Diabetes mellitus is a metabolic disorder characterized by chronic hyperglycaemia with disturbances of carbohydrate, fat and protein metabolism resulting from defects in insulin secretion, insulin action, or both. Type 2 (non–insulin dependent) Diabetes mellitus is one of the preventable non communicable disease resulting in increased morbidity and mortality in developing countries like India. It is characterized by disorders of insulin action and/or insulin secretion. Number of people with Type 2 Diabetes is growing rapidly worldwide with economic development, ageing populations, increasing urbanisation, dietary changes, reduced physical activity and lifestyle changes. The global prevalence of diabetes is 9%, while in India it is 8.63% and in Tamil Nadu it is 10.4%.
National and State programmes on Diabetes control are implemented to combat the disease burden. A detailed review of the programme modules, operational guidelines and visit to health facilities were done to understand the implementation process related to control of Diabetes mellitus. As part of these programmes, opportunistic screening is implemented for target population. Though these programmes are unique, there are few lacunae identified which are missing opportunities and time consuming. There are no strategies so far in such programmes to make the screened positive cases to undergo confirmatory tests. Since screening is only opportunistic, the screened positive cases can be subjected to undergo confirmatory tests by different methods. The specified roles and responsibilities of health staffs at various levels to ensure follow up should also be framed and followed. The objective of this article is to review the existing strategies and to suggest the need for follow up pathways to be adopted from the first contact level to the level of final confirmation for better compliance.
Metabolic disorder, NCD Programmes, Random blood sugar
Introduction
Diabetes mellitus is a metabolic disorder characterized by chronic hyperglycaemia with disturbances of carbohydrate, fat and protein metabolism resulting from defects in insulin secretion, insulin action, or both [1]. Diabetes mellitus is classified into 3 types based on the aetiology [1]:
(1) Type 1 diabetes (insulin dependent).
(2) Type 2 diabetes (non-insulin dependent).
(3) Other specific type of diabetes (gestational diabetes).
Type 2 Diabetes mellitus is characterized by disorders of insulin action and/or insulin secretion [1]. It is one of the preventable non communicable diseases (NCDs), resulting in increased morbidity and mortality in developing countries like India. Owing to the rising prevalence of disease due to both modifiable and non-modifiable risk factors and there being a long latent, asymptomatic period in which diabetes can be detected, it is essential for early diagnosis and treatment of diabetes. This will prevent the complications that affect the vascular system, nervous system and organs like eye, heart and kidney.
Global Burden
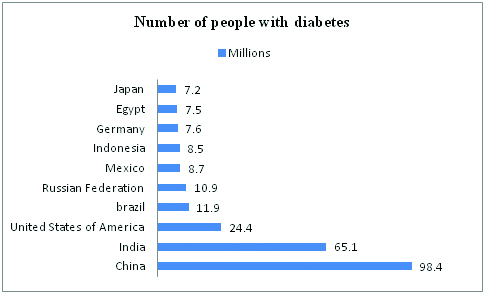
The leading causes of NCD deaths in 2012 were cardiovascular diseases, cancers, respiratory diseases including asthma, chronic obstructive pulmonary disease and diabetes alone accounting to 1.5 million or 4% of NCD deaths and 89 million disability adjusted life years (DALYs) [2]. Thus, these four major NCDs were responsible for 82% of NCD related deaths [2]. The proportion of deaths under the age of 70 years, attributed to NCDs is 52% of which the cause of deaths due to Diabetes mellitus is 4% [2]. In 2013, the top ten countries/territories for number of people with diabetes in the age group of 20 to 79 years are depicted in [Table/Fig-1] [3]. In 2014, the global prevalence of diabetes was estimated to be 9% [2].
Top 10 countries/territories for number of people with diabetes (20 to 79 years), 2013, IDF [3]
In India
As per the International Diabetes Federation report in 2014, the total number of diabetic cases is 66 million, prevalence is 8.63% and deaths due to diabetes is 10.4 lacs [4]. In 2011, a study by Indian Council of Medical Research, India Diabetes(INDIAB), Phase I done in the rural and urban settings in 3 States and 1 Union Territory, shows the prevalence of diabetes in Tamil Nadu as 10.4%, 8.4% in Maharashtra, 5.3% in Jharkhand, and 13.6% in Chandigarh. The prevalence of pre diabetes (impaired fasting glucose and/or impaired glucose tolerance) is 8.3% in Tamil Nadu, 12.8% in Maharashtra, 8.1% in Jharkhand and 14.6% in Chandigarh respectively [5].
Screening for early diagnosis of type 2 Diabetes Mellitus
For an early diagnosis, screening is essential to identify individuals who are in the pre-diabetes state and diabetes state to intervene at the right time to prevent a pre-diabetic to become a diabetic and a diabetic to be affected by further complications. Screening is defined as the presumptive identification of unrecognised disease or defect by application of tests, examinations and other procedures which can be applied rapidly. A screening test is not intended to be diagnostic [6]. There are several approaches to screen diabetes such as screening the entire population, targeted/ selective screening and opportunistic screening. The screening tool for diabetes might vary depending upon the feasibility of the screening programme when it comes to cover a wider community. The screening tools that one can opt for are risk assessment questionnaire, biochemical tests or combination [1].
Opportunistic screening
Opportunistic screening is carried out at a time when people are seen by health care professionals, for a reason other than the disorder in question [1]. When it comes to opportunistic screening for diabetes, the patient or the attender visiting the hospital for some other reason, is sensitized to undergo screening for diabetes. The individual undergoing screening might be in a fasting state or would have had a cup of tea or a meal and the time interval between his last meal and the screening varies widely from patient to patient and is not possible to retrieve that history every time one comes for screening. In that case, under opportunistic screening, the blood sample collected will be taken for testing as random blood sugar (RBS). Suppose, if the value of random blood sugar is above the cut off value, then the individual is requested to come another day for testing fasting blood sugar (FBS) and post prandial blood sugar (PPBS) to confirm the diagnosis. But, whether the individual will return another day to undergo the said tests is uncertain. Even if the individual is going to return the next day or some other day for testing fasting and post prandial blood sugar, the individual has to again come another day to the health facility to get the report.
So to confirm whether an individual is diabetic or not, the individual has to visit the health facility three to four times after the initial screening. We have to remember that if an individual has overt symptoms that disturbs his day to day life, only then he visits the health facility to get the treatment. In services like opportunistic screening though feasible, whether the individual will return to the health facility three to four times spending those few hours of their work life to know the test results is something that has to be looked into, inspite of how much the individual is motivated. Sometimes, there are chances of false reporting in such situations as well.
A detailed review of National and State programme modules of NCD interventions were carried out [7–11]. An extensive review of published articles related to the need for follow up strategies to confirm diabetes [12–22] was done. These articles were obtained through internet search of medical literature in Google and Google scholar irrespective of any particular timeline. The key words used for the selection of articles were opportunistic screening, diabetes mellitus, follow up, reminders.
National and State programmes to combat burden of Diabetes Mellitus
In India, National and State Programmes have been launched to combat the burden of NCD, to create awareness among the people, to create a behaviour change, to diagnose at an early stage followed by management and follow up. Two such programmes included in the review are:
National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) implemented by Ministry of Health and Family Welfare, Government of India from 2010.
Programme for Prevention, Screening, Treatment and Follow up of NCDs like diabetes mellitus, hypertension, cervical cancer, breast cancer funded by World Bank and implemented by the Department of Health and Family Welfare, Government of Tamil Nadu from 2011.
A brief description of both these programmes is given in [Table/Fig-2,3]. Tamil Nadu has implemented the NCD intervention programme even before the implementation of NPCDCS. Hence it is proposed that National Programme will supplement the State’s efforts by providing technical and financial support.
National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) [7].
| National Programme for prevention and control of cancer, diabetes, cardiovascular diseases and stroke |
| a. | Objective | Early diagnosis and management of cancer, diabetes, cardiovascular diseases and stroke. |
| b. | Strategy | Opportunistic screening of all individuals aged 30 years and above in all government health facilities and camps. |
| c. | Screening tool for DM | Measuring RBS using glucometer. |
| d. | Cut off values for diagnosis | Fasting blood sugar >/= 126mg/dlPost prandial blood sugar >/=200mg/dl(as per WHO definition 1999) |
| e. | NCD clinic | A NCD clinic is set up in the government health facility starting at a sub centre level to render the screening, treatment and counseling services. The clinic will have a doctor, nurse, counselor, data entry operator in a community health centre level (CHC) and training is imparted to them. For screening of diabetes, glucometer, test strips and auto disabled lancets are procured at central level as per the requirements from time to time. |
| f. | Patient flow | Day 1 | Screening is done using glucometer. The capillary blood test is taken as measuring the random blood sugar. If the RBS is above the cut off value, the individual is considered as suspected diabetic and advised to come the next day or referred to higher facility to test for FBS and PPBS. |
| | Day 2 | The same individual who was screened positive the previous day visits the health facility to undergo tests such as FBS and PPBS by testing plasma glucose. |
| | Day 3 | The individual will visit the health facility to collect the reports and depending on the test result, the individual is referred to medical officer for further advice. |
| g. | Referral and follow up | The suspected cases of diabetes will be referred to CHC or higher health facility for further diagnosis and management. The nurse and counselor should assist in follow up care and referral of screened positive cases for further investigations or treatment. |
| h. | Suspected to be diabetic [8] | 6.13% |
Programme for prevention, screening, treatment and follow up of NCDs in Tamil Nadu [9,10].
| Programme for prevention, screening, treatment and follow up of NCDs |
| a. | Objective | To reduce the morbidity and mortality due to diabetes and other NCDs by screening for early detection and treatment. |
| b. | Strategy | Opportunistic screening of all men and women aged 30 years and above for hypertension & diabetes mellitus while women in addition are screened for cervical and breast cancer. |
| c. | Screening tool for DM | Measuring RBS by analysing in semi – auto analyser |
| d. | Cut off values for diagnosis | Random blood sugar >200mg/dl with symptoms of diabetes.orRandom blood sugar from 110 to 200mg/dl, advised for FBS PPBS.Fasting blood sugar >/= 126mg/dlPost prandial blood sugar >/=200mg/dl(as per ADA guidelines 2009) |
| e. | NCD clinic | A NCD clinic is set up in all the government health facilities starting from a primary health care with trained staff nurses exclusively posted to carry out screening services. The clinic is fully equipped with the required logistics like equipments, registers, reagents and drugs to carry out the intervention smoothly. Online screens for real time data entry is also provided in the health facilities. |
| f. | Patient flow | Day 1 | Screening is done by collecting the blood sample to analyse the plasma glucose level. The sample withdrawn is taken as measuring the random blood sugar. The sample has to be analysed in a semi auto analyser. The individual is asked to visit the health facility next day to collect the report. |
| | Day 2 | The individual returns to the health facility to get the report and if the RBS value is above the cut off value, then is advised to come the next day to undergo confirmatory tests like fasting blood sugar and post prandial blood sugar. |
| | Day 3 | The screened positive individual returns to undergo fasting as well as 2 hour post prandial blood sugar tests. |
| | Day 4 | The individual returns to collect the report and depending upon the results the individual is referred to the medical officer for further management. |
| g | Referral and follow up | The follow up of cases for investigations is done by the staff nurse posted in NCD clinic. For confirmed cases, follow up is done by providing drugs for a month and investigations like FBS, PPBS, Sr. cholesterol, Sr. creatinine, urine albumin are done once is 3 months. The complicated cases of diabetes are however referred to higher centres from PHC. |
| h. | Positivity rate [11] | 4.21% |
Advantages of such programmes-
Helps in identifying the undiagnosed pre-diabetic and diabetic cases in the community.
Provides management and monthly follow up for the diagnosed cases.
Provides an opportunity for Inter Personal Communication (IPC) on healthy life style modifications.
Creates awareness to a large number of people about services available in health facilities and to avail them for free of cost.
Individuals who are conscious about their health will definitely follow the advice given by health staffs for follow up and referral and adhere to management.
Gaps identified related to follow up of screened positive cases.
Based on the extensive review the following gaps were observed in the existing programmes:
A maximum number of 3 to 4 visits should be done by the individual to know the blood glucose test results.
The programme guidelines and modules don’t mention about the ways for stringent follow up of screened positive cases to undergo confirmatory tests and the same is not imparted during the training also.
The roles and responsibilities of health staff to follow screened positive cases at different levels are not explained.
In NPCDCS programme, the focus on how the referral is done in screening camps and ensuring the screened positive individuals visit to the health facility is not clear.
The reports only reflect on suspected to be diabetic or the positivity rate but not on the number that needs confirmatory tests.
Recommendations
There are various studies done in different regions that emphasize on the number of loss to follow up of diabetes patients and need for follow up strategies [12–22]. Since screening test and confirmatory tests are different to diagnose Diabetes mellitus, certain strategies to ensure follow up can be framed and followed such as:
Preparation of line listing of screened positive cases with contact details like full address and phone number on a daily basis can be shared with field staffs to mobilize the individuals to health facility [11].
The screened positive cases can be subjected to undergo the confirmatory tests by arranging camps or outreach activities once in fortnight so that it is possible to mobilize those individuals with prior information.
The government can provide facilities to make reminder calls or send short message services or automated voice messages or flash messages through mobile technology from the respective health facility about the test report and further advice to act upon by the individual [11,12,15,21,22].
Reminder letters through postal services can be utilized to ensure follow up of cases [13].
The health facilities are provided with Hospital Management System (HMS) and (Health Management Information System (HMIS) for online reporting in states like Tamil Nadu [9,10], which can be utilised for tracking the screened positive cases [13,14,17].
The operational guidelines or the training manual of any such programme should provide the follow up mechanism or algorithm in detail [17] and the roles and responsibilities of every individual category of health staff to be involved should be mentioned [11].
Information Education Communication (IEC) messages emphasizing not only on healthy lifestyle modification (LSM) and screening services provided in health facilities but also on the importance to follow up to undergo confirmatory tests should be highlighted [14].
Conclusion
Community based pilot studies should be done in order to find out the most feasible and cost effective ways to follow up with the screened positive case to undergo confirmatory tests. Reducing the number of visits to health facility from 4 to a minimum of 2 visits to know the test results will have scope for better compliance, cooperation and follow up. The data of such programmes or studies should not just reflect on the prevalence of diabetes overall but the split up details such as the number of screened positive cases, number of cases that require the confirmatory tests, the number who underwent the confirmatory tests and diagnosed to have the disease and the number initiated with treatment should also be included. Such complete screening and undergoing of confirmatory tests by the targeted individual will provide the actual burden of diabetes overall and also prevent chances of any false positive or false negative reporting. This will make the reporting more reliable and valid to plan feasible interventions to reduce the morbidity and mortality due to diabetes mellitus.
[1]. Screening for Type II Diabetes: Report of a World Health Organisation and International Diabetes Federation Meeting: 2003 WHO. [Internet]. [cited 2015 November 11]. Available from http://www.who.int/diabetes/publications/en/screening_mnc03.pdf [Google Scholar]
[2]. Global Status Report on Non communicable Diseases: 2014 WHO. [Internet]. [cited 2015 November 11]. Available from http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf?ua=1 [Google Scholar]
[3]. International diabetes Federation (IDF) Diabetes Atlas: 6th Edition: 2013 IDF. [Internet]. [cited 2015 November 11]. Available from https://www.idf.org/sites/default/files/EN_6E_Atlas_Full_0.pdf [Google Scholar]
[4]. International diabetes Federation (IDF) Diabetes Atlas: 6th Edition: 2014 update IDF. [Internet]. [cited 2015 November 11]. Available from https://www.idf.org/sites/default/files/Atlas-poster-2014_EN.pdf [Google Scholar]
[5]. Anjana RM, Pradeepa R, Deepa M, Datta M, Sudha V, Unnikrishnan R, Prevalence of diabetes and prediabetes in urban and rural India: phase I results of the Indian Council of Medical Research–INdiaDIABetes (ICMR–INDIAB) studyDiabetologia 2011 54:3022-27. [Google Scholar]
[6]. Wilson JMG, Jungner G. Principles and practice of screening for disease: 1968 WHO. [Internet]. [cited 2015 November 11]. Available from http://www.who.int/bulletin/volumes/86/4/07-050112bp.pdf [Google Scholar]
[7]. Operational guidelines: National Programme for prevention and control of cancer, diabetes, CVD and stroke (NPCDCS): Directorate General of Health Services: Ministry of Health and Family Welfare [Internet]. [cited 2015 November 11]. Available from https://www.health.bih.nic.in/Docs/Guidelines/Guidelines-NPCDCS.pdf [Google Scholar]
[8]. Press Information Bureau: National Programme for prevention and control of cancer, diabetes, CVD and stroke (NPCDCS): Ministry of Health and Family Welfare [Internet] 9-December-2013 17.32 IST. [cited 2015 November 11]. Available from https://www.pib.nic.in/newsite/PrintRelease.aspx?relid=101234 [Google Scholar]
[9]. Tamil Nadu Health Systems Project, Clinical manual on NCD interventions for medical and paramedical staff, Department of Health and Family Welfare Department, Government of Tamil Nadu, 2012 [Google Scholar]
[10]. Tamil Nadu Health Systems Project, Manual for programme managers, programme for prevention, screening and treatment of non communicable diseases, Department of Health and Family Welfare Department, Government of Tamil Nadu, 2011 [Google Scholar]
[11]. Tamil Nadu Health Systems Project, Patient follow-up pathway, NCD intervention programme. Department of Health and Family Welfare Department, Government of Tamil Nadu, 2015 [Google Scholar]
[12]. Shewade HD, Palanivel C, Balamurugesan K, Vinayagamoorthi R, Sunderamurthy B, Vasudevan Feasibility of opportunistic screening for type 2 diabetes mellitus: Need for interventions to improve follow upJournal of Social Health and Diabetes 2015 3(1):43 [Google Scholar]
[13]. Sargeant LA, Simmons RK, Barling RS, Butler R, Williams KM, Prevost AT, Who attends a UK diabetes screening programme? Findings from the ADDITION-Cambridge studyDiabetic Medicine 2010 27(9):995-1003. [Google Scholar]
[14]. Ealovega MW, Tabaei BP, Brandle M, Burke R, Herman WH, Opportunistic screening for diabetes in routine clinical practiceDiabetes Care 2004 27(1):9-12. [Google Scholar]
[15]. Kumar S, Shewade HD, Vasudevan K, Durairaju K, Santhi VS, Sunderamurthy Effect of mobile reminders on screening yield during opportunistic screening for type 2 diabetes mellitus in a primary health care setting: A randomized trialPreventive Medicine Reports 2015 2:640-44. [Google Scholar]
[16]. Venugopal V, Selvaraj K, Majumdar A, Chinnakali P, Roy G, Opportunistic screening for diabetes mellitus among adults attending a primary health center in PuducherryInternational Journal of Medical Science and Public Health 2015 4(9) [Google Scholar]
[17]. Sailesh M, Prabhakaran D, Noncommunicable Diseases in India: Challenges and Implications for Health Policy, India Infrastructure Report, 2013/14. p.213 – 222. [Internet]. [cited 2015 November 11]. Available from http://www.idfc.com/pdf/report/2013-14/Chapter-17.pdf [Google Scholar]
[18]. Woolthuis EPK, de Grauw WJ, van Gerwen WH, van den Hoogen HJ, van de Lisdonk EH, Metsemakers JF, Yield of opportunistic targeted screening for type 2 diabetes in primary care: the diabscreen studyThe Annals of Family Medicine 2009 7(5):422-30. [Google Scholar]
[19]. Dhippayom T, Fuangchan A, Tunpi S, Chaiyakunapruk N, Opportunistic screening and health promotion for type 2 diabetes: an expanding public health role for the community pharmacistJournal of Public Health 2012 :fds078 [Google Scholar]
[20]. Jeppesen C, Kristensen JK, Ovesen P, Maindal HT, The forgotten risk? A systematic review of the effect of reminder systems for postpartum screening for type 2 diabetes in women with previous gestational diabetesBMC Research Notes 2015 8(1):373 [Google Scholar]
[21]. Friedman RH, Automated telephone conversations to assess health behavior and deliver behavioral interventionsJournal of Medical Systems 1998 22(2):95-102. [Google Scholar]
[22]. Kenealy T, Arroll B, Petrie K J, Patients and computers as reminders to screen for diabetes in family practiceJournal of General Internal Medicine 2005 20(10):916-21. [Google Scholar]