“Petrified Ears” in Secondary Adrenal Insufficiency
Soumik Goswami1, Partha Pratim Chakraborty2, Sayantan Ray3, Sujoy Ghosh4, Subhankar Chowdhury5
1 Residential Medical Officer, Department of Endocrinology and Metabolism, NRS Medical College and Hospital, Kolkata, West Bengal, India.
2 Assistant Professor, Department of Medicine, Midnapore Medical College and Hospital, Midnapore, West Bengal, India.
3 Senior Resident, Department of Endocrinology and Metabolism, Institute of Post Graduate Medical Education & Research and SSKM Hospital, Kolkata, West Bengal, India.
4 Associate Professor, Department of Endocrinology and Metabolism, Institute of Post Graduate Medical Education & Research and SSKM Hospital, Kolkata, West Bengal, India.
5 Professor, Department of Endocrinology and Metabolism, Institute of Post Graduate Medical Education & Research and SSKM Hospital, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sayantan Ray, Room No. 502, Junior Doctors’ Hostel, 244, AJC Bose Road, Kolkata-700020, West Bengal, India.
E-mail: sayantan.ray30@gmail.com
Petrification of the auricle, a rarely encountered clinical entity usually results from ectopic calcification of the auricular cartilages and manifests as rigid ear. The underlying pathogenesis remains ambiguous with several proposed hypotheses till date. Auricular calcification may be the sole cutaneous marker of underlying endocrinopathy at times. Adrenal insufficiency is the most common endocrinological disorder to be associated with such stiff ears and it has been described in both primary as well as secondary forms of the disease. We present here a 30-year-old man whose clinical condition deteriorated following levothyroxine supplementation and the presence of “petrified ears” ultimately provided a clue to the diagnosis of associated secondary adrenal insufficiency.
Auricular calcification, Partial empty sella
Case Report
A 30-year-old man initially presented to his primary care physician with generalized weakness, easy fatiguability and loss of appetite for the preceding year. A thyroid function test was advised which revealed free thyroxine (T4) of 0.71 ng/dL (N, 0.8-1.8 ng/dL) and a thyroid-stimulating hormone (TSH) concentration of 9.8 μIU/mL. He was put on 75 μg of levothyroxine daily, but following initiation of levothyroxine he experienced further deterioration of his symptoms and was referred to our outpatient department. He complained of unintentional weight loss of about 10 kg over the past year. Further enquiry revealed an episode of hospitalization for possible acute bacterial meningitis at the age of 16 years. Physical examination revealed a supine blood pressure of 90/60 mm Hg with no significant postural drop. There was marked rigidity of both ears without any signs of inflammation or scarring [Table/Fig-1a]. No mucosal or skin hyperpigmentation was detected and he had normal secondary sexual characters.
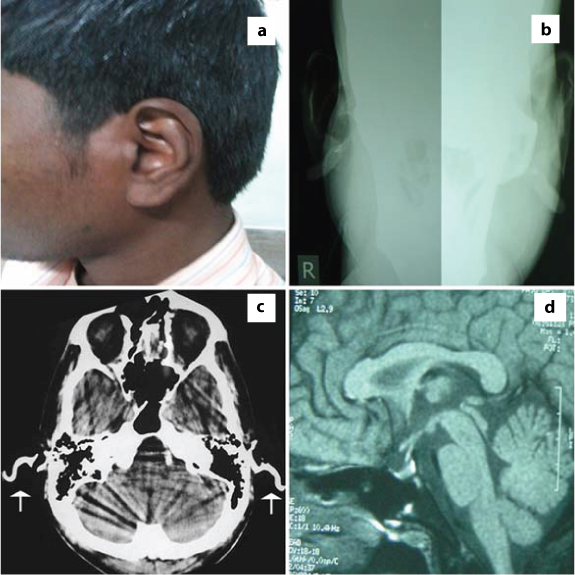
(a) Left ear appeared normal externally; (b) Radiographs of the ears show hyperdense opacity as a sign of calcification of the auricular cartilages; (c) Head CT scan showing high densities of the auricles bilaterally (arrows); (d) MRI of pituitary showing partial empty sella with normal looking pituitary stalkand posterior pituitary bright spot.
Complete blood count and baseline biochemistry were normal. Serum electrolytes and hormonal evaluation revealed the following: Sodium: 136 mEq/L, potassium: 3.9 mEq/L, corrected calcium: 9.5 mg/dl; phosphorus:4.1 mg/dl, parathyroid hormone: 22 pg/ml and 25 (OH) vitamin D: 42 ng/ml. Endocrine work-up revealed morning serum cortisol concentration of <1 μg/dL (N, 5-25 μg/dL), adrenocorticotropic hormone (ACTH) of 5.9 pg/mL (N,10-65pg/ml), free T4 of 1.35 ng/dL, TSH of 0.4 μIU/mL (N, 0.4-4 μIU/mL), with negative thyroid autoantibodies. The results of other anterior pituitary hormone tests were normal. Skull X-ray demonstrated hyperdense opacities over both auricular cartilages [Table/Fig-1b]. Non-contrast Computerized Tomography (CT) scan of head revealed auricular calcification [Table/Fig-1c]. Contrast-enhanced Magnetic Resonance Imaging (MRI) of the hypothalamo-pituitary region revealed partially empty sella with normal stalk [Table/Fig-1d].
The clinical and biochemical profile led to the diagnosis of secondary adrenal insufficiency with secondary hypothyroidism, possibly a late sequel of acute bacterial meningitis. Calcification of auricular cartilages was an unusual cutaneous marker of adrenal insufficiency. The patient was treated with prednisolone at a dose of 5 mg in the morning along with L-thyroxine. He recovered fully, but his ears remain unchanged.
Discussion
“Petrified ears” due to calcified or ossified auricular cartilages is an infrequently encountered clinical entity. In this condition, one or both the ears become stony hard without any alteration in external appearance and the diagnosis is mostly incidental as patients generally do not complain of the same [1]. The most commonly encountered etiologies are local trauma, frost bite, and inflammation. Hypoadrenalism and associated hypercalcaemia is the most common systemic disease underlying stiffening of the auricular cartilages [2,3]. High incidence of this clinical entity has been observed in patients with primary adrenal insufficiency and the clinical presentation varied from mild stiffness of the involved ears to a stony hard feel [4]. Interestingly, although there are several reports of its association with different causes of primary adrenal insufficiency, there are very few reported cases of secondary adrenal insufficiency leading to bilateral rigid auricles [5–8]. Auricular calcification has rarely been reported in other endocrinopathies like diabetes mellitus, hypo and hyperthyroidism, acromegaly, hyperparathyroidism, pseudo-hypoparathyroidism and hypopituitarism [9]. Although the underlying mechanism is yet to be crystallized, increased circulating ACTH has been proposed to play a causative role in primary adrenal insufficiency [10]. However, our patient had secondary adrenal insufficiency with low plasma ACTH. Barkan et al., previously have shown the association of hypopituitarism with auricle ossification and they proposed that the ossification was the result of endogenous cortisol deficiency [5]. Cohen et al., hypothesized that the condition is the result of mesenchymal cells proliferation, which ultimately form a calcified tissue. This process is facilitated by the enhanced input of calcium into the extracellular space because of underlying cortisol insufficiency [11]. Though alteration in calcium homeostasis has been suggested to contribute to ectopic calcification in cortisol deficiency, abnormal serum calcium has not been a constant finding in these patients. As auricular calcification has been predominantly described in males, androgens have also been proposed to play a role [5].
The pathogenesis of this phenomenon is complex and not well understood. Bilateral involvement is more frequent than unilateral involvement, and petrified ears are more commonly encountered in males than in female [12]. Patients may complain of varying degree of ear pain, though most of them are asymptomatic. Clinical examination usually reveals stiffening of the auricular cartilages sparing the lobule. Auricular calcification and ossification cannot be differentiated clinically. Further work-up should include radiography and appropriate biochemistry to detect underlying metabolic or endocrine disorders. A skull X-ray may demonstrate a hyperdense area and a useful first line imaging modality, but a CT of the temporal bones is undoubtedly the investigation of choice with higher sensitivity for this particular finding. Most cases of “petrified ears” are clinically asymptomatic and it is not unusual that there exist no treatment guidelines for this condition.
Conclusion
In our patient, the clinical condition deteriorated following levothyroxine supplementation as thyroid hormones are known to accelerate the metabolism of cortisol. The presence of auricular calcification provided an important clinical clue to the diagnosis of associated adrenal insufficiency and probably helped to avoid case fatality. Laboratory investigations should always be guided and interpreted by the patient’s clinical history and physical examination. Authors believe that all clinicians should be aware of this unusual manifestation of potentially serious and life-threatening endocrinopathies, like cortisol deficiency as in this particular case. Additional reporting and experiences may further elucidate pathophysiologic mechanisms and treatment of such uncommon manifestations of a commonly encountered disease.
[1]. Buikema KE, Adams EG, A rare case of petrified earCase Rep Dermatol Med 2012 2012:1-4. [Google Scholar]
[2]. Novick WH, Calcification of auricular cartilage in Addison’s diseaseArch Otolaryngol 1960 72:448-49. [Google Scholar]
[3]. Gordon DL, Calcification of auricular cartilageArch Intern Med 1964 113:23-27. [Google Scholar]
[4]. Jarvis JL, Jenkins D, Sosman MC, Thorn GW, Roentgenologic observations in Addison’s diseaseRadiology 1954 62:16-29. [Google Scholar]
[5]. Barkan A, Glantz I, Calcification of Auricular cartilages in patients with HypopituitarismJ Clin Endocrinol Metab 1982 55:354-57. [Google Scholar]
[6]. Randall RE, Spong FW, Calcification of the auricular cartilage in a patient with hypopituitarismN Engl J Med 1963 269:1135-37. [Google Scholar]
[7]. Gogate Y, Gangadhar P, Walia RR, Bhansali A, "Petrified ears" with idiopathic adult-onset pituitary insufficiencyIndian J Endocrinol Metab 2012 16:830-32. [Google Scholar]
[8]. Koning MV, Struijs A, Adrenal insufficiency presenting as bilateral rigid auricles: a case reportJ Med Case Rep 2014 8:302 [Google Scholar]
[9]. Strumia R, Lombardi AR, Altieri E, The petrified ear- a manifestation of dystrophic calcificationDermatology 1997 194:371-73. [Google Scholar]
[10]. Siebenmann RE, The ossification of the ear cartilage in Addison’s diseaseSchweiz Med Wochenschr 1977 107:468-74. [Google Scholar]
[11]. Cohen AM, Talmi YP, Floru S, Tsigelman R, Kalmanovitz M, Zohar Y, X-ray microanalysis of ossified auricles in Addison’s diseaseCalcif Tissue Int 1991 48:88-92. [Google Scholar]
[12]. Wang CY, Chang TC, Chen FW, Ossification of the auricles: a forgotten sign in adrenal insufficiencyJ Otolaryngol 2002 31:52-54. [Google Scholar]