Forgotten Vaginal Foreign Body Presenting as Cervical Dystocia
Sonia Chawla1, Anshuja Singla2, Charu Chandra3, Swati Falodia4
1 Senior Resident, Department of Obstetrics & Gynecology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
2 Assistant Professor, Department of Obstetrics & Gynecology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India.
3 Senior Resident, Department of Obstetrics & Gynecology, S.P. Medical College, Bikaner, Rajasthan, India.
4 Associate Professor, Department of Obstetrics & Gynecology, S.P. Medical College, Bikaner, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sonia Chawla, Senior Resident, Department of Obstetrics & Gynecology, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi-110095, India.
E-mail: drsonia0685@gmail.com
Generally encountered in paediatrics age group, vaginal foreign body is a rare presentation in gynaecological clinics. Inserted as a part of sexual abuse, gratification or psychiatric disorder, these foreign bodies can present with a varied symptomatology. We report a case of 22-year-old female, a victim of domestic violence, who had a foreign body inserted in the vagina which was forgotten. Later it was discovered when she presented at term with cervical dystocia.
Domestic violence, Sexual abuse
Case Report
A 22-year-old unbooked, primigravida at term presented to gynaecological emergency of a tertiary care hospital in Bikaner, Rajasthan, India with labour pains for 2 days and foul smelling discharge per vaginum for 1 day.
General physical examination was normal. Uterus was term size with cephalic presentation, contracting intermittently and fetal heart was 136 bpm. On per speculum examination, yellowish discharge was present. On per vaginum examination, cervix was 3 cm dilated, partially effaced, vertex was at -3 station. A ring shaped hard mass, embedded in wall of cervix was felt through os. There was a foul smelling discharge. A provisional diagnosis of foreign body in cervix was made but on further questioning no positive history was revealed. All mandatory antenatal investigations were sent and a vaginal swab was taken and appropriate parenteral antibiotics in the form of injection ceftriaxone (500 mg) and injection metrogyl (100 ml) were started. No radiological examination was done as the patient was already in active labour. Same antibiotics were continued as per the culture/sensitivity report of the vaginal swab obtained later on.
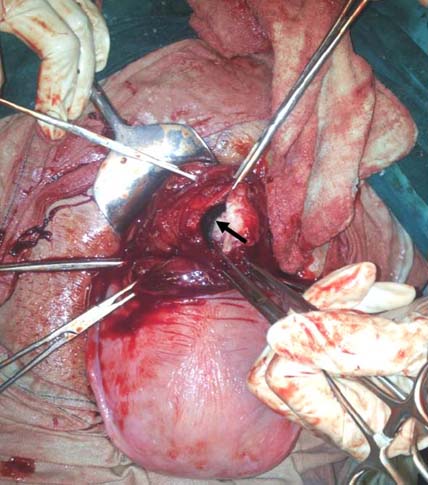
Removal of foreign body was attempted vaginally but was unsuccessful as it was deeply embedded and was painful. After a trial of labour for 2 hours patient was taken for emergency caesarean section in view of cervical dystocia. Intraoperatively, a ring like tubular structure was present up till lower uterine segment with decidua grown over it [Table/Fig-1].
Foreign body seen through uterine incision.
An incision was given over the same and a plastic cap of about 5x3 cm was dissected out [Table/Fig-2].

There was no ulceration, calcification or fistula formation below the foreign body.
Postoperatively, she revealed the history of domestic violence and sexual abuse by her husband. A cap was inserted by him into her vagina around one and half year back suspecting infidelity which she told was removed. She suffered recurrent episodes of vaginal discharge and was prescribed multiple courses of antibiotics without any significant improvement. No imaging studies were ever done. Patient was discharged on post op day 8 in satisfactory condition and was advised follow up. At 6 weeks, on-per speculum examination anatomy of cervix and vagina was apparently normal and vaginal discharge was healthy.
Discussion
Vaginal foreign bodies are a complaint occasionally encountered in gynaecology clinic and emergency department. Amazingly, large variety of foreign bodies has been found in the vagina. Generally the problem is encountered in paediatric and adolescent age group but adults may also seek care for vaginal foreign bodies which may have been placed intentionally for sexual gratification, sexual abuse, psychiatric disorder, medical treatment (pessaries, intra uterine contraceptive devices), or inadvertently for example toilet papers, tampons etc. A variety of symptoms may result from foreign body in vagina commonest being foul smelling vaginal discharge, bleeding, dyspareunia, pelvic pain, pressure, vesicovaginal fistula or rarely may be asymptomatic and forgotten [1–4].
Intimate partner violence and sexual abuse is a major public health problem that is grossly under reported. Survivors can suffer long term sequelae like depression, anxiety, psychological and physical disabilities. Cases with foreign body in vagina are not common but do occur.
A foreign body of long duration stimulates vaginal mucosa causing local infection and malodorous vaginal discharge, which is the most common symptom. This may eventually lead to abrasion, pressure necrosis, ulceration, calcification and fistula formation. A detailed history, vaginal examination and radiological assessment such as x-ray, ultrasound, MRI and vaginoscopy may be helpful in making a diagnosis. In all the cases object should be removed as early as possible either directly or under anaesthesia.
Singh et al., reported a vesicovaginal fistula in a young girl as a result of insertion of a plastic cap [3]. Chopra et al., reported a similar case of vaginal foreign body, which was a hexagonal cap removed later in a 50-year-old patient who was diagnosed as carcinoma cervix elsewhere and was referred for the same [5]. Balci et al., reported two plastic balls extracted from a postmenopausal woman which were inserted as a means of contraception and to treat uterine prolapse which were forgotten [6].
Conclusion
Whenever a patient presents with longstanding history of vaginal discharge of unknown aetiology possibility of foreign body should be kept in mind. Early removal can save a lot of morbidity to women. A sensitive and encouraging approach would probably help these women to come out of menace of domestic violence and prevent physical and psychological morbidity.
Ethical Concerns
There were no ethical concerns as the patient consented to the publication of the manuscript and nowhere direct patient information and identity has been revealed in the manuscript.
[1]. Malatyalioglu E, Alper T, Kokoo An intravaginal foreign body of over 25 years’ durationActa Obstet Gynaecol Scand 2000 79:616-17. [Google Scholar]
[2]. Nwosu EC, Rao S, Igweike C, Hamed H, Foreign objects of long duration in the adult vaginaJ Obstet Gynaecol 2005 25(7):737-39. [Google Scholar]
[3]. Singh RR, Ghotra HS, Garg R, Kaur R, An unusual foreign body in the vagina producing vesicovaginal fistulaJ Dent Med Sci 2013 6:72-73. [Google Scholar]
[4]. Puneet Khanna A, Khanna AK, Intravaginal foreign body—a rare cause of large bowel obstructionJ Indian Med Assoc 2002 100(11):671 [Google Scholar]
[5]. Chopra S, Singh Y, Magon N, Case of intravaginal foreign bodyMJAFI 2010 66:266-68. [Google Scholar]
[6]. Balci O, Goktepe H, Mahmoud AS, Acar A, Intravaginal foreign bodies placed in the vagina to treaty uterine prolapsed retained for 35 yearsTaiwan J Obstet Gynaecol 2009 48:431-33. [Google Scholar]