The global burden of TB in the world is estimated to be 9.3 million out of which India contributes 2.6 million [1]. India bears the third largest burden of HIV-TB due to high TB infections in HIV individuals [2]. The diagnosis of pulmonary TB is based on clinical signs and symptoms along with laboratory tools such as sputum microscopy, culture and radiography. Extrapulmonary TB, depending on the site of involvement usually requires additional diagnostic tools such as fine needle aspiration cytology (FNAC) of the suspected tissues, biopsy, culture and imaging (Ultrasound/CT/MRI). The diagnosis of TB in HIV co-infected individuals continues to be a challenge, with sensitivity ranging from 33.7% to 74.4% in various serological tests [3,4]. Various Mycobacterium tuberculosis (M.tb) antigens have been well characterized and have been used in TB detection assays [5–7] and there is ongoing research on multiple antigen based serological assays [8–10]. World Health Organization (WHO) recommends further targeted research on serological tests for TB detection [11] keeping in view the simplicity, feasibility and cost effectiveness of serological tests. The present study measured the antibody response to 38kDa, LAM and ESAT-6, in patients with TB and HIV-TB co-infection and also evaluated the sensitivity of TB detection using multiple ELISA tests. This study was carried out in view of the significant morbidity and mortality of TB per se as well as among a sizable proportion of HIV co-infected individuals in India as well as its wider application to other countries endemic for TB [12]. The 38kDa protein of M.tb is a phosphate binding protein that produces B and T cell responses that are highly specific to TB [13–16]. Lipoarabinomannan (LAM) is a glycolipid that induces mycobacteria specific immune responses [17]. Early secretory antigenic target-6 (ESAT-6) is a 6kDa protein of M.tb and is a potent immunogen [18].
Materials and Methods
Study setting and Ethics: Patients were recruited from the outpatient clinic of Nireekshana ACET and the Government Chest Hospital, Hyderabad, India. The study was approved by the institutional ethics committee of Nireekshana ACET. Informed consent was obtained from the subjects prior to their participation in the study. Blood was collected from the patients before starting treatment.
Diagnosis of TB: Pulmonary TB (PTB) was bacteriologically confirmed by sputum smear positivity, and or chest X-ray positivity, and clinical examination. Extrapulmonary TB (ETB) patient detection and categorization was as per guidelines by the Governmental Revised National Tuberculosis Control Programme (RNTCP) [19]. ETB included patients with one or two organ sites of the body infected without lung involvement. Individuals with clinical symptoms of ETB underwent the following routine diagnostic tests; sputum microscopy, culture for certain cases (according to RNTCP), chest X-ray, fine needle aspiration cytology (FNAC) of the suspected tissues, biopsy and imaging (CT/MRI). Subjects were included in the study if they were positive by one or more of the diagnostic tests.
Diagnosis of HIV: HIV-1 status was confirmed by three immunoassays according to the National Integrated Counseling and Testing Programme by National AIDS Control Organization (NACO) India, after appropriate pretest counseling. These include two enzyme immunoassays (EIA and Comb AIDS-RS, Span Diagnostics, India) and one spot test (HIV TRI-DOT, J. Mitra & Co, India) for 3 different HIV specific antigens according to NACO [20]. All the study subjects included in the study were screened for HIV.
The study subjects are described in detail below: HIV-TB co-infected subjects (HIV-TB): This group had a total number of 124 HIV-TB subjects, sub grouped into HIV-Pulmonary TB (HIV-PTB) and HIV-extrapulmonary TB (HIV-ETB). HIV-PTB included 62 seropositive individuals (Males 46, Females 16) who were co-infected with pulmonary tuberculosis, with a median age of 32 years. Of the 62 patients, 39 were sputum positive and 23 were confirmed by chest X-ray and clinical examination. The mean CD4 count of patients in this subgroup was 251±137 cells/ mm3.
The HIV extrapulmonary TB (HIV-ETB) included 62 seropositive individuals (48 males and 14 females) who were co-infected with extrapulmonary tuberculosis, with a median age of 33 years. HIV-ETB included patients with TB lymphadenitis (n=26), pleural effusions (n=17), abdominal TB (n=7), cervical & lingual TB (n=7), miliary TB (n=3), TB spine (n=1) and meningial TB (n=1). The mean CD4 count of patients in this subgroup was 237±130 cells/ mm3.
Tuberculosis subjects (TB): This group included 39 individuals with TB (25 males and 14 females) with a median age of 31 years. There were 27 PTB patients and 12 ETB patients. All the TB subjects of this study were also screened for HIV as a cross referral mandatory test after appropriate pre-test counseling and were seronegative [19,20].
HIV seropositive subjects (HIV): This group consisted of 56 individuals (34 males; 22 females) with a median age of 33 years. Their mean CD4 count was 421±165 cells/ mm3. These patients had no signs or symptoms suggestive of TB and were followed up for one year with no clinical manifestation of TB.
Healthy subjects (HS): A total of 57 HS (31 males and 26 females) with a median age of 39 years were recruited from the Nizam’s Institute of Medical Sciences Blood Bank, Hyderabad. The subjects were apparently normal and without any clinical symptoms. They were screened for HIV and other blood borne infections which are listed as mandatory by the National Blood Transfusion guidelines criteria and were found to be negative. A questionnaire on TB and other chronic illness were part of the screening programme for blood donation and those without any of the mentioned problems were considered healthy blood donors [20].
Enzyme Linked Immunosorbent Assays (ELISAs): ELISAs were performed using Pathozymemyco kits and were referred to as ELISA I, II, III and an additional ESAT-6 ELISA was referred to ELISA IV for clarity.
ELISA-I, II and III for 38kDa-LAM: Serum IgG, IgM and IgA antibodies to 38kDa plus native LAM from M. tb was coated on an ELISA plate as a combined antigens in the kit [21,22]. The three ELISAs were numbered ELISA I-IgG antibody response to 38kDa-LAM; ELISA II - IgM antibody response to 38kDa-LAM and ELISA III - IgA antibody response to 38kDa-LAM. Briefly, antigen coated plates were dispensed with 100ul of 1:100 diluted patient serum and incubated for 1hr at 37°C; followed by 30 minutes incubation with conjugated secondary antibody at 37°C; and followed by incubation with substrate. Each step was interspersed with 5 cycle wash with wash buffer using Bio-Rad ELISA washer except for the final step of termination with stop solution. The colour developed was measured at 450 nm using a Bio-Rad microplate reader.
ELISA-IV for ESAT-6: Purified recombinant ESAT-6 was obtained from Colorado State University, USA through a TB research materials and vaccine testing contract (Gift from Dr. John S. Spencer, Colourado State University). Indirect ELISA was performed for ESAT-6 by coating 400ng per well on a Nunc ELISA plate (Cat # 167008) and incubated overnight. Unbound ESAT-6 antigen was removed and blocked with 20mM phosphate buffer saline pH 7.4 containing 2% BSA. The blocking step was followed by five wash cycles with 300ul of wash buffer. Then 100μl of diluted (1/100) serum samples were added to the wells and incubated for 60 min at 20-30°C. This step was followed by five wash cycles using Bio-Rad washer. The wells were subsequently incubated with a mix of 100μl of anti-human IgG, IgA and IgM horse radish peroxidase conjugate for 30 min at 26°C. After another wash cycle, 100μl of 3, 3’, 5, 5’-tetramethylbenzidine (TMB) containing 0.6% hydrogen peroxide was added to the wells and the colourimetric reaction was placed for 15 min in the dark at 26°C. The reaction was terminated by 100μl of 3N sulphuric acid and the colour was read at an absorbance of 450 nm using a Bio-Rad microplate reader.
Statistical Analysis
Individual optical densities (OD) obtained from the samples of each group were recorded and compared by one way ANOVA using SPSS 16. For ELISA I, II and III cut off values (according to manufacturer’s instructions) were used to detect seropositivity. For ELISA IV, mean OD plus one standard deviation value of HS was used as cut off to detect seropositivity. The sensitivity and specificity of the assay was calculated as described by Toman in 1981[23]. All the four ELISA results of various subject groups tested were entered in an excel sheet to evaluate the value of any single or multiple ELISA seropositivities to ascertain sensitivities and specificities for TB detection.
Results
Antibody response to TB antigens by ELISAs: The antibody responses to TB antigens were evaluated by ELISA I, II, III and IV measuring IgG, IgM, IgA antibodies to 38kDa-LAM and ESAT-6 and the O.D values are presented in a scatter gram [Table/Fig-1].
Scattergram of the optical densities (OD) obtained with IgG, IgM, IgA for 38kDa, LAM and ESAT-6 in HS, HIV, TB, HIV-PTB, HIV-ETB groups.
The scattergram shows statistical means of each isotype (IgG, IgM, IgA and ESAT-6). There was significant increase (p<0.05) in TB, HIV-PTB, HIV-ETB groups as compared to HS or HIV infected group.
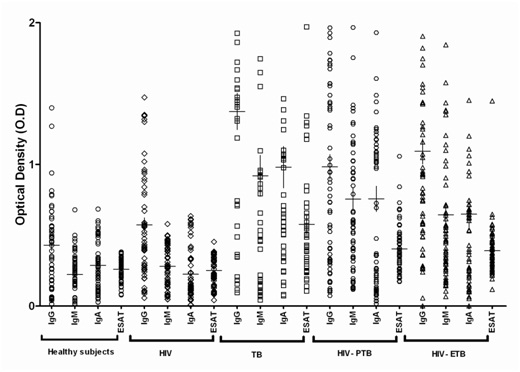
The antibody levels in ELISA-I were significantly elevated (p<0.05) in HIV-TB {HIV-PTB (1.03±0.62) and HIV-ETB (1.09±0.69)} and TB with mean ± SDs (1.12±0.72), as compared to HS (0.42±0.30) or HIV infected group (0.56±0.36). Similarly, antibody levels in ELISA-II were significantly elevated (p<0.05) in HIV-TB {HIV-PTB (0.69±0.4) and HIV-ETB (0.64±0.53)} and TB with mean ± SDs (0.74±0.40), as compared to HS (0.22±0.15) or HIV infected group (0.29±0.14). ELISA-III levels were significantly elevated (p<0.05) in HIV-TB {HIV-PTB (0.67±0.35) and HIV-ETB (0.64±0.42)} and TB with mean ± SDs (0.79±0.69), as compared to HS (0.28±0.18) or HIV infected group (0.25±0.16). ELISA-IV levels were significantly elevated (p<0.05) in HIV-TB {HIV-PTB (0.39±0.17) and HIV-ETB (0.39±0.17)} and TB with mean ± SDs (0.57±0.40), as compared to HS (0.25±0.08) or HIV infected group (0.25±0.10) [Table/Fig-1]. There was no significant difference between HIV-TB and TB antibody levels (p>0.05) for all four ELISAs.
Sensitivity and Specificity of ELISAs: The sensitivities and specificities of ELISA I, II, III and IV for HIV-TB and TB groups are summarized in [Table/Fig-2]. The higher sensitivity was seen with ELISA-I in HIV-TB (72%) and TB group (64%) and the lowest with ELISA-II (39% in HIV-TB; 41% in TB). Further when HIV-TB infected individuals were categorized into HIV-PTB and HIV-ETB the tests showed a small range of sensitivity of 74% and 69% for ELISA-I; 41% and 35% for ELISA-II; 50% and 47% for ELISA-III and 62% and 60% for ELISA-IV respectively. The specificities ranged from 79% for ELISA-I to 96% for ELISA-III.
Sensitivity and Specificity of ELISAs in TB and HIV-TB groups.
| ELISA | Sensitivity | Specificity |
|---|
| HIV-TB (n=124) | TB (n=39) | HIV (n=56) | HS* (n=57) |
|---|
| I | 89(72%) | 25(64%) | 19(33%) | 45(79%) |
| II | 48(39%) | 16(41%) | 3(5%) | 54(95%) |
| III | 61(49%) | 20(51%) | 5(9%) | 55(96%) |
| IV | 76(61%) | 23(59%) | 16(28%) | 53(93%) |
HIV-TB (n=124 of which HIV-PTB is 62, HIV-ETB is 62) and TB (n=39), HIV (n=56), HS (n=57). True positive values with sensitivities are presented in parenthesis for HIV-TB, TB & HIV subjects.* True negative value with specificities is presented in parenthesis for HS.
TB seropositivity by any single or multiple ELISAs: All the four ELISA results of the study subjects tested were studied to evaluate the value of any single or multiple ELISA seropositivity for TB detection [Table/Fig-3]. The highest sensitivity of 93% was observed in any one of the four ELISA’s positives. This was followed by 87% sensitivity in the TB group.
TB seropositivity by any single or multiple ELISAs in TB and HIV-TB subjects.
| Subjects | ELISA Sensitivity |
|---|
| Any 1 | Any 2 | Any 3 | Any 4 |
|---|
| HIV-TB (n=124) | 116(93%) | 88(71%) | 53(43%) | 18(14%) |
| TB(n=39) | 34(87%) | 28(71%) | 17(44%) | 5(13%) |
| HIV(n=56) | 31(55%) | 11(19%) | 1(1.7%) | 0(0%) |
| HS (n=57)* | 40(70%) | 54(95%) | 56(98%) | 57(100%) |
HIV-TB (n=124 of which HIV-PTB is 62, HIV-ETB is 62) and TB (n=39), HIV (n=56), HS (n=57). True positive values with sensitivities are presented in parenthesis for HIV-TB, TB & HIV subjects.* True negative value with specificities is presented in parenthesis for HS.
When HIV-TB was further categorized into HIV-PTB and HIV-ETB any single ELISA showed a small range of sensitivity of 93% and 90%; any two ELISAs 74% and 71%; any three ELISAs 47% and 39% and for all four seropositive ELISAs 15% and 13% respectively. For HS, the true negative value is given in the [Table/Fig-3] with specificity in parenthesis.
Discussion
The major factor influencing the control of TB is early diagnosis and treatment. Conventionally, the diagnosis of TB is based on clinical history, physical examination, chest radiograph and sputum microscopy. In addition to basic investigations, a number of additional tests have been developed which range from simple tuberculin skin test to more advanced tests such as rapid culture (BACTEC and Microscopic Observation Drug-Susceptibility Assay (MODS) [24]; TB polymerase chain reaction (PCR); Xpert MTB/RIF) [25] and Interferon gamma release assays (IGRAs) have been developed for the diagnosis of TB and HIV-TB [26,27]. These tests are useful, however cost per test are high and skill and training are needed [28] which can be overcome by multiple antigen and antibody tests. Additionally, the costing of basic and alternative tests has been compared in the global scenario and is in the range of 3.2 to 20 USD/test [29,30]. In the present study all the four ELISAs together were found to be cost effective at about 15 USD per set of test and are in affordable range in resource limited settings.
The present study used the TB ELISA tests to detect TB in HIV co-infected individuals and in individuals with active TB [13–18]. Several serological tests have been researched on to improve sensitivity of TB diagnosis [31–34]. An earlier study with secretory protein antigens or extracellular proteins of M.tb which included a combination of 38kDa, LAM, 6kDa have shown greater sensitivity and specificity as compared to independent antigen ELISAs in TB [8]. In the present study, the antibody responses did not show any significant difference between HIV-TB and TB patients [Table/Fig-1] and this could be attributed to the integrity of humoral response in HIV infection in spite of decreased cell mediated immunity [35,36]. Significantly elevated antibody levels in HIV-TB (PTB and ETB) and TB emphasizes the importance of ELISAs as an adjunct test along with gold standard diagnostic tests especially in HIV-TB. The antibody response was similar in pulmonary and extrapulmonary tuberculosis suggesting that HIV-TB can be considered as a single entity for ELISA tests.
Among ELISAs, the most frequently used antigens are 38kDa & LAM (IgG, IgA, and IgM) and their sensitivities range from 10% to 85% and specificity from 90% to 100% as published earlier [5]. In our study, sensitivity and specificity of these ELISAs in HIV-TB and TB was in the similar range as reported earlier [37–39].
Earlier studies on combination of antibodies IgG+IgM, IgG+IgA and IgM+IgA showed an increase in sensitivity ranging from 49-63% and specificity of 91-98%. The IgG+IgM+IgA antibody combination has shown a 68% sensitivity and 91% specificity [38,39]. These observations suggest a combination of antigens and antibodies could increase sensitivity and specificity of TB diagnosis. We also observe IgG, IgM and IgA immune responses in an individual infected with M.tb and combination could be considered for TB detection [40].
Individually, ELISA I, II, III and IV showed a limited sensitivity of 72%, 39%, 49% and 61% in HIV-TB [Table/Fig-2]. However, when any single ELISA seropositivity was considered (out of four ELISA tests) the sensitivity increased in HIV-TB to 92% (93% HIV-PTB & 90% HIV-ETB) with a specificity of 70% suggesting that it can be considered for screening tests in HIV-TB. The best optimized sensitivity and specificity was when two out of the four ELISAs were positive. The sensitivity was 72% in HIV-TB (74% in HIV-PTB, 71% in HIV-ETB), 71% in TB and with a specificity of 95% [Table/Fig-3]. When a combination of any three or four ELISA positivity was considered for TB detection, there was a decrease in sensitivity to 44% and 14% respectively but an increase of specificity to 98% and 100% [Table/Fig-3]. Based on the specificities observed in our study, it could be deduced: When four ELISAs are positive (specificity 100%) in a patient-confirmed TB; when three ELISAs are positive (specificity 98%) – probably TB; when two ELISAs are positive (specificity 95%) – possibly TB and When one ELISA is positive (specificity 70%) – suspicion of TB. In endemic areas, resource limited settings and in an individual case management scenario, multiple TB ELISAs could be considered for TB detection.
The sensitivity of the present study was in the similar range of earlier studies with 74% in HIV-PTB, and 71% in HIV-ETB and specificity of 95%. Earlier studies on ELISA tests in HIV-TB co-infection showed that 38-kDa+ LAM +16-kDa has a sensitivity of 80% and a specificity of 87% [41]. With38-kDa+CFP-10 the sensitivity was 59.3% with a specificity of 94% in HIV-TB subjects [9]. Tiwari et al., used a cocktail of four antigens (6, 27, 30 and 38 kDa) and found the sensitivity to be as high as 99% and a specificity of 100% in HIV-PTB patients [8]. Further research needs to be carried out to optimize the use of multiple ELISAs for HIV-PTB and HIV-ETB detection. There was also no significant difference in the CD4 counts between HIV-PTB and HIV-ETB suggesting that the decrease of CD4+ cell counts observed in either forms of HIV-TB does not affect TB detection and these can be used in both forms of TB.
The present study used well characterized antigens, 38kDa, LAM and ESAT-6 for HIV-TB detection by ELISA and supports an earlier evidence of increased sensitivities and specificities of TB detection [8,34]. An optimized combination of other TB antigens like cord factor, an 88-kDa antigen (MTB81) with potential early diagnosis in HIV-TB as an additional test should be further evaluated for multiple ELISAs in HIV-TB [25]. Further studies on newer M.tb antigen combinations could help identify tests with high specificity and sensitivity.
Conclusion
The early diagnosis of tuberculosis and TB in HIV co-infection continues to be a priority. The detection of extrapulmonary TB is a diagnostic challenge. There is a continuing need to identify cost effective, sensitive and specific point of care serological tests for TB. The present study establishes the value of combining two or more M.tb antigen based ELISAs to enhance the sensitivity and specificity of TB detection in patients with tuberculosis as well as in those co-infected with HIV.
HIV-TB (n=124 of which HIV-PTB is 62, HIV-ETB is 62) and TB (n=39), HIV (n=56), HS (n=57). True positive values with sensitivities are presented in parenthesis for HIV-TB, TB & HIV subjects.* True negative value with specificities is presented in parenthesis for HS.
HIV-TB (n=124 of which HIV-PTB is 62, HIV-ETB is 62) and TB (n=39), HIV (n=56), HS (n=57). True positive values with sensitivities are presented in parenthesis for HIV-TB, TB & HIV subjects.* True negative value with specificities is presented in parenthesis for HS.