Swinging is a natural way to stimulate vestibular system, which is the first sensory-system that starts functioning in the course of early development [1]. Vestibular system has complex network with diverse pathways, including the cortical and subcortical structures of central nervous system [2]. Vestibular system consists of afferent and efferent connections with most of the brain structures involved in regulation of stress, sleep and cognition [2]. Hippocampus is the area of continued neurogenesis, where new neurons are formed throughout the life [3]. Several studies have reported evidence for hippocampal networks and vestibular lesions leading to impairment in spatial memory in humans [4–6]. Vestibular dysfunction can lead to depression, anxiety, postural incoordination, occulo-motor changes and behavioural changes [7]. It was reported that vestibular stimulation improves cognitive functions [8].
Most of the students in higher education experience stress due to demands of very competitive college life [9]. High levels of stress can negatively affect cognitive functions (attention, comprehension, thinking, memory, problem solving, etc.,) and decrease academic performance in college students [10,11]. Though several methods are developed to alleviate stress among college students, minimum attention is given to arrange swings in the campus and providing adequate time to the students to use the swing. Most of the students reported that swings are a nice way to enjoy fresh breeze. Swinging in a green space will provide students an opportunity to alleviate stress [8]. Swinging on a swing is a natural method of stimulating vestibular system. Vestibular stimulation may alleviate stress by inhibiting hypothalamo- pituitary adrenal-axis and sympathetic- adreno medullary axis [9–12]. Vestibular stimulation decreases heart rate and blood pressure within normal limits through vagal stimulation [13]. The present study was aimed to assess the evidence for stress alleviating effects of vestibular stimulation among college students.
Materials and Methods
Study Design: Experimental (pre and post with control) design.
Participants, inclusion and exclusion criteria: Sixty male and female college students were a part for this research. The study was approved by Institutional Ethics committee (10th Jan 2014) of Little Flower Hospital and Research Center. After obtaining written informed consent from all the participants, they were randomly assigned to control (females (n=17), males (n=13) and intervention groups (females (n=24), males (n=6) by random numbers generated by computer. A detailed medical history was obtained from all participants and they underwent a standard physical examination, which enabled us to exclude individuals involved in drug/alcohol abuse, and those taking any kind of medication or suffering from any somatic or mental disorders. The selected female students were having regular menstrual cycles for at least 6 months prior to this study. Students with a history of use of corticosteroids in the past year, students with a history of antidepressant medication and students on hormone supplements including oral contraceptives and ear infections or any vestibular disturbances were excluded from the study.
Laboratory setting: The present study was conducted at Department of Physiology, Little Flower Institute of Medical Sciences and Research Centre (LIMSAR), Angamaly, Kerala, India. After recording baseline (pre-intervention) scores, intervention was given to the participants for 28 days and post- intervention scores were recorded and compared to observe effect of our intervention.
Vestibular stimulation: Vestibular stimulation was achieved by swinging on a swing, according to their comfort. (Back to front direction) [14,15].
Assessment of depression, anxiety and stress: Assessment of depression, anxiety and stress was done by using standard questionnaires after obtaining permission to reproduce the questionnaires and in consultation with psychiatrist [16,17].
State-Trait Anxiety Inventory for AdultsTM: The STAI inventory comprises of state and trait forms, to assess anxiety levels. Each form consists of 20 questions with total scores that range from a minimum of 20 to a maximum of 80. Anxiety scores ≤ 40 were considered as low anxiety while a score of > 40 were considered as high anxiety. License obtained from Mind Garden, Inc., to reproduce State-Trait Anxiety Inventory for AdultsTM in our research.
Depression Anxiety Stress Scale (DASS): DASS is a 42 item questionnaire designed to assess depression, anxiety and stress levels.
The students’ Stress Questionnaire: The students stress questionnaire is a standard questionnaire, designed by Ministry of Social Security, National Solidarity and Reform Institutions, to assess stress levels in students (www.gov.mu/portal/sites/suicideprevention/file/student).
Assessment of Cognition
Verbal and spatial memory test: Verbal and spatial memory test is a standardized test to assess cognition levels by assessing spatial and verbal memory scores [18,19].
Assessment of cardio-respiratory parameters: Blood pressure was recorded by using Diamond digital sphygmomanometers (BPDG024) and P02, pulse rate was recorded by using pulse oximeter (EDAN H100B) respiratory rate was measured manually [14,20].
The Pittsburgh Sleep Quality Index (PSQI): It is a standardized instrument to assess quality of sleep through seven components of sleep. Permission obtained to use the questionnaire for our research [21].
The Epworth Sleepiness Scale (ESS): It is a standard questionnaire to assess observe abnormal excessive day time sleepiness [22].
Quality of Life: The WHO-QOL BREF is a standardized questionnaire developed as a cross-culturally comparable tool to assess an individual’s perceptions in the context of their culture and value systems, their personal goals, standards and concerns [23]. Twenty six questions are used to measure the quality of life in four domains––physical, psychological, social and environmental. Each item is scored on a five-point Likert scale [24].
Haematological parameters: Bleeding time was estimated by duke method and clotting time was estimated by capillary tube method. Increase in cortisol causes atrophy of all lymphoid tissues and decreases output of lymphocytes. Cortisol decreases eosinophils, lymphocytes and monocytes and increases red blood cells and platelets [25–27].
Autonomic Function Test
Blood pressure –response to standing: It was reported that stress can modulates autonomic functions in students [28]. The test was performed by measuring the blood pressure in lying position and again in standing position. The postural fall in blood pressure was taken as difference between the systolic blood pressure lying and systolic blood pressure standing [29].
Statistical Analysis
Data is represented as Mean±SD and were analysed using SPSS 20.0. Statistical tests applied are Two-Way ANOVA and Bonferroni posttests. The p-value <0.05 was taken as significant.
Results
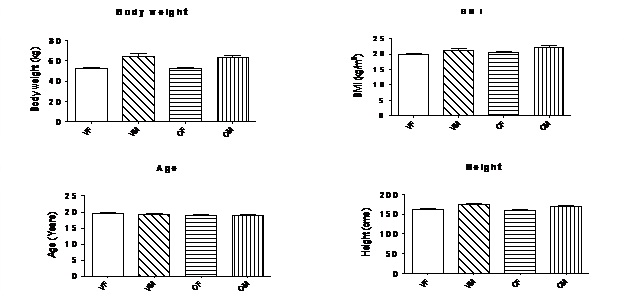
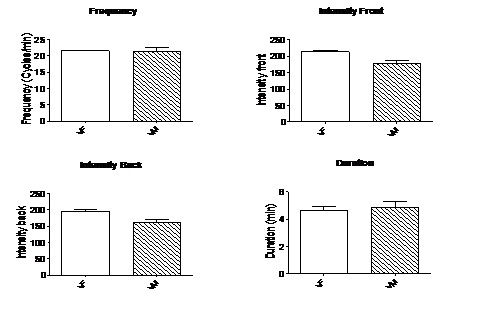
Results were presented in [Table/Fig-1,2,3,4,5,6,7,8,9 and 10]. [Table/Fig-1] presents demographic information and [Table/Fig-2] presents mean frequency, intensity and duration of vestibular stimulation. [Table/Fig-3,4,5,6,7,8,9 and 10] presents variations in different parameters before and after vestibular stimulation.
Age, Body weight, height and BMI of participants (VF- vestibular group females, VM-Vestibular group males, CM- Control group males, CF- Control group females).
Mean frequency, intensity, duration of vestibular stimulation. (Frequency, intensity, duration was measured manually as previously described) [15].
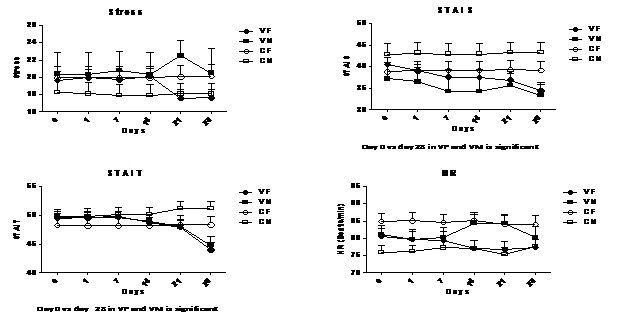
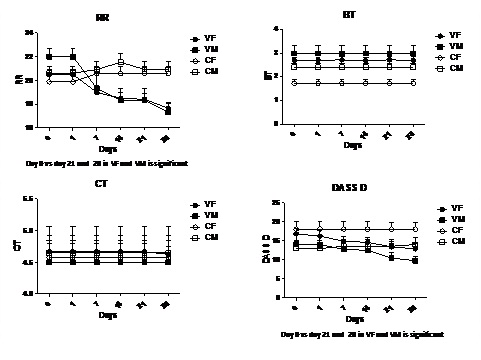
Student’s Stress, STAI S, STAI T scores, Heart rate in participants before and after vestibular stimulation. (VF- vestibular stimulation group females, VM- Vestibular stimulation group males, CM- control group males, CF- control group females).
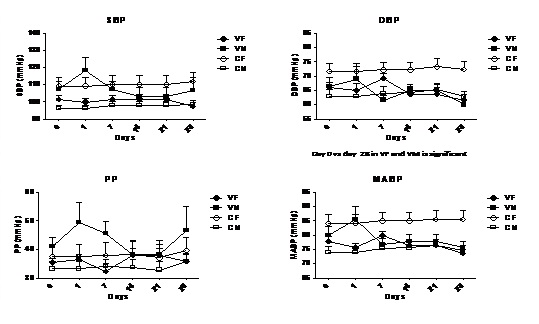
Blood pressure changes in participants before and after vestibular stimulation.
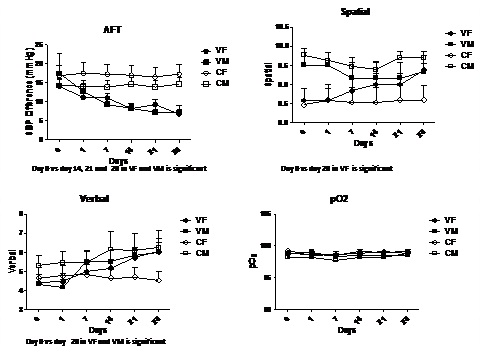
Autonomic function test values, spatial and verbal memory test scores and Po2 levels before and after vestibular stimulation.
Respiratory rate, bleeding time, clotting time and DASS depression scores before and after vestibular stimulation.
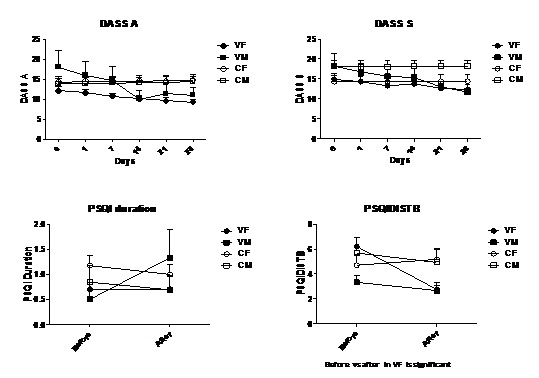
Anxiety, stress scores, PSQI duration of sleep, PSQI sleep disturbance before and after vestibular stimulation. (DASS A- DASS anxiety scores, DASS S- DASS stress scores, PSQI DISTB- PSQI sleep disturbance).
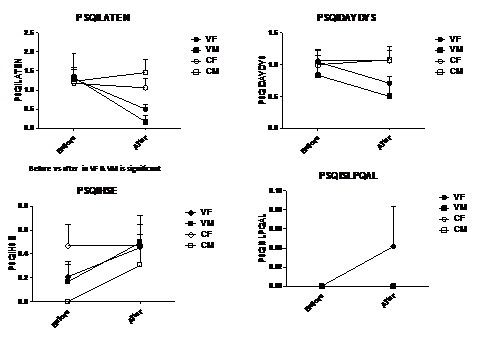
PSQI sleep latency, PSQI day dysfunction due to sleepiness, PSQI efficiency, PSQI overall sleep quality before and after vestibular stimulation.
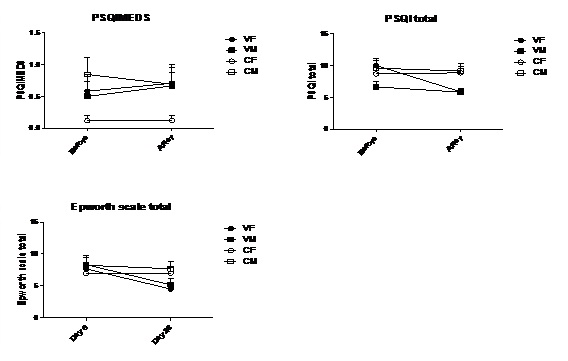
PSQI need medicines to sleep, PSQI total score, Epworth sleepiness scale total score before and after vestibular stimulation.
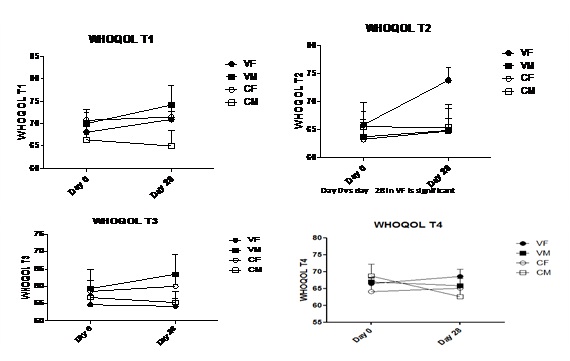
WHO QOL BREF transformed scores before and after vestibular stimulation (T1- physical health, T2-psychological, T3-social relationships, T4-Environment).
Student’s stress scores and heart rate did not change in vestibular group after vestibular stimulation. STAI S and STAI T scores were significantly different in vestibular and control groups on 28th day of vestibular stimulation. STAI S and STAI T scores of day 0 Vs day 28 in vestibular female (VF) and vestibular male (VM) were statistically significant [Table/Fig-3]. Systolic blood pressure, pulse pressure was within normal limits in vestibular group after vestibular stimulation. Diastolic blood pressure and mean arterial blood pressure were significantly decreased and remained within normal limits in vestibular group on 28th day of vestibular stimulation. Diastolic blood pressure significantly decreased in vestibular female (VF) and vestibular male (VM) when compared with baseline values. Postural fall in blood pressure was significantly different between control and vestibular groups on 14, 21, 28 days of vestibular stimulation. Postural fall in blood pressure of day 0 Vs day 14, 21 and 28 in VF and VM was significantly different [Table/Fig-4,5].
Spatial and verbal memory scores were not significantly different between control and vestibular groups before and after vestibular stimulation. Spatial memory scores of day 0 Vs day 28 in VF was significantly increased. Verbal memory scores of Day 0 Vs day28 in VF and VM were significantly increased. Po2 was not significantly different between control and vestibular groups before and after vestibular stimulation [Table/Fig-5].
Respiratory rate was significantly decreased in vestibular groups on days 7, 14, 21 and 28 when compared with control group. Respiratory rate of day 0 Vs day 21 and 28 in VF and VM was significantly decreased. Bleeding but not clotting time was significantly different between control and vestibular groups before and after vestibular stimulation [Table/Fig-6].
DASS depression scores were not significantly different between control and vestibular groups before and after vestibular stimulation. DASS depression scores of day 0 Vs day 21 and 28 in VF and VM was significantly different. DASS anxiety scores were significantly decreased in vestibular group on 14, 21, 28 days. DASS stress scores were not significantly different between control and vestibular groups before and after vestibular stimulation [Table/Fig-6,7].
PSQI sleep disturbance, PSQI sleep latency, PSQI total score was significantly decreased in vestibular after vestibular stimulation, which indicates improvement in sleep quality. PSQI sleep disturbance was significantly decreased before Vs after in VF. PSQI sleep latency was significantly decreased before Vs after in VF and VM groups. Epworth sleepiness scale total score was significantly decreased in vestibular group after vestibular stimulation, which indicates decrease in excessive daytime sleepiness [Table/Fig-7,8 and 9].
WHO QOL BREF transformed scores of four domains were not significantly different between control and vestibular groups before and after vestibular stimulation. WHO QOL BREF T2 (psychological domain) of Day 0 Vs day 28 in VF is significantly increased [Table/Fig-10].
Discussion
In our study significant decrease in salivary cortisol, autonomic and haematological parameters were observed following controlled vestibular stimulation [14]. We have attributed these beneficial effects of vestibular stimulation to inhibition of stress axes. However in the present study we have did not observed any change in student’s stress scores, DASS depression and stress scores, which may be due to short term vestibular stimulation.
It was reported that balance control and anxiety are closely linked [8]. Vestibular training may reduce some forms of anxiety, while cognitive and behavioural therapy of anxiety improves balancing performance [30]. Our study concurs with previous studies, as we have observed significant decrease in STAI S and STAI T scores and DASS anxiety scores following vestibular stimulation. Earlier studies reported that heart rate, blood pressure decreased following vestibular stimulation [31]. In the present study we have observed significant decrease in diastolic pressure and mean arterial blood pressure in vestibular group when compared to control group.
Previous researchers testified that anatomical connections exist between vestibular and autonomic nuclei [32]. Vestibular lesions modulated autonomic functions in humans and animals [33]. In the present study, systolic blood pressure difference in sitting and standing postures was significantly different in vestibular group when compared to control group. Vestibular system is connected with the brain areas related to cognition and bilateral vestibular lesion and can influence defects in spatial memory [34]. Our previous study categorically confirms that caloric vestibular stimulation with hot water, enhances cognition [35]. However, in the present study we observed only gradual improvement in spatial and verbal memory test scores. Vestibular stimulation modulates abdominal (expiratory) and phrenic (inspiratory) nerves activity [36]. Electrical or natural stimulation of the vestibular system results in changes in blood pressure and respiratory motor output and helps to maintain homeostasis during movement [37]. In the present study we have observed significant decrease in the respiratory rate in vestibular group when compared with control group. Although no significant change in p02 was observed. Also, bleeding but not clotting time was significantly different in control and vestibular groups before and after vestibular stimulation, hence short-term Vestibular stimulation may not have significant influence on bleeding and clotting time.
It is our routine day experience that motion promotes sleep as we become sleepy in boats, planes and cars [38]. It was reported that vestibular stimulation has positive impact on sleep [39–41]. Our study provides further evidence that vestibular stimulation improves sleep quality as PSQI total score and Epworth sleepiness score was decreased significantly after vestibular stimulation. Indeed vestibular stimulation improves quality of life in patients with benign paroxysmal positional vertigo, irrespective of age and gender [42]. Our study concurs with earlier findings that we have observed marginal improvement in all four domains of WHO QOL BREF.
Limitations and Future Perspectives
The study sample size was small and duration of intervention was short. In our future studies, we plan to increase sample size and long-term intervention.
Conclusion
Our study provides preliminary evidence that vestibular stimulation can be used for stress management in students. We recommend further detailed study with higher sample size and long-term vestibular stimulation to improve impact of this practically applicable intervention to reduce stress.