A Rare and Extensive Case of Oral Malignant Melanoma involving Mandibular Gingiva
Rajendrasinh S Rathore1, Rashmi GS Phulari2, Dharmesh G Vasavada3, Dipen K Patel4
1 Professor and Head of Department, Department of Oral Pathology, Manubhai Patel Dental College & Hospital, Vadodara, Gujarat, India.
2 Professor, Department of Oral Pathology, Manubhai Patel Dental College & Hospital, Vadodara, Gujarat, India.
3 Senior Lecturer, Department of Oral Pathology, Manubhai Patel Dental College & Hospital, Vadodara, Gujarat, India.
4 Senior Lecturer, Department of Oral Pathology, Manubhai Patel Dental College & Hospital, Vadodara, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rashmi GS Phulari, II, 15 Sri Hari Residency, Behind GERI Compound, Gotri Road, Gotri, Vadodara-390021, Gujarat, India. E-mail : rashugs@rediffmail.com
Oral malignant melanoma is an infrequent but an aggressive neoplasm of unknown etiology, seen most commonly in middle age male patients and is more frequently seen at the hard palate and gingiva. The tumor tends to metastasize or locally invade tissue more readily than other malignant tumors in the oral region. In this article, we report a rare case of extensive oral melanoma in a 55-year-old male patient, with a chief complaint of painless growth in mandibular anterior gingiva measuring about 2.6 X 1.7 X 0.8 cm and extending bilaterally till posterior mandibular gingiva and unilaterally to right buccal mucosa. The most common site being hard palate and maxillary gingiva, it is extremely rare in mandibular gingiva (less than 7%) and hence, this rare occurrence in mandibular gingiva is reported, the diagnosis of which was confirmed by histopathology and immunohistochemistry.
HMB-45, Melanocytes, Nodular malignant melanoma
Case Report
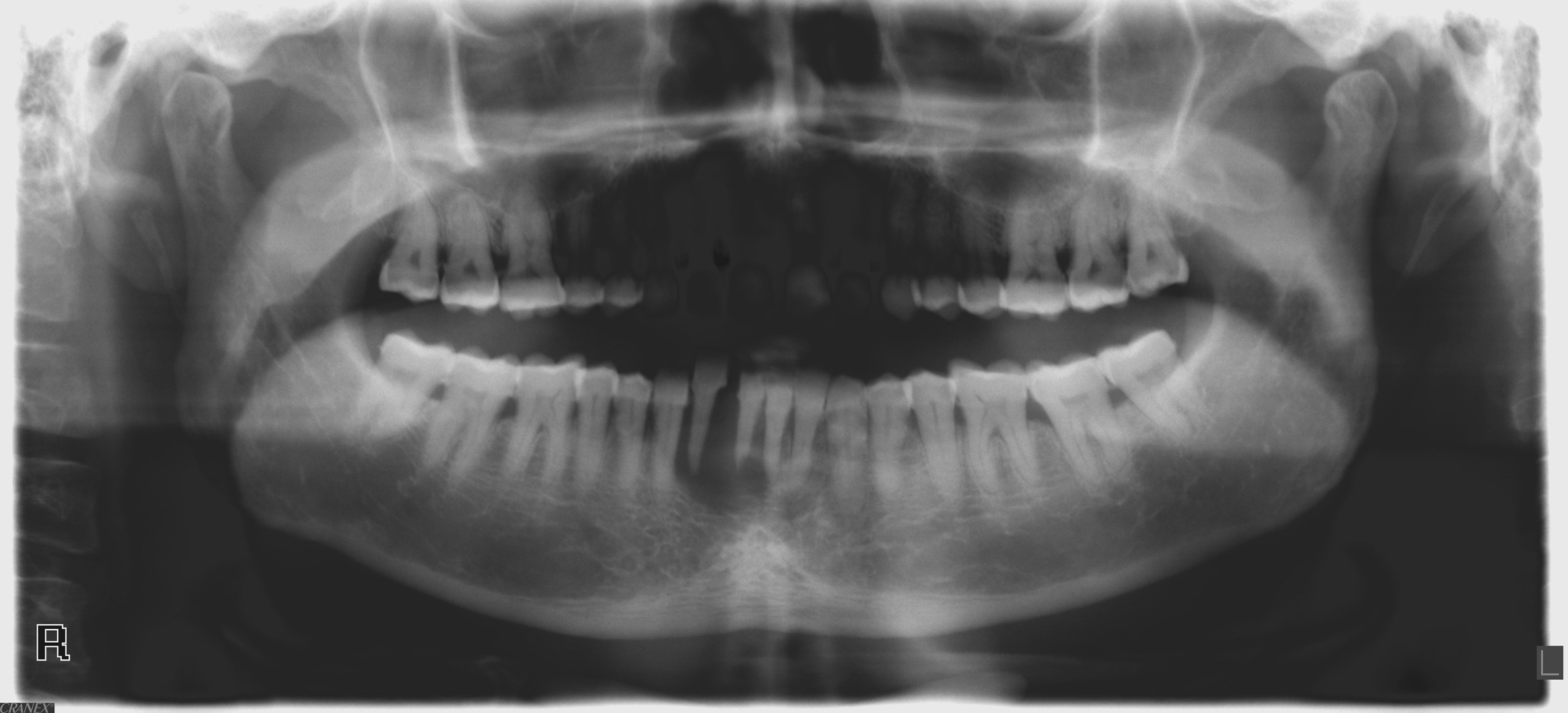
A 55-year-old male patient was referred to the Department of Oral Pathology, Manubhai Patel Dental College and Hospital and Oral Research Institute, Vadodara, Gujarat, India with a chief complaint of painless growth in the mandibular anterior gingival region since four months. Patient’s medical and dental history was noncontributory. Intraoral examination showed an ovoid pigmented growth on the labial gingiva of mandibular anterior region, soft in consistency, grayish black in colour, measuring about 2.6 X 1.7 X 0.8cm. It was sessile, lobulated extending superiorly to the middle third of mandibular central incisors, inferiorly upto the labial vestibule, covering the labial mucosa and extending upto the buccal mucosa in right third molar region. The growth extended to the lingual aspect of mandibular anterior gingival region which was grayish black in colour, soft in consistency measuring about 4.1 X 1.7 X 1.2 cm extending from distal aspect of left mandibular lateral incisor to distal aspect of right lesion was seen covering the mandibular first premolar. The pigmented lesion was seen covering the mandibular marginal gingiva both buccally and lingually and buccal vestibule of the right side extending till the retromolar area [Table/Fig-1,2,3 and 4]. Orthopantomogram showed bone loss in relation to mandibular anterior region [Table/Fig-5].
Clinical Image showing the brownish black growth on buccal and lingual mandibular gingiva.

Clinical Image showing pigmented growth on the anterior mandiblular gingiva and its extension into labial and buccal mucosa.

Clinical Image showing extension of the lesion into the right buccal vestibule.

Clinical image showing extension of the lesion into the left mandibular gingiva.

Orthopantomogram showing bone loss in relation to mandibular anterior teeth.
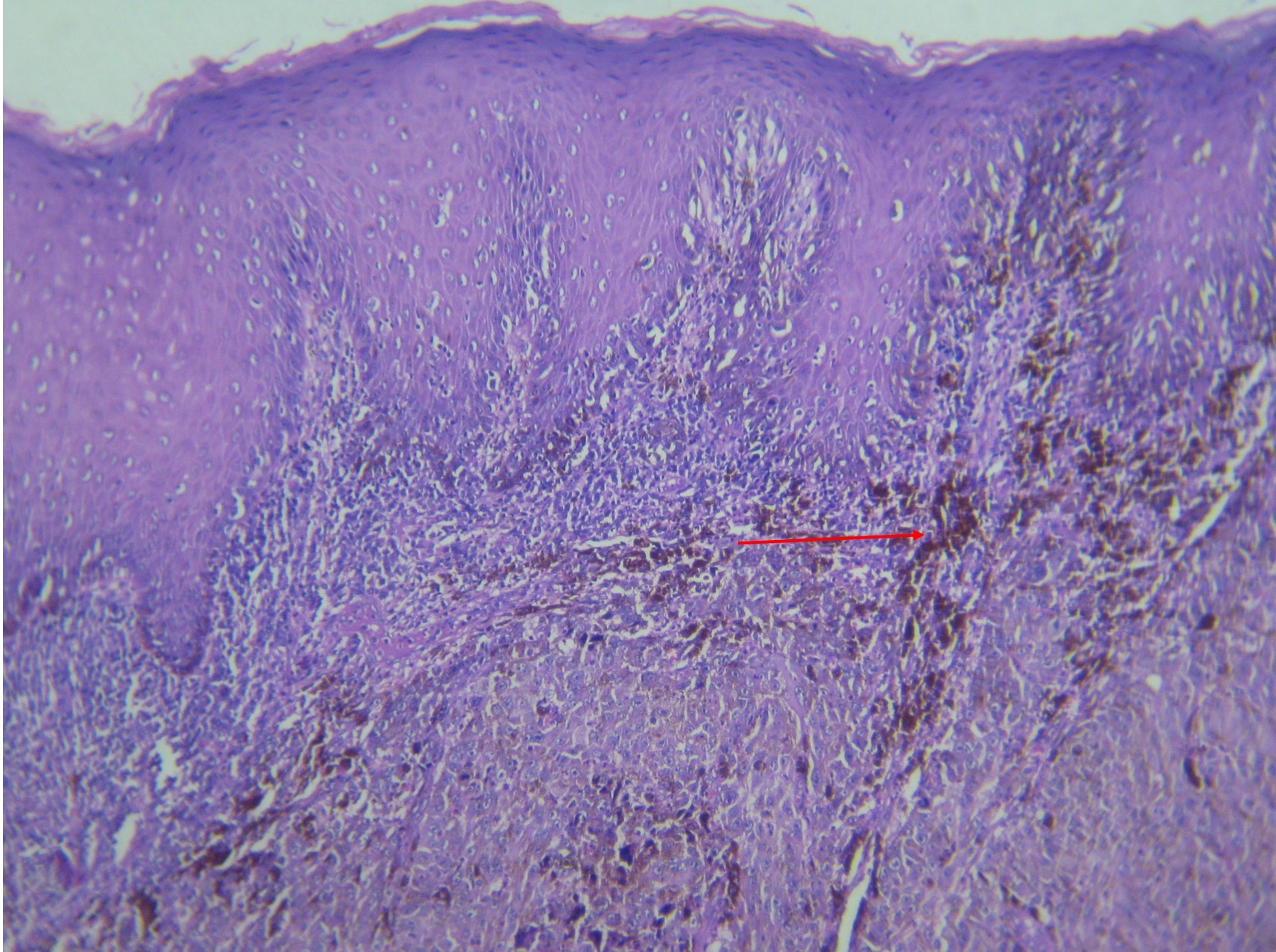
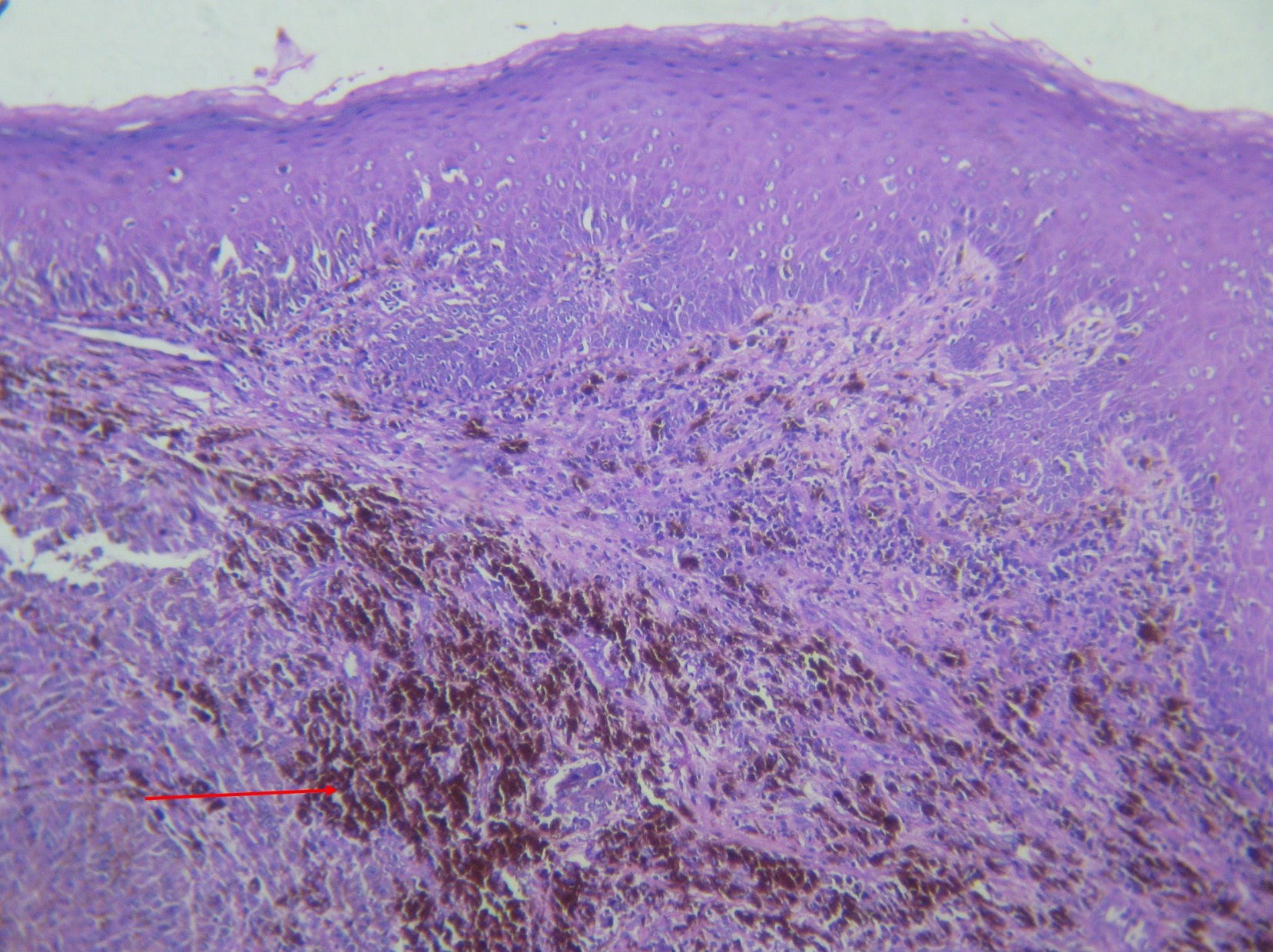
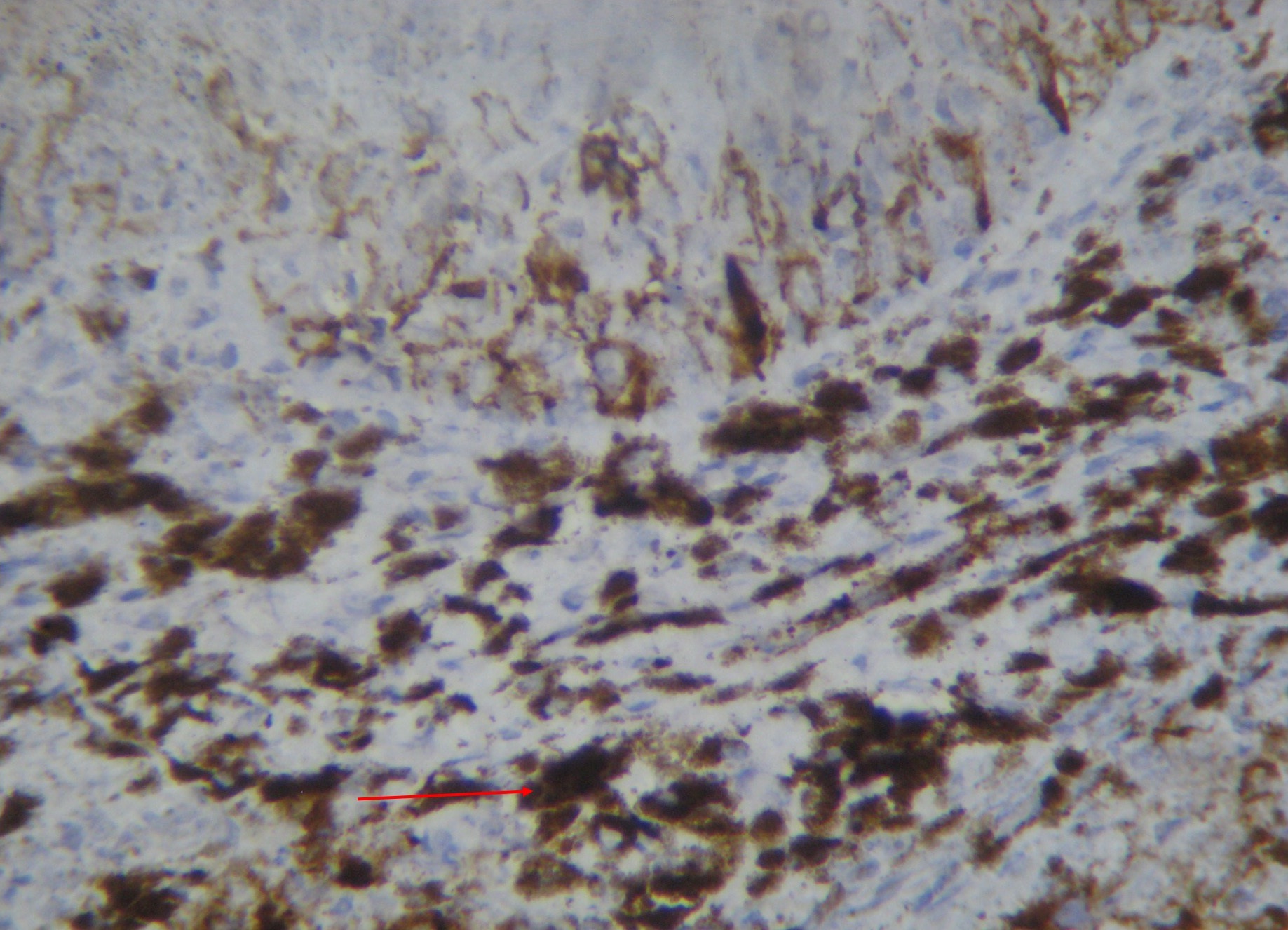
H&E stained sections of incisional biopsy specimen showed nodular mass of malignant melanocytes invading into the connective tissue. The malignant cells were atypical, hyperchromatic, spindle shaped cells with vesicular, hyperchromatic nuclei and prominent nucleoli. Few mitotic figures were also seen. The cells contained fine melanin granules that appeared brownish in colour. These cells were distributed into sheets and groups in the juxta-epithelial region and mucosa. The overlying epithelium was stratified squamous and showed dysplastic features such as hyperchromatism and loss of polarity [Table/Fig-6,7]. Immunohistochemical staining was performed to confirm the origin of the malignant cells. HMB 45, which is the preferred marker for melanocytes, was used and the cells showed high positivity for HMB 45 marker thus confirming diagnosis of melanoma [Table/Fig-8].
Photomicrograph showing stratified squamous epithelium with invasion of melanocytes in the connective tissue (H&E 10x).
Photomicrograph showing sheets of atypical melanocytes invading into the connective tissue. The melanocytes are pleomorphic and show brown pigmentation. (H&E 10x).
Photomicrograph of IHC marker S-100 showing high positivity for melanocytes (40x).
Based on the histopathological features and immunohistochemistry, a confirmatory diagnosis of invasive nodular malignant melanoma was given.
Discussion
Melanoma constitutes only 3%- 5 % of all cutaneous malignancies, and accounts for most skin cancer related deaths (77%) [1]. Oral melanoma is aggressive neoplasm which accounts for less than 0.5% of all melanomas commonly affecting palate and maxillary gingiva whereas mandible, tongue, buccal mucosa and upper and lower lip are less frequently affected [2,3]. Our patient is one of those rare case with the lesion occurring in the mandibular gingiva. It occurs in adults between 55 and 65 years of age and exhibits a male predilection. In our case also the age and gender of the patient was in accordance with the above mentioned findings [4]. Although there is no racial predilection, Afro-Americans and Asians are more commonly affected than Caucasians [5]. The aetiology of oral malignant melanoma is unknown, in contrast to cutaneous melanoma, which is linked to sun exposure. Most melanomas are thought to arise de novo or due to risk factors like chronic irritation and tobacco use [6]. Our patient gave history of bidi smoking approximately 5 to 10 bidis per day for 25 years. Melanoma presents itself as a growth or swelling with smooth intact or ulcerated overlying mucosa. Oral melanoma shows colour variations which may range from black, brown, gray, purple, and may also show red shades, or may be depigmented [7]. Our case also exhibited asymptomatic swelling which was grayish black in colour with smooth & sessile surface and well defined borders. On the basis of clinical appearance, oral malignant melanoma was classified by Lopez et al., into pigmented nodular type, non-pigmented nodular type, pigmented macular type, pigmented mixed-type, and non-pigmented mixed type [8]. The lesion in our case was of the pigmented nodular type. After the diagnosis the patient was referred to higher center for excision and further treatment.
Surgery remains the most effective treatment for malignant melanoma [9]. The primary lesion is excised via an intraoral approach and 1.5 cm of healthy tissue is usually involved in excision [10]. Lymph node involvement reduces the survival rate of the patient. In our case there was no regional lymph node involvement detected on clinical palpation, however excision along with neck dissection was performed at higher center. Surgery is combined with radiotherapy, chemotherapy and immunotherapy as adjuvant treatment methods. The prognosis of oral malignant melanoma is poor with five-year survival rate ranging from 4.5 – 48% [11].
Conclusion
Most oral melanomas are often asymptomatic and large in presentation, delaying the diagnosis until symptoms occur. A high level of suspicion, precise history and a thorough physical examination by dentists regarding these malignancies are essential as the patients often neglect their complaints. The present case also emphasis the need of early diagnosis and prompt treatment which would result in better prognosis.
[1]. Boring CC, Squires TS, Tong T, Montgomery S, Cancer statistics, 1994CA Cancer J Clin 1994 44:7-26. [Google Scholar]
[2]. Ebenezer J, Malignant melanoma of the oral cavityIndian J Dent Res 2006 17:94 [Google Scholar]
[3]. Bhullar R, Bhullar A, Vanaki S, Puranik R, Sudhakara M, Kamat M, Primary melaonoma of oral mucosa: A case report and review of literatureDent Res J 2012 9(3):353-56. [Google Scholar]
[4]. Reddy B, Sridhar GR, Anuradha CH, Chandrasekhar P, Lingamaneni KP, Malignant melanoma of the mandibular gingiva: A rare occurrenceIndian J Dent Res 2010 21:302-05. [Google Scholar]
[5]. Bujas T, Pavic I, Prus A, Marusic Z, Balicevic D, Primary oral malignant melanoma:case reportActa Clin Croat 2010 49(1):55-59. [Google Scholar]
[6]. Symvoulakis EK, Kyrmizakis DE, Drivas EI, Koutsopoulos AV, Malandrakis SG, Skoulakis CE, Oral mucosal melanoma: A malignant trapHead Face Med 2006 2:7 [Google Scholar]
[7]. Gondivkar SM, Indurkar A, Degwekar S, Bhowate R, Primary oral malignant melanoma–a case report and review of the literatureQuintessence Int 2009 40(1):41-6. [Google Scholar]
[8]. Lopez-Graniel CM, Ochoa-Carrilo FJ, Menese-Garcia A, Malignant melanoma of the oral cavity: diagnosis and treatment experience in a Mexican populationOral Oncol 1999 35:425-30. [Google Scholar]
[9]. Dimitrakopoulos I, Lazaridis N, Skordalaki A, Primary malignant melanoma of the oral cavity Report of an unusual caseAust Dent J 1998 43:379-81. [Google Scholar]
[10]. Younes MN, Myers JN, Melanoma of the head and neck: Current concepts in staging, diagnosis and managementSurg Oncol Clin N Am 2004 13:201-29. [Google Scholar]
[11]. Manigandan T, Sagar GV, Amudhan A, Hemalatha VT, Babu NA, Oral malignant melanoma: A case report with review of literatureContemp Clin Dent 2014 5:415-18. [Google Scholar]