Hypertonic Dextrose Injection for The Treatment of a Baker’s Cyst
Ferdi Yavuz1, Sibel Kibar2, Birol Balaban3
1 The Clinic of Physical Therapy and Rehabilitation, The Fizyocare Medical Center, Ankara-Turkey.
2 The Clinic of Physical Therapy and Rehabilitation, The Fizyocare Medical Center, Ankara-Turkey.
3 Professor, Department of Physical Therapy and Rehabilitation, Faculty of Health Sciences, European University of Lefke, Lefke-Mersin, Turkey; The Clinic of Physical Therapy and Rehabilitation, The Fizyocare Medical Center, Ankara-Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ferdi Yavuz, The Clinic of Physical Therapy and Rehabilitation, The Fizyocare Medical Center Ankara-Turkey. E-mail : ferdiyavuz@yahoo.com
We present extremely rare and interesting case of a Baker’s cyst treated with hypertonic dextrose injection. A 54-year-old female patient had a Baker’s cyst which was diagnosed by an ultrasonography. After the failure of the two-weekly conservative treatment, we injected hypertonic dextrose (25%) into her right knee joint for the treatment of a Baker’s cyst. Two weeks after the injection, the patient reported improvement in posterior knee pain, and an US showed a resolution of the posterior knee cyst. Certainly hypertonic dextrose injection for the treatment of a Baker’s cyst appears to be a reasonable treatment option. Further studies are needed in order to elucidate the efficacy of hypertonic dextrose injection in the treatment of Baker’s cysts.
Knee joint, Musculoskeletal ultrasound, Popliteal cyst
Case Report
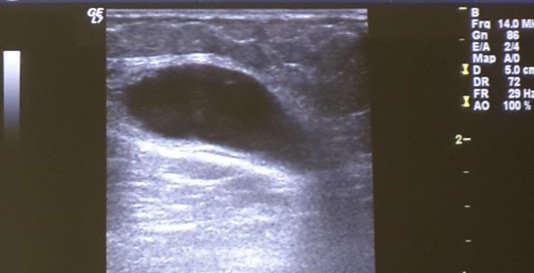
A 54-year-old female patient was admitted to the our outpatient clinic with complaints of popliteal pain and swelling in her right knee. Her symptoms had began two weeks prior to admission. There was no history of any previous injury to the affected leg. On physical examination the patient had a swelling and tenderness with palpation over the popliteal fossa. Her right knee flexion was mildly restricted due to the pain and popliteal cyst. No laboratory evidence of infection and rheumatological disorder was identified. The erythrocyte sedimentation rate was 12 mm/hr (normal value: 0-20 mm/hr), C- reactive protein was 2.6 mg/L (normal value 0-5 mg/L), serum uric acid level was 3.26 mg/dL (normal value 0-6 mg/dL), white blood cell count was 5600 (normal value 4000-11000), rheumatoid factor level was 12 IU / mL (normal value 0-20 IU / mL). An ultrasound examination showed a cystic mass located in the popliteal fossa [Table/Fig-1]. The cyst was measured to be 3.6 X 2.4 (axial dimension) X 3.0 cm (craniocaudal dimension). The patient was diagnosed as having a Baker’s cyst based on the clinical, laboratory and radiologic findings. She was ordered to use analgesic and anti-inflammatory drugs, and to apply coldpack over the popliteal fossa. However, the patient showed no respond to the two-weekly conservative treatment. Thus, we decided to inject hypertonic dextrose into her right knee joint for the treatment of a Baker’s cyst.
Pre-injection ultrasound imaging.
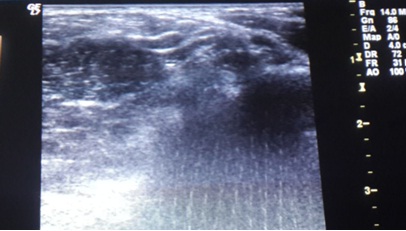
With informed consent, we began a single-dose injection of 25% dextrose without draining a Baker’s cyst. “Prolotherapy” of the Baker’s cyst with 25% dextrose solution was performed as described by Hemwall et al ., [1]. A 10 mL of a solution that was prepared with 5 mL of 50% dextrose, 4 mL of 0.9% NaCl, and 1 mL of 2% lidocaine was injected intraarticular through a lateral infrapatellar approach. Two weeks after the injection, the patient reported improvement in posterior knee pain, and an ultrasound showed almost complete resolution of the posterior knee cyst with a size of 0.6 X 0.5 (axial dimension) X 0.4 cm (craniocaudal dimension) [Table/Fig-2]. At the 6 month follow-up, the popliteal cyst was not observed again.
Ultrasound imaging at 2 weeks after the injection.
Discussion
Baker’s cyst is defined as swelling of gastrocnemius-semimembranosus bursa [2]. Baker’s cyst can cause pain and palpable mass at popliteal fossa, and decreased range of motion. Baker’s cyst is often secondary to osteoarthritis, rheumatoid arthritis and juvenile rheumatoid arthritis. Since it is important to exclude other differential diagnoses such as lipoma, aneurysm of popliteal artery and soft tissue tumour, imaging studies are recommended to diagnose a Baker’s cyst [3]. An ultrasonography is a very helpful imaging technique in the evaluation of the popliteal cysts.
In daily practise, corticosteroid injections into the knee joint are frequently used in the treatment of a Baker’s cyst. Although corticosteroid injections can reduce the size of the cyst, steroids can actually cause the deterioration of cartilage in the joint [4]. So that, alternative treatment options should be offered to the patients with a Baker’s cyst. When we searched literature for the alternative treatment options, we found dextrose prolotherapy of a Baker’s cyst [5]. In this case study, dextrose prolotherapy seemed to be an effective treatment for a Baker’s cyst. We decided to inject hypertonic dextrose into the knee joint for the treatment of a Baker’s cyst.
In this paper we present extremely rare and interesting case of a Baker’s cyst treated with hypertonic dextrose injection.
Recent studies showed that intra-articular steroid injections have been shown to be effective in relieving pain and in reducing cyst volume for the patient with symptomatic Baker cysts [6–8]. However, steroids can actually cause the deterioration of cartilage in the joint [4]. The idea of protecting knee cartilage directed us in applying a different therapeutic approach. In our case intraarticular injection of hypertonic dextrose was applied for the treatment of a Baker’s cyst. The cyst was resolved completely in 2 weeks after the injection.
In previous study ethanol sclerotherapy has been tried, and author’s suggested that ethanol sclerotherapy can be the treatment of choice for Baker’s cyst [9]. Among the 6 patients with Baker cysts, only one patient showed recurrence of a Baker’s cyst in follow-up period. In another case report, the Baker’s cyst was first completely drained, and then the patient was injected with three intra-articular injections of 12.5% dextrose mixed with sodium morrhuate. The Magnetic Resonance Imaging (MRI) confirmed that the Baker’s cyst resolved in 4 months after the injection [5]. In contrast to the previous case report, we didn’t have drainage of the Baker’s cyst before the intraarticular injection, and 25% dextrose solution was given only once.
The effect of dextrose prolotherapy on knee is still not clear [10]. Synovial fluid is being secreted and absorbed continualy in joint by synovium and synovial lining [11]. Glucose level of synovial fluid is determined by facilitated diffusion of glucose from blood to synovia to maintain the glucose levels according to plasma glucose levels. It was reported that at 3 hours after a meal glucose level of synovial fluid is higher than serum [12]. Therefore glucose is a non-stop changing substance in synovial fluid. Additionally, water is one of the prominent constutient of synovial fluid [13]. After the hypertonic dextrose injection into the knee joint, synovial fluid in intraarticuler cavity has been become more hypertonic than synovial fluid in Baker’s cyst. It can be thought that this hypertonicty determined the movement of water from Baker’s cyst cavity to intraarticular space.
Ultrasound is a very helpful and non-invasive imaging technique in the evaluation of popliteal cysts. On ultrasound, Baker’s cysts are generally anechoic or hypoechoic and show posterior acoustic enhancement. Ultrasound has been shown to be highly accurate and comparable to MRI in the imaging of popliteal cysts [14–18].
Conclusion
In summary, a rare case of a Baker’s cyst treated with hypertonic dextrose injection was presented herein. Certainly hypertonic dextrose injection for the treatment of a Baker’s cyst appears to be a reasonable treatment option. Further studies are needed in order to elucidate the efficacy of hypertonic dextrose injection in the treatment of Baker’s cysts.
[1]. Hackett GS, Hemwall GA, Montgomery GA, Ligament and Tendon Relaxation—Treated by Prolotherapy 1991 5th edOak Park, IL [Google Scholar]
[2]. Wigley RD, Popliteal cysts: variations on a theme of BakerSemin Arthritis Rheum 1982 12:1-10. [Google Scholar]
[3]. Choi YJ, Kang JH, Kang GH, Choi SJ, Osteochondrolipoma Presenting as a Popliteal CystClin Orthop Surg 2015 7(2):264-68. [Google Scholar]
[4]. Hauser RA, The deterioration of articular cartilage in osteoarthritis by corticosteroid injectionsJournal of Prolotherapy 2009 1(2):107-23. [Google Scholar]
[5]. Centeno CJ, Schultz J, Freeman M, Sclerotherapy of Baker’s cyst with imaging confirmation of resolutionPain Physician 2008 11(2):257-61. [Google Scholar]
[6]. Acebes JC, Sánchez-Pernaute O, Díaz-Oca A, Herrero-Beaumont G, Ultrasonographic assessment of Baker’s cysts after intra-articular corticosteroid injection in knee osteoarthritisJ Clin Ultrasound 2006 34:113-17. [Google Scholar]
[7]. Bandinelli F, Fedi R, Generini S, Porta F, Candelieri A, Mannoni A, Longitudinal ultrasound and clinical follow-up of Baker’s cysts injection with steroids in knee osteoarthritisClin Rheumatol 2012 31(4):727-31. [Google Scholar]
[8]. Köroğlu M, Callıoğlu M, Eriş HN, Kayan M, Cetin M, Yener M, Ultrasound guided percutaneous treatment and follow-up of Baker’s cyst in knee osteoarthritisEur J Radiol 2012 81(11):3466-71. [Google Scholar]
[9]. Fukumoto K, Kojima T, Tomonari H, Kontani K, Murai S, Tsujimoto F, Ethanol injection sclerotherapy for Baker’s cyst, thyroglossal duct cyst, and branchial cleft cystAnn Plast Surg 1994 33(6):615-19. [Google Scholar]
[10]. Hashemi M, Jalili P, Mennati S, Koosha A, Rohanifar R, Madadi F, The Effects of Prolotherapy With Hypertonic Dextrose Versus Prolozone (Intraarticular Ozone) in Patients With Knee OsteoarthritisAnesth Pain Med 2015 5(5):e27585 [Google Scholar]
[11]. Levick JR, McDonald JN, Fluid movement across synovium in healthy joints: role of synovial fluid macromoleculesAnn Rheum Dis 1995 54(5):417-23. [Google Scholar]
[12]. Alice Faryna, Kim Goldenberg, Joint fluid. In: Walker HK, Hall WD, Hurst JW, editorsClinical Methods: The History, Physical, and Laboratory Examinations 1990 3rd editionBostonButterworths:773-776. [Google Scholar]
[13]. Miroslav Petrtyl, Jaroslav Lisal, Jana Danesova, Biomechanical Properties of Synovial Fluid in/Between Peripheral Zones of Articular Cartilage. In: Rosario Pignatello. edBiomaterials - Physics and Chemistry 2011 InTechpp.207-224 ISBN: 978-953-307-418-4 [Google Scholar]
[14]. Ward EE, Jacobson JA, Fessell DP, Hayes CW, van Holsbeeck M, Sonographic detection of Baker’s cysts: comparison with MR imagingAJR Am J Roentgenol 2001 176:373-80. [Google Scholar]
[15]. Subhas N, Bui KL, Sundaram M, Ilaslan H, Recht MP, Incidental tumor and tumor-like lesions around the kneeSemin Musculoskelet Radiol 2009 13:353-70. [Google Scholar]
[16]. Beaman FD, Peterson JJ, MR imaging of cysts, ganglia, and bursae about the kneeMagn Reson Imaging Clin N Am 2007 15:39-52. [Google Scholar]
[17]. Marra MD, Crema MD, Chung M, MRI features of cystic lesions around the kneeKnee 2008 15:423-38. [Google Scholar]
[18]. Acebes JC, Sánchez-Pernaute O, Díaz-Oca A, Herrero-Beaumont G, Ultrasonographic assessment of Baker’s cysts after intra-articular corticosteroid injection in knee osteoarthritisJ Clin Ultrasound 2006 34:113-17. [Google Scholar]