PPV), 91% Negative Predictive Value (NPV) and 90% accuracy using angiography as the gold standard. The low velocity monophasic waveform was seen in 38 (33%) of 114 segments and was reliable predictor of significant aortoiliac disease with positive predictive value of 93%.
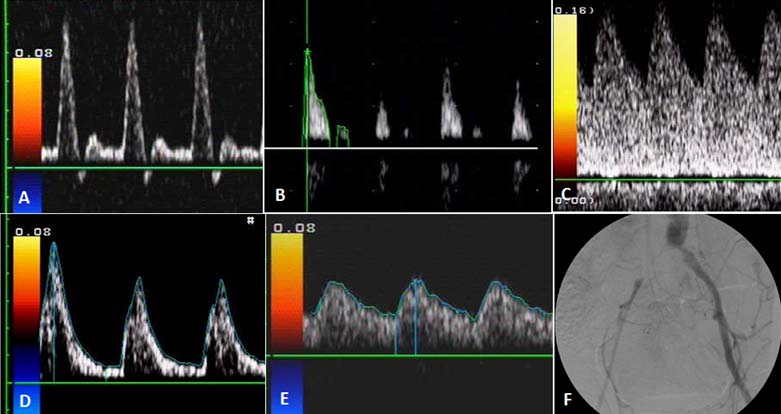
Common Femoral Artery (CFA) waveform patterns (a-e): a) Normal triphasic waveform of CFA with diastolic flow reversal and clear spectral window; b) Abnormal biphasic waveform with loss of flow reversal; c) Monophasic waveform with loss of reversal and increased diastolic flow. Both these patients (b,c) had significant stenosis of CFA on angiography; d) Monophasic waveform with sharp systolic peaks and continuous diastolic flow; e) Monophasic parvus tardus flow pattern. Angiography revealed occlusion of common iliac arteries (CIA) in these patients (d,e). f) Digital subtraction angiography image showing occlusion of right CIA and stenosis of left CIA.
Results of CFA waveform analysis versus angiography in detection of significant aortoiliac lesions.
| CFA waveform/Significant aortoiliac lesion | Aortoiliac lesion | Total |
|---|
| Present | Absent |
|---|
| CFA waveform | Abnormal | 41 | 05 | 46 |
| Normal | 06 | 62 | 68 |
| Total | 47 | 67 | 114 |
Discussion
Peripheral arterial disease (PAD), especially the advanced stage of critical limb ischemia, is an emerging, severe and often underdiagnosed disease with limited knowledge about the prognosis and optimal treatment [6]. Peripheral arterial diseases have many aetiologies and are variable in location, presentation and severity. The ankle brachial index (ABI) can be used as screening test to establish the diagnosis and severity of PAD [7]. Duplex ultrasonography allows assessment of the vessel wall and plaque morphology and is helpful in further defining the location and degree of stenosis or occlusion [7,8]. The efficacy of Doppler ultrasound in the evaluation of PAD has improved over the period and the results are comparable to angiography which is often used as gold standard [1–4]. Imaging of aortoiliac segments is very important in complete assessment and treatment planning of patients of PAD. However, due to deep anatomical location and tortuous course of aortoiliac segments, their Doppler examination is often difficult and time consuming. It is further hindered by other factors like artifacts, bowel gases, patient obesity and movement, use of higher frequency transducer and severe atherosclerotic disease arterial wall changes and calcification [4]. The Doppler evaluation of CFA which is easier to access and assess have been proposed for prediction of proximal aortoiliac disease by many authors [9–13]. A normal CFA waveform is triphasic with normal reversal pattern and clear spectral window, while the waveform distal to a significant stenosis or occlusion often becomes biphasic or monophasic with reduced velocities and can be indicative of significant proximal aortoiliac lesion. A monophasic and dampened signal can be obtained proximal as well as distal to occlusion. Just distal to stenosis, Doppler waveform shows dampened systolic component and absent diastolic flow but it is not as high amplitude as the stenotic signal. The waveform distal to occlusion is similar to poststenotic signal, with even lower amplitude systolic component. There similar abnormal waveforms are difficult to interpret and is either labeled as normal or abnormal in routine practice [14]. Quantitative interpretation of Doppler waveform has also been evaluated for assessment of significant proximal aorto-iliac disease using measurement of pulsatility index (PI) and acceleration time at CFA [14,15]. Normal PI value of 5.5 is seen in CFA and its reduction (PI of 4/5) indicates proximal aortoiliac occlusive disease. Acceleration time which is duration of upstroke from end-diastole to peak systole is prolonged the site of the Doppler interrogation in presence of proximal arterial obstruction.
The results in our study suggested that abnormal CFA waveform could diagnose significant aortoiliac lesion with 87% sensitivity, 92% specificity, 89% positive predictive value (PPV), 91% negative predictive value (NPV) and 90% accuracy using angiography as the gold standard. These results are comparable to the study by Cossman DV et al., who found sensitivity, specificity and kappa value of 81%, 98% and 0.82, respectively for diagnosis of iliac disease by common femoral waveform analysis against conventional arteriography [10]. In a similar study, Sensier Y et al., found that visual interpretation of the common femoral Doppler waveform had sensitivity, specificity and accuracy of 95%, 80% and 87% respectively for the prediction of significant aortoiliac stenosis [11]. Eiberg JP et al., reported sensitivity, specificity, PPV and NPV of 98%, 81%, 86% and 97% respectively for visual interpretation of CFA Doppler waveform in prediction of significant aortoiliac occlusive disease compared to conventional arteriography [12]. The low velocity monophasic waveform was seen in 38 (33%) of 114 segments and was decisive predictor of significant aortoiliac disease with positive predictive value of 93%. Spronk S et al., in their study concluded that presence of a poor monophasic waveform in CFA with a positive predictive value of 92% was a reliable sign of significant aortoiliac disease [5]. O’Neill S compared CFA Doppler waveforms and MR angiography for diagnosing aortoiliac stenosis and fount that monophasic waveforms alone were more specific (88%) but less sensitive (57%) for predicting iliac lesions [13]. Normal CFA waveform showed negative predictive value of 91% for exclusion of significant proximal aortoiliac lesions underlining its significance as timesaving and cost effective screening technique. The false negative cases in our study had short segment stenosis of proximal common iliac artery. It has been reported by some authors that Doppler waveform can become normal at sufficient distance distal to the stenosis [11,16]. The false positive cases with abnormal CFA waveform [Table/Fig-3] had proximal occlusion of superficial femoral artery (SFA) out of which proximal profunda femoris stenosis was also seen in two patients. Similar findings of abnormal CFA waveform in cases of SFA occlusion have been previously reported in the literature [17,18].
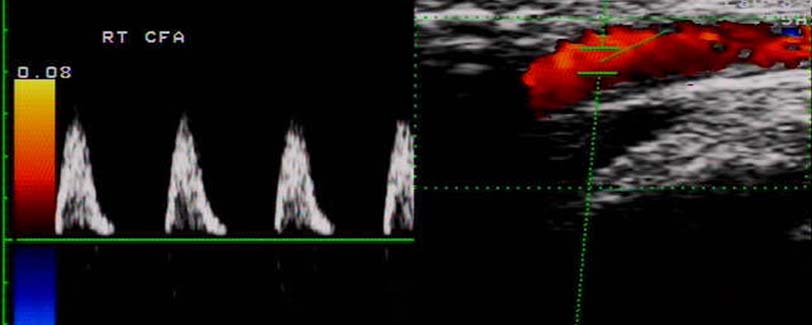
Abnormal CFA waveform showing systolic peaks with absence of flow reversal and diastolic flow. Angiography revealed normal aortoiliac arteries with occlsuion in superficial femoral artery.
Conclusion
In conclusion, qualitative evaluation of the common femoral Doppler waveform is a sensitive and accurate technique for the prediction of significant aortoiliac stenosis. Also, normal CFA Doppler waveform can safely exclude significant upstream aortoiliac lesions. Analysis of CFA is cost effective and easy to perform and is of particular value when full aortoiliac assessment is not feasible due to time, technique and patient related limiting factors.
[1]. Jager KA, Phillips DJ, Martin RL, Hanson C, Roederer GO, Langlois YE, Noninvasive mapping of lower limb arterial lesionsUltrasound Med Biol 1985 11:515-21. [Google Scholar]
[2]. Kohler TR, Nance DR, Cramer MM, Vandenburghe N, Strandness DE, Duplex scanning for diagnosis of aortoiliac and femoropopliteal disease: a prospective studyCirculation 1987 76(5):1074-80. [Google Scholar]
[3]. Aly S, Sommerville K, Adiseshiah M, Raphael M, Coleridge Smith PD, Bishop CC, Comparison of duplex imaging and arteriography in the evaluation of lower limb arteriesBr J Surg 1998 85(8):1099-102. [Google Scholar]
[4]. Ramaswami G, Al-Kutoubi A, Nicolaides AN, Dhanjil S, Griffin M, Belcaro G, The role of duplex scanning in the diagnosis of lower limb arterial diseaseAnn Vasc Surg 1999 13(5):494-500. [Google Scholar]
[5]. Spronk S, den Hoed PT, de Jonge LC, van Dijk LC, Pattynama PM, Value of the duplex waveform at the common femoral artery for diagnosing obstructive aortoiliac diseaseJ Vasc Surg 2005 42(2):236-42. [Google Scholar]
[6]. Reinecke H, Unrath M, Freisinger E, Bunzemeier H, Meyborg M, Lüders F, Peripheral arterial disease and critical limb ischaemia: still poor outcomes and lack of guideline adherenceEur Heart J 2015 36(15):932-38. [Google Scholar]
[7]. Wennberg PW, Approach to the patient with peripheral arterial diseaseCirculation 2013 128(20):2241-50. [Google Scholar]
[8]. Azam SM, Carman TL, Diagnostic approach to peripheral arterial diseaseCardiol Clin 2011 29(3):319-29. [Google Scholar]
[9]. Nicolaides AN, Gordon-Smith IC, Dayandas J, Eastcott HH, The value of Doppler blood velocity tracings in the detection of aortoiliac disease in patients with intermittent claudicationSurgery 1976 80(6):774-78. [Google Scholar]
[10]. Cossman DV, Ellison JE, Wagner WH, Comparison of contrast arteriography to arterial mapping with color-flow duplex imaging in the lower extremitiesJ Vasc Surg 1989 10(5):522-28.discussion 528-29 [Google Scholar]
[11]. Sensier Y, Bell PR, London NJ, The ability of qualitative assessment of the common femoral Doppler waveform to screen for significant aortoiliac diseaseEur J Vasc Endovasc Surg 1998 15(4):357-64. [Google Scholar]
[12]. Eiberg JP, Jensen F, Gronvall Rasmussen JB, Schroeder TV, Screening for aortoiliac lesions by visual interpretation of the common femoral Doppler waveformEur J Vasc Endovasc Surg 2001 22(4):331-36. [Google Scholar]
[13]. O’Neill S, George RK, Wallace WD, Blair PH, McKinley A, Do Doppler waveforms at the common femoral artery accurately predict iliac stenosis?Ir J Med Sci 2011 180(1):247-49. [Google Scholar]
[14]. AbuRahma A, Bandyk D, Noninvasive Vascular Diagnosis: A Practical Guide to Therapy 2013 3rd edPublisher- SpringerCh 19. Pg. 233- 234 [Google Scholar]
[15]. Cronenwett JL, Johnston KW, Rutherford’s Vascular Surgery 2014 8th EdPublished by SaundersSection 3 - Ch15. Pg. 215-217 [Google Scholar]
[16]. Evans DH, Macpherson DS, Asher MJ, Bentley S, Bell PR, Changes in Doppler ultrasound sonograms at varying distances from stenosesCardiovasc Res 1982 16:631-36. [Google Scholar]
[17]. Peripheral vascular ultrasound. How, why and when, 2nd ed., A. Thrush, T. Hartshorne. Elsevier (2005). Chapter -9. Page 128-129 [Google Scholar]
[18]. Rosfors S, Eriksson M, Hoglund N, Johansson G, Duplex ultrasound in patients with suspected aortoiliac occlusive diseaseEur J Vasc Surg 1993 7(5):513-17. [Google Scholar]