Mediterranean basin (Portugal, Spain, Southern France, Italy, Greece, Turkey, North Africa), Mexico, South & Central America, Eastern Europe, Asia, Africa, the Caribbean and the Middle East are listed by CDC as high risk areas for brucellosis [1].
Sporadic cases amongst the travelers from non-endemic countries are reported after their travel to endemic countries [2,3]. Even though countries like UK, Australia, New Zealand, Japan and Canada have been declared Brucella free, half a million new cases of human brucellosis are reported worldwide [4,5] and human brucellosis is a major zoonotic disease in India owing to the fact that more than 70% of total population reside in approximately 5,00,000 villages [6,7]. The problems with diagnosis of human brucellosis include its protean manifestations, unawareness amongst clinicians, poor culture yields, difficulties in interpretations of serology results due to presence of endemic titers and usage of non-standardized kits for antibody estimations.
We evaluated two serological tests which are easy to perform, very economical and PCR which is highly sensitive and specific diagnostic tool for diagnosis of human brucellosis but costly and technically demanding, with culture which is considered as gold standard due to its specificity. This was to ascertain the best modality for diagnosing brucellosis in areas which are endemic not only for brucellosis but also for cross reacting gram negative bacterial pathogens and resources including technically qualified manpower are scarce. The uniqueness of this study lies in location of study and patients’ demographic profile since the area in and around Belgaum (South India) is endemic for brucellosis [8] leading to persistently elevated antibody levels in general population. Further the clinical profile was not suggestive of brucellosis to attending physicians due to lack of typical symptoms of brucellosis and infections with cross reacting gram negative bacilli viz E.coli, Salmonella, Vibrio are very common in this area.
The aim of the study was evaluation of conventional serological techniques and PCR for diagnosis of human brucellosis in and around north Karnataka which is endemic for brucellosis and patients often present with elevated base line antibody titers and confounding clinical manifestations.
Materials and Methods
The study was designed as cross-sectional and carried out over a period of 18 months (January 2004-July 2005) in the serology and molecular biology sections of Microbiology department of Jawaharlal Nehru Medical College after obtaining clearance from institute ethics committee.
Four hundred patients with chief complaint of acute undifferentiated fever (AUF) reporting to KLE Dr Prabhakar Kore hospital and medical research center were included in this study. Majority of patients belonged to north Karnataka which is endemic for brucellosis. Blood/serum samples of these patients were submitted to Microbiology department for one or more AUF investigations like Widal, Venereal Disease Research Laboratory (VDRL) test for syphilis, Anti-Streptolysin O (ASLO), Malaria.
Inclusion Criteria
Patients with undifferentiated fever of > 10 days were included in the study.
Exclusion Criteria
Patients with less than 10 days of fever or those who had tested positive for malaria/Widal/VDRL/ASLO were excluded from the study.
Sample size was calculated with estimated sensitivity of SAT as 75% and specificity at 90% with reference standard of culture with relative precision of 15% and prevalence of brucellosis was considered as 15% in endemic area. All calculations were done for estimation with 95% confidence. Calculated sample size was 381. We have enrolled 400 participants.
All 400 were subjected to culture, Brucella slide agglutination test (SAT), and Brucella standard tube agglutination test (STAT) with 2ME.
Serology
Both the SAT and STAT antigens were procured from Division of Biological Products, Indian Veterinary Research Institute, Izzatnagar, (Uttar Pradesh), India, which prepares the antigen in conformity to international reference laboratories. Four hundred serum samples received at serology section of Department of Microbiology over a period of six months for one or the febrile agglutination tests for diagnosis of AUF were included in the study. Despite absence of differential diagnosis of brucellosis by physicians, all 400 serum samples were subjected to Brucella slide agglutination test (SAT), using Rose Bengal Plate Test (RBPT) antigen which is a Rose Bengal dye stained phenolised 8% suspension of pure smooth killed cells of Brucella abortus strain 99 and buffered at pH 3.65 using lactic acid buffer. The tests were performed using positive control (serum sample known to have Brucella antibody titers ≥ 80 IU/ml, obtained in Standard tube agglutination test) and a negative control (serum from healthy person) simultaneously.
The STAT was performed using Brucella abortus plain antigen which is unstained suspension of pure smooth culture of Brucella abortus strain 99 in phenol saline. In parallel to STAT, the samples were also subjected to 2-merceptoethanol (2ME), which provide information as regards to the amount of anti-Brucella IgG agglutinins present in the serum by dissolving disulfide bonds which link IgM molecules to release the subunits, thus inactivating the IgM antibodies. The Brucella standard tube agglutination test was performed with a set of antigen control tubes with which agglutination of serum samples were compared with and minimum of 50% agglutination was considered as end-point and each set had 12 tubes for testing patient’s serum in doubling dilution and 5 tubes as antigen control as prescribed by IVRI Izzatnagar, the manufacturer of the Brucella antigens. A test was considered positive only if agglutination titer were above the cut-off value of ≥80 IU/ml determined by STAT. The cut-off value of ≥80 IU/ml was used as per the cut-off value provided by the IVRI Izzatnagar along with antigen for considering a serum sample positive for brucellosis in humans.
Culture
For culture, 5-10 ml of blood was inoculated to brain-heart infusion (BHI) medium poured in biphasic manner (Castaneda method) and incubated at 37°C up to four weeks or till the time of appearance of growth, whichever was earlier. The growth was identified as Brucella on the basis of Gram stain morphology, positive oxidase test and rapid hydrolysis of Urea demonstrated in Christensen’s urease medium.
PCR
IS711 downstream of BMEI1162 (Gene bank accession number NC_003317) was used as target for DNA amplification and the primers were 5’AAC AAG CGG CAC CCC TAA AA3’ (Forward Primer) and 5’CAT GCG CTA TGA TCT GGT TACG3’ (Reverse Primer) giving 279bp amplification product. The primers and PCR mastermix were obtained from Bangalore Genie Ltd, Bangalore. Though IS711 is considered a conserved insertion sequence asused previously also L Zerva et al., we also tested 18 culture isolates of Brucella melitensis isolated in our department over a period for ascertaining the presence of IS711 gene by PCR in Brucella species prevalent in this part of country [9]. IS711 was detected in all 18 isolates and then it was decided to use this as target in PCR for identifying Brucella melitensis in serum samples included in this study. DNA extraction from the serum samples and amplification was performed by following the method described by L Zerva et al., [9].
The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), diagnostic accuracy and likelihood of positive test were calculated for SAT and STAT as compared to culture considered as the gold standard.
Results
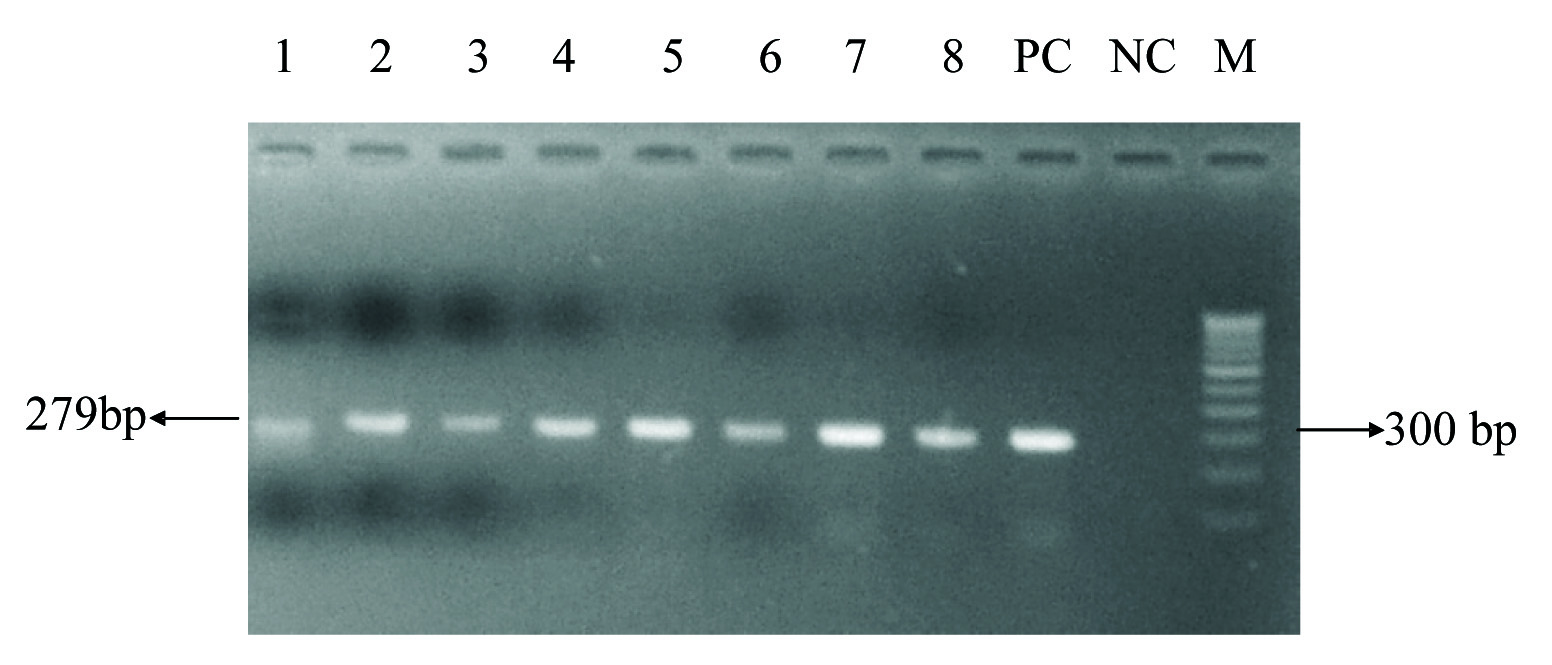
Brucella was isolated in culture in 20 blood samples only. Thirty five cases were positive by Brucella slide agglutination test, whereas 34 cases had antibodies levels of ≥ 80IU/ml cut-off value in Brucella standard tube agglutination test (STAT). Thirty two cases found positive by PCR as evident by presence of IS711 providing 279 bp amplicon [Table/Fig-1]. Two patients having antibodies titres of 160 IU/ml (above the cut-off value of 80IU/ml), were negative by PCR.
PCR for IS711 gene (279bp), Lane 1-8: Serum samples. PC: Known strain of Brucella melitensis isolated and identified in own institute. NC: PCR master mix without template. M: Molecular weight marker (100 bp).
Antibody titres obtained in STAT ranged from 20 IU / ml to 10240 IU/ml [Table/Fig-2]. Titres obtained with 2-ME showed simultaneous presence of anti-Brucella IgG antibodies along with much elevated IgM antibodies in many cases suggesting acute exacerbation. The sensitivity, specificity positive predictive value, negative predictive value, diagnostic accuracy and likelihood ratio of a positive test for SAT and STAT compared with culture are provided in [Table/Fig-3a3b,4a&b]. As compared to 34 case found positive by serology only 20 (57%) blood samples yielded Brucella in culture. All samples positive by culture were found positive by PCR also. Another important observation from this study is probable need to raise cut-off titers to ≥160 IU/ml from the existing ≥80 IU/ml in this endemic region for better clinical correlation.
Titers of cases as determined by STAT (n=35).
| Titers (I.U./ml) | Number of cases |
|---|
| 20 | 01 |
| 160 | 09 |
| 320 | 02 |
| 640 | 05 |
| 1280 | 06 |
| 2560 | 05 |
| 5120 | 05 |
| 10240 | 02 |
| Total=35 |
Result of SAT as compared to gold standard blood culture.
| SAT | Blood culture |
|---|
| Positive | Negative | Total |
|---|
| Positive | 20 | 15 | 35 |
| Negative | 0 | 365 | 365 |
| Total | 20 | 380 | 400 |
Diagnostic test parameters of SAT for diagnosis of human brucellosis.
| Parameter | Estimate | Lower-upper 95% CIs |
|---|
| Sensitivity | 100% | (83.89, 1001) |
| Specificity | 96.05% | (93.59, 97.591) |
| Positive Predictive Value | 57.14% | (40.86, 72.021) |
| Negative Predictive Value | 100% | (98.96, 1001) |
| Diagnostic Accuracy | 96.25% | (93.91, 97.711) |
| Likelihood ratio of a Positive Test | 27.14 | (23.6–31.22) |
Result of STAT as compared to gold standard blood culture.
| STAT | Blood culture |
|---|
| Positive | Negative | Total |
|---|
| Positive | 20 | 14 | 34 |
| Negative | 0 | 366 | 366 |
| Total | 20 | 380 | 400 |
Diagnostic test parameters of STAT for diagnosis of human brucellosis.
| Parameter | Estimate | Lower-upper 95% CIs |
|---|
| Sensitivity | 100% | (83.89, 1001) |
| Specificity | 96.32% | (93.91, 97.791) |
| Positive Predictive Value | 58.82% | (42.22, 73.631) |
| Negative Predictive Value | 100% | (98.96, 1001) |
| Diagnostic Accuracy | 96.5% | (94.21, 97.91) |
| Likelihood ratio of a Positive Test | 27.14 | (23.6 – 31.22) |
Results from Open Epi, version 3.
Discussion
Majority of the brucellosis patients (82%) in our study presented with on and off undifferentiated fever of more than 15 days, reiterating the fact that fever remains the chief complaint in brucellosis. In our study though the evaluation of culture was not primary objective, it was performed as adjunct to serology and PCR for its value as gold standard. In 20 blood samples Brucella was isolated. If culture positivity is calculated amongst 35 Brucella seropositive cases it is 57.1%. Culture yields for Brucella in literature vary from 10-90% and are dependent on type of sample, stage of infection, previous use of antibiotics and low yields are also attributed to slow growing nature of this intra-cellular bacteria [10]. Techniques like lysis-centrifugation can provide higher yields as demonstrated by Mantur BG but require strict laboratory containment facilities [11].
Anti-Brucella antibodies were detected by SAT and STAT in all patients which were found positive by PCR and culture. In three patients’ positive by SAT and two patients positive by STAT IS711 gene for Brucella was not detected by PCR. One serum sample had titers of 20 IU/ml in STAT, less than the designated cut-off value and considered not positive. There are three possibilities to be considered in this patient with titers less than the cut-off value (80IU/ml). The first one is presence of endemic titers, which are commonly present in the endemic areas where this study was undertaken. The second possibility could be of early phase of disease, where the significant sero-conversion has not taken place. Third possibility is of cross-reactivity because though the Brucella slide agglutination test is extremely sensitive, but known to lack specificity, as this test detect both the IgG and IgM antibodies and anti- Brucella class M antibodies are known to give cross-reaction with Escherichia coli 0116 and 0157, Salmonella urbana, Yersinia enterocolitica 0:9, Vibrio cholerae, Xanthomonas maltophilia and Afipia clevellandensis [12].
We had two patients who had anti-Brucella antibodies titers of 160 IU/ml (above the cut-off value of 80IU/ml), as detected by STAT, but negative by PCR. One patient was a 25-year-old farmer, with un-united fracture of both bones of left leg and fever for last 12-15 days. Sample was submitted to Microbiology department for suspected enteric fever. Second case was of a 36-year-old male teacher who was diagnosed with brucellosis one year before and had been treated with Rifampin, Doxycycline, and Streptomycin. Patient himself approached to our department, with pain in left hip, both the knees and lipomatous swellings over dorsum of hand, left hypochondrium, rib cage, and right flank. At the time of sample collection, patient was on INH and Doxycycline.
In both the cases though there is a possibility of false negative by PCR, but given to the sensitivity/ detection capacity of PCR, other possibilities cannot be ruled out as PCR has been shown to detect and amplify very little quantity of bacterial DNA likely to be present in blood of patient with clinical brucellosis [13,14].
There could be reasons common for both the aforementioned cases which were not detected by PCR, but having antibody levels above cut-off value. Brucellosis is characterized by exacerbations and remissions, and during remission there may not be any bacteremia and consequently no breakdown products (DNA) present in serum, to be picked up by PCR. Another very important reason could be that population in brucellosis endemic area may have normally elevated high titers of antibodies. In studies from many middle-east countries, Spain and Greece, where also the disease is endemic, cut-off values for considering active infection are higher (≥320 I.U) than of 80 IU/ml taken in the present study [9,14,15].
The cut-off value of ≥80 IU/ml was used as per the cut-off value provided by the IVRI Izzatnagar for considering a serum sample positive for brucellosis in humans. This also provided us an opportunity to determine aptness/utility of these cut-off titers in the face of SAT, STAT, PCR and culture and we found that on account of PCR results probably there is need for upward revision of cut-off titers to ≥160 IU/ml.
Sensitivity and specificity of and SAT as well as STAT was higher that is 100% and 96% respectively when gold standard was the blood culture. The blood culture was used as gold standard because of its 100% specificity even thoughits sensitivity is low due to low yields due to various reasons.
The reason for brucellosis being endemic in developing countries including India is that their economies are largely based on agriculture, making contact of large rural population with livestock inevitable for tilling fields, as source of milk, wool, hide and meat, thus providing definitive risk factors for contracting brucellosis. Additionally practices like conducting delivery of cattle at home without protective gear, consumption of un-boiled milk and keeping cattle sheds in near vicinity of residential premises, frequent movement and mixing of various herds of cattle, sheep and goats and poorly maintained farm hygiene provide ideal settings for acquiring Brucella infection by various routes. Despite being endemic in many of the countries the disease is very much under-diagnosed and under-reported [6]. It is estimated that for every reported case of brucellosis three cases goes unreported thus truly demonstrating tip of iceberg phenomenon [16].
Despite being endemic the diagnosis is often missed mainly because of varied presentations, non-specific symptoms, period of long remissions and unawareness amongst health care providers [17-19].
A 2-ME test which was set up in parallel to Brucella STAT is looked upon as an indicator to the amount of anti-Brucella IgG agglutinins present in the serum. In both these patients’ serum 50% agglutination was observed up to identical dilutions in STAT and 2-ME, suggesting the anti- Brucella antibodies being comprised of predominantly IgG component only. Hence in these patients there are long persisting IgG antibodies which are known to remain positive (greater than or equal to 160) for 1.5 years in up to 48% of the patients despite adequate antibiotic treatment whereas the 2-ME titers are said to remain positive (greater than or equal to 160) in only 9% patients after 1 year, and in only < 4% of patients after 1.5 years [20]. Hence IgG antibodies are not a very good predictor of the disease process on stand-alone basis and this possibility could exist in these two cases and PCR negativity can be explained. Because Brucella melitensis is the prevalent species for causing human brucellosis cases in this region, primers specific for are Brucella melitensis used for PCR. There is possibility, however remote that this might have led these two cases of human brucellosis missed by PCR, as few human cases due to B.abortus are reported in other regions [4].
Possibility of Brucella abortus infection and presence of predominantly IgG base line titers in absence of any active disease could be the two major reasons for the two cases (specially the second patient who had taken full course of anti-Brucella treatment), being found positive by serology but negative by PCR. In either of these two scenarios the PCR results in our study shall be true negative. Accurate seroprevalence of brucellosis in India vary widely and yet to be determined across the country [21] but it is said to be forgotten clinical entity [22] which could be ascribed largely to protean manifestations and inexperience/unawareness about the disease among clinical practitioners.
Limitation
One of the limitations of the study is that PCR was not performed on all 400 samples but only on the SAT positive samples due to paucity of resources but considering these values SAT and STAT can be used instead of culture and PCR in resource poor settings to rule out brucellosis.
Conclusion
It is concluded that in resource poor settings where PCR cannot be routinely performed due to its non-availability /high running cost/lack of trained technical staff, serological tests are the best choice which are much less expensive and can be carried out in any laboratory with basic facilities. The Brucella SAT requires less than two minutes to perform and cost less than 1 INR (60 INR = 1USD) and Brucella STAT costs approximately 5 INR providing quantitative estimation ofantibodies in 24 hours. There is no doubt in our mind that routine screening of all the serum samples (which are submitted for various febrile agglutination tests) for brucellosis will certainly detect more number of Brucella infections than actually suspected by attending physicians, because protean manifestations of brucellosis make clinical diagnosis difficult. Brucella SAT can be used for screening large number of susceptible population in endemic areas requiring only a white ceramic tile and spreader to give results in two minutes at a cost which is small fraction of 1USD. A 2-ME is useful adjunct to STAT from which the information about stage of the disease (acute/ chronic/ acute exacerbation of chronic illness) can be obtained.
Results from Open Epi, version 3.