Major Protein of Carcinoembryonic Antigen Gene Family - CD66c, A Novel Marker in Colon Carcinoma
Suma M Nataraj1, Chaitra Linganna Prema2, Manjunath Gubbanna Vimalambike3, Sheeladevi Chandakavadi Shivalingaiah4, Shivakumar Sundaram5, Anjali Pradeep Kumar6, Ananda Kuruvatti Math7, Akila Prashant8
1 Professor and Head, Department of Biochemistry, Centre of Excellence in Molecular Biology and Regenerative Medicine, JSS Medical College, JSS University, Mysore, Karnataka, India.
2 Student, Department of Biochemistry, JSS Medical College, JSS University, Mysore, Karnataka, India.
3 Professor and Head, Department of Pathology, JSS Medical College, JSS University, Mysore, Karnataka, India.
4 Asssociate Professor, Department of Pathology, JSS Medical College, JSS University, Mysore, Karnataka, India.
5 Professor and Head, Department of Pathology, Mandya Institute Of Medical Sciences, Mandya, Karnataka, India.
6 Student, Department of Biochemistry, JSS Medical College, JSS University, Mysore, Karnataka, India.
7 Student, Department of Biochemistry, JSS Medical College, JSS University, Mysore, Karnataka, India.
8 Professor, Department of Biochemistry, Centre of Excellence in Molecular Biology and Regenerative Medicine, JSS Medical College, JSS University, Mysore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Akila Prashant, Centre of Excellence in Molecular Biology and Regenerative Medicine, Department of Biochemistry, JSS Medical College, JSS University, Mysore – 570015, Karnataka, India.
E-mail: akila.prashant@gmail.com
Introduction
In view of rising trend of the incidence of colorectal carcinoma in the Indian population due to adoption of western lifestyles and behaviours, we investigated the expression of the new emerging stem cell biomarker, CD66c in colorectal carcinoma of Indian origin.
Aim
To study the expression of CD66c in human colorectal carcinoma and to correlate level of marker expression with tumour staging.
Materials and Methods
This hospital based prospective study was conducted on 26 colorectal carcinoma patients in the age group of 20 years to 70 years. Surgically resected tumour specimens along with adjacent normal tissue were collected taking necessary precautions, paraffin embedded sections were prepared and used for histological and immunohistochemical analysis of CD66c.
Statistical analysis
Descriptive statistical measures like mean, standard deviation, percentage was applied. Other inferential statistical tests like Chi-square, Fisher’s-exact test and one-way ANOVA was applied to find out the association of CD66c with different stages. The difference were interpreted as statistically significant when p <0.05.
Results
CD66c showed differential expression with membrane positivity in normal colorectal epithelial cells and cytoplasmic expression in tumour cells. There was significant correlation between CD66c expression and tumour site (p=0.02) with colon carcinoma showing positive expression compared to the rectal carcinoma. There was no significant correlation between CD66c staining and tumour stage (p=0.947). No significant relationship was observed between CD66c expression and other clinicopathologic variables studied such as sex (p=0.552), age (p=0.713) and tumour grade (p=0.263).
Conclusion
CD66c can be specifically used for colon carcinoma and may be a novel marker in colon carcinoma stem cell isolation. The quantification of CD66c can be further verified by flow cytometry and RT-PCR. Further studies can be carried out using CD66c alone or in combination with other markers to develop cancer stem cell directed therapy.
Colorectal carcinoma, Immunohistochemistry, Indian population, CD66c
Introduction
Colorectal carcinoma is a global public health problem [1]. It is the fourth most common cancer in males and third in females [2] affecting both men and women equally [3]. It is the third leading cause of death [4]. It is primarily sporadic, 5 to 10% is constituted by heritable form [5].
According to World Health Organisation, 1,471,808 cases are diagnosed each year [6] and there are 65,000 deaths worldwide each year [7]. In 2015 alone 726,028 deaths have occurred from colorectal carcinoma [6]. Incidence is rising annually in developing countries [8] and also in most Asian countries [1]. Incidence is also increasing in economically transitioning countries due to high fat diet, smoking and physical inactivity [2].
Colorectal carcinoma is diagnosed at an advanced stage when conventional combination chemotherapy regimens have limited efficacy and are associated with significant toxicity. Also, high incidence of recurrence is reported in colorectal carcinoma because the slowly proliferating stem cells escape the chemotherapeutic regimen [9]. Cancer stem cells are more resistant to therapy than differentiated tumour cells. Identification of cancer stem cell is a crucial step, as they play an important role in tumour development and recurrence [10]. For this purpose, cell surface antigens are used to characterize different cell populations. The potential candidates to regulate proliferation, differentiation and cell death in colon are the genes which are turned on or off during colonic epithelia development. They also play a role in tumourigenesis when deregulated or mutated. With respect to this concept, Carcinoembryonic antigen family (CEA) is of emerging interest [11]. CEA family has 18 active genes located on long arm of chromosome 19. The main members of CEA family includes Carcinoembryonic antigen related cell adhesion molecule family member 6 (CEACAM 6), also known as CD66c or Non-Specific Cross Reacting Antigen (NCA), Biliary Glycoprotein (BGP, CD66a) and CEA gene family member 2 (CGM2) [12]. CD66c is of emerging cancer stem cell related biomarker in colorectal carcinoma as its silencing halts tumour growth in vivo [13]. CD66c is expressed on normal mucosal epithelia of colon [12] and also seen in normal lung, granulocytes and cancers of epithelial cell origin [14]. Very few studies have been done relating to CD66c. Three members which are co-expressed with CEA are CEACAM1, CEACAM6 and CEACAM7. CEACAM1 and CEACAM7 expression is down-regulated in colorectal carcinoma whereas, CEACAM6 expression is up-regulated in colorectal carcinoma compared to the normal mucosa [15].
In view of rising trend of the incidence of colorectal carcinoma in the Indian population this study was taken up to investigate the expression of new emerging stem cell biomarker CD66c in colorectal carcinoma of Indian origin. Since immunohistochemistry is an easily applicable and relatively fast and cheap procedure, we investigated the expression CD66c protein in colorectal carcinoma and paired normal tissue by immunohistochemistry, evaluated the possible alternations in their expression and associated our results with other classical clinicopathologic parameters.
Materials and Methods
Twenty six colorectal carcinoma patients, in the age group of 20 years to 70 years attending the surgery OPD and inpatient surgery ward were included in the study. The study was conducted for a period of one year from January 2014 to January 2015. Ethical committee clearance and written consent was taken from the patients before the commencement of the study. All patients were clinically evaluated preoperatively with chest X-ray, CT scan and abdominal ultrasound. Tumours were histologically classified as well differentiated, moderately differentiated or poorly differentiated adenocarcinomas using the WHO criteria [16] and clinical staging was based on Dukes classification. Description of the patient characteristics is summarized in [Table/Fig-1].
Clinical and pathological features of 26 patients with colorectal carcinoma.
| Variables | Total n = 26 |
|---|
| Sex | Male | 15 |
| Female | 11 |
| Age | 20-40years | 4 |
| 40-60years | 14 |
| >60years | 8 |
| Tumour staging | Stage-I | 6 |
| Stage-II | 10 |
| Stage -III | 10 |
| Duke staging | A | 6 |
| B | 10 |
| C | 10 |
| Tumour site | Colon | 12 |
| Rectum | 11 |
| Rectosigmoidal | 3 |
| Tumour grade | Well differentiated | 2 |
| Moderately differentiated | 22 |
| Poorly differentiated | 2 |
Cases of inflammatory bowel diseases, pre-malignant conditions of colon and who did not survive in the immediate postoperative period were excluded from the study. Patients who received preoperative chemotherapy or radiotherapy were also excluded from the study.
Immunohistochemical staining: Surgically resected tumour specimens along with adjacent normal tissue were collected taking necessary precautions, paraffin embedded sections were prepared and used for histological and immunohistochemical analysis. The slices were cut into 5μm sections and stained with Haematoxylin-Eosin (H&E) for histological evaluation.
Sections of 5μm from paraffin embedded slices that include the most representative area were chosen in each patient and used for immunohistochemical staining of CD66c. The sections were placed in an incubator for 2 hours at 80°C and then deparaffinized in xylene, rehydrated through graded ethanol solutions and immersed in a 0.3% hydrogen peroxide solution in methanol for 15 min to inhibit endogenous peroxidase activity. After washing with tris buffer saline (TBS), antigen retrieval was performed by placing the slides at 95°C for 20 min in a microwave oven and allowed to cool for 1 hour at room temperature. The slides were again washed three times with TBS, and nonspecific binding was blocked by pre-incubation with Power BlockTM reagent (HK083-5K; Biogenex, Fremont, CA, USA) for 10 min at room temperature. Each slide was then incubated for 2 hours at 4°C with primary anti-CD66c antibody (PAR6039; Neobiolab, Woburn, MA, USA) at a dilution of 1:300 in the blocking buffer. After washing the slides three times with TBS they were stained using Super SensitiveTM* Polymer-HRP detection system (QD400-60KE; Biogenex, Fremont, CA, USA) as per the manufacturer’s instructions. Briefly, sections were subsequently treated with Poly HRP reagent (HK519-06K; Biogenex, Fremont, CA, USA) for 30 min. Diaminobenzidine (DAB) was used as a chromogen followed by slight haematoxylin counterstaining. The slides were then dehydrated, cleared with xylene and mounted with Dibutyl phthalate xylene (DPX). Omission of the primary antibody served as negative control and tonsil was used as a positive control.
Semiquantitative analysis of slides
The IHC staining results were evaluated independently by two pathologists blinded to the patients clinical and pathologic information. Discrepancies of any kind between the pathologists were resolved by consensus. For CD66c, an intensity score was used to represent the average intensity of the positive cells with scores of -/+ (none or very faint intensity, at the limit of detection, in >80% of cells), + (weak in <50% of cells), ++ (intermediate in >50% of cells), and +++ (strong in >80% of cells).
Statistical Analysis
Statistical analysis was performed using microsoft excel 2010 and SPSS version 22. Descriptive statistical measures like mean, standard deviation, percentage was applied. Other inferential statistical tests like Chi-square and Fisher’s-exact test was applied. The difference were interpreted as statistically significant when p < 0.05.
Results
Twenty six colorectal carcinoma cases ranging from 20 to 70 years were included in the study. The mean age of patients was 52.88±13.5 years (15 males and 11 females). According to the tumour location, 12 were in the colon, 11 were in the rectum and 3 were in the recto-sigmoidal region. According to TNM staging, 6 cases were in stage I, 10 cases in stage II and 10 in stage III and as per Duke’s staging, 6 cases were in stage A, 10 in stage B and 10 in stage C. All the tumours were adenocarcinomas, 2 well differentiated, 22 moderately differentiated and 2 poorly differentiated [Table/Fig-1].
CD66c expression
CD66c expression was detected in 12 of 26 tumours (46.2%). CD66c expression was seen more in colon carcinoma compared with rectal carcinoma. The expression was seen in 9 of 12 colon carcinomas where as in rectal carcinoma only 2 were positive for CD66c out of 11 cases. Of these, 30.8% showed low expression (<50% of neoplastic cells), 15.4% showed moderate expression (51-80 % of neoplastic cells) and no cases showed extensive expression (>80% of neoplastic cells).
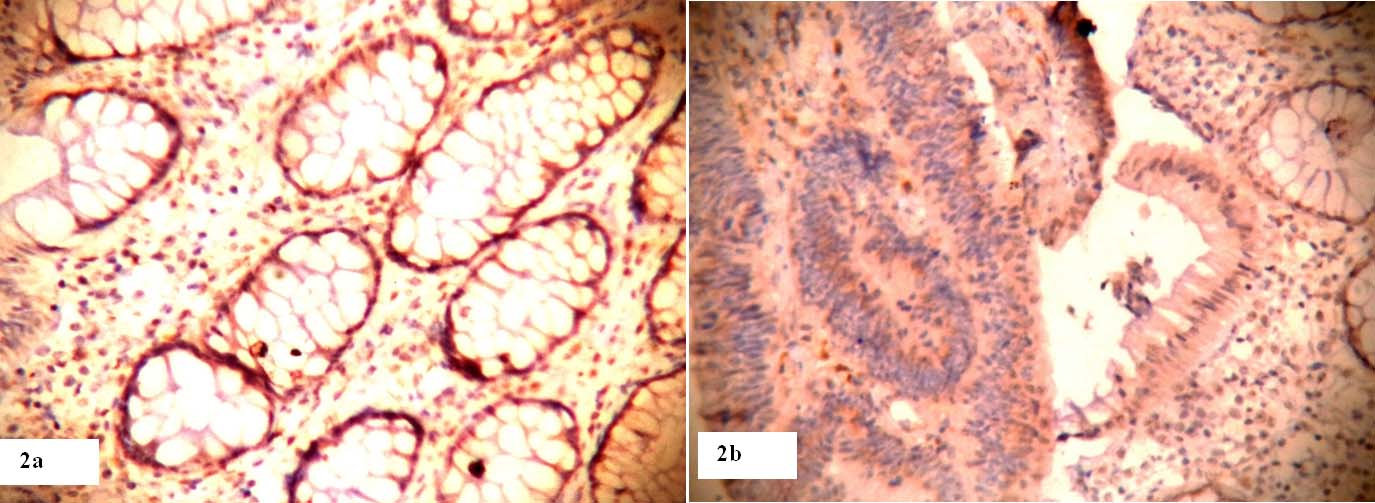
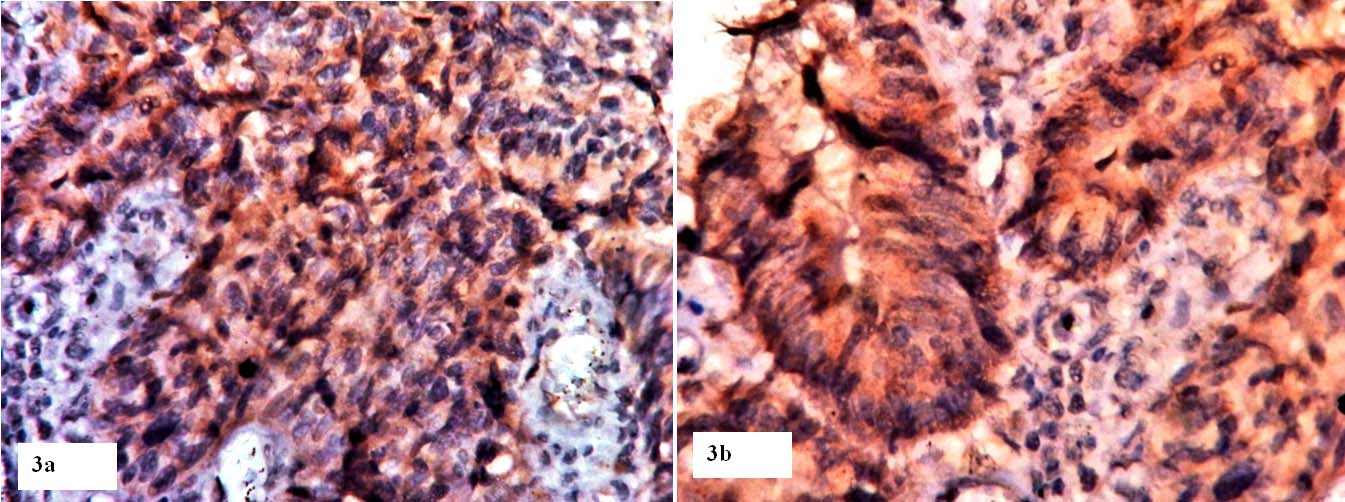
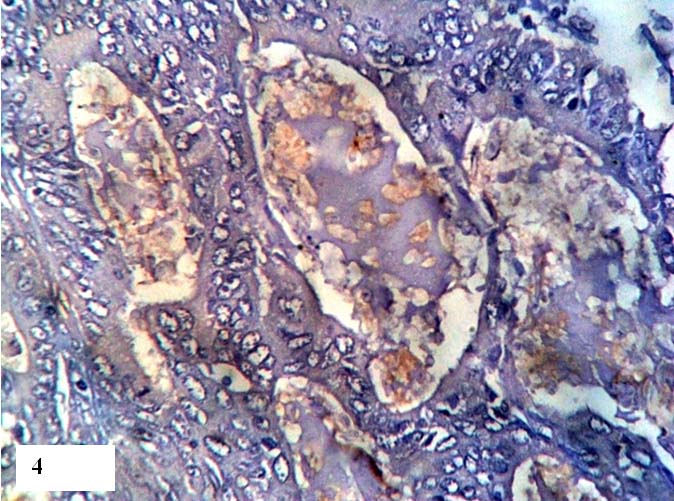
Different staining pattern were observed for CD66c. In normal colorectal mucosa, CD66c showed membrane positivity [Table/Fig-2a] where as in adenoma and colorectal carcinoma cytoplasmic expression was seen [Table/Fig-2b,3]. The intensity of CD66c marker expression showed a gradient increase from normal to adenoma to carcinoma. Faint intensity was observed in normal colorectal mucosa confined to membrane [Table/Fig-2a] and intermediate and strong intensity of CD66c marker expression in adenoma [Table/Fig-2b] and colorectal tumour cells [Table/Fig-3] respectively. In mucin secreting moderately differentiated adenocarcinoma, the mucin secretions took up the stain where as the tumour cells were negative for CD66c marker expression by immunohistochemistry [Table/Fig-4].
CD66c marker expression in normal colonic mucosa and adenoma (40x). In normal glands, CD66c staining was confined to membrane with faint intensity (a) where as in adenoma the staining was localized to cytoplasm (b). Nearly 50 to 80% adenoma have taken positivity with intermediate intensity (2+).
Moderately differentiated adenocarcinoma showing CD66c expression in nearly 50 to 80% tumour cells with strong intensity (2+) in 20x (a) and 40x (b).
In mucin secreting moderately differentiated adenocarcinoma, mucin secretions have taken up staining and tumour cells are negative for CD66c marker expression (20x).
CD66c expression and clinicopathological features
The relationship between CD66c expression and a range of clinicohistopathological variables is summarized in [Table/Fig-5]. There was significant correlation between CD66c expression and tumour site (p=0.02) with colon carcinoma showing positive expression compared to the rectal carcinoma. There was no significant correlation between CD66c staining and tumour stage (p=0.947). Also no significant relationship was observed between CD66c expression and other clinicopathologic variables studied such as sex (p=0.552), age (p=0.713) and tumour grade (p=0.263).
CD66c expression according to clinicopathologic parameters in CRC patients.
| Variables | CD66c Immunohistochemistry |
|---|
| Total | Neg-ative | <50% | 51-80% | >81% | Chi-square | p-value |
|---|
| Sex | Male | 15 | 7 | 6 | 2 | 0 | 1.489 | 0.552 |
| Female | 11 | 7 | 2 | 2 | 0 |
| Age | 20-40years | 4 | 3 | 1 | 0 | 0 | 2.119 | 0.713 |
| 40-60years | 14 | 8 | 4 | 2 | 0 |
| >60years | 8 | 3 | 4 | 1 | 0 |
| TNM staging | Stage-I | 6 | 4 | 1 | 1 | 0 | 1.541 | 0.947 |
| Stage-II | 10 | 5 | 3 | 2 | 0 |
| Stage -III | 10 | 5 | 4 | 1 | 0 |
| Duke staging | A | 6 | 3 | 2 | 1 | 0 | 1.541 | 0.947 |
| B | 10 | 6 | 2 | 2 | 0 |
| C | 10 | 5 | 4 | 1 | 0 |
| Tumour site | Colon | 11 | 2 | 5 | 4 | 0 | 11.63 | 0.02 |
| Rectum | 12 | 10 | 2 | 0 | 0 |
| Rectosigmoidal | 3 | 2 | 1 | 0 | 0 |
| Tumour grade | Well differentiated | 2 | 1 | 0 | 1 | 0 | 5.149 | 0.263 |
| Moderately differentiated | 22 | 12 | 8 | 2 | 0 |
| Poorly differentiated | 2 | 1 | 0 | 1 | 0 |
Foot Note: Chi-square / Fisher’s-exact test
Discussion
Despite many advances in therapeutics, still cancer is a major public health issue. All malignant cells cannot be eliminated even with standard chemotherapy. Efforts are being made to explain cancer pathogenesis and resistance to medication [17]. Stem cells are defined as those cells that can perpetuate themselves through self renewal, involved in generation of mature cells through differentiation, play a role in organ homeostasis and are involved in tumourigenesis [18]. Cancer stem cell hypothesis states that only a small subset of rare tumour stem cells is capable of initiating and propagating tumour formation and a better characterization of these stem cells could lead to improvement of cancer therapies. According to the traditional model of carcinogenesis the cells ought to be more long lived and accumulate several mutations and genetic alterations to be able to convert to a cancer cell. The concept of contribution of stem cells in colorectal carcinoma widely accepted based on the fact that colon epithelium physiologically regenerates and is shed periodically over a short span of time [19]. This suggests the presence of stem cells which are long lived cells that accumulate cancer inducing mutations.
Similar to normal stem cells, cancer stem cells also show different stages of maturity and hierarchial structure of cells. More importantly cancer stem cells are heterogenous. Cancer stem cells have been identified in haemotological malignacies and even in solid tumours which includes colon cancer, ovarian cancer, lung cancer, liver cancer, pancreatic cancer, breast cancer, melanoma, etc [18].
Efforts are required to detect whether cancer stem cells are present in all cancers and involved in tumourigenesis [17]. If the disease is due to cancer stem cells, the present day treatment which targets all dividing cells may be useless as cancer stem cells are quiescent which makes full recovery of the patient at the time of treatment only to relapse a few years later when cancer stem cells are reactivated. This means we are not getting into the root of the problem [20]. Identification of cancer stem cells with specific markers helps to design effective anticancer drugs [17]. Since colorectal carcinoma is a common disease in western population not many studies have been carried out in Indian population. In view of the rising trend of the incidence of colorectal carcinoma in the Indian population this study was taken up to investigate the expression of new emerging stem cell marker CD66c in colorectal carcinoma of Indian origin.
CEA is a cell surface glycoprotein and is glycosylated with molecular weight 180,000. The genes for CEA family are clustered on long arm of chromosome 19. CEA gene family is included in immunoglobulin gene super family. CD66c belongs to CEA family [21] and was first described in 1965, as colon tumour specific antigen [22]. CD66c mediates invitro homotypic and heterotypic adhesion function [21]. This intercellular adhesion is a calcium dependent mechanism [23]. CD66c is involved in cellular aggregation [24]. CD66c is tethered to cytoplasmic membrane via phosphotidyl inositol anchor [25]. Very few studies have been done related to CD66c and it is an emerging biomarker which requires more attention as cancer stem cell marker.
In previous studies, the intensity of CD66c expression ranged from low to bright, CD66c with bright expression fully corresponded with CD133 positive cells. CD66c showed higher positivity in cases of hepatic metastasis. siRNA mediated silencing of CD66c inhibited proliferation, colony formation with enhancement of apoptosis and necrosis of colorectal carcinoma cells. It is also an independent prognostic factor in resectable colon samples. It is an important therapeutic target for monoclonal antibody and small interfering RNA based approaches in pancreatic malignancy [13]. It is upregulated in gastric tumours as well as in colon cancers [12]. It is also found in breast, lung tumours, normal spleen and granulocytes [23]. CD66c mRNA is expressed more in both gastric and colon cancer when compared to normal mucosa. CD66c is also elevated in most of the lung diseases and is considered as major component of diseased lung cells and play a role in cancer metastasis [26].
Our study showed that CD66c was expressed more in colon carcinoma when compared to rectal carcinoma and was statistically significant. CD66c showed differential expression with membrane positivity in normal colorectal mucosa and cytoplasmic positivity in colorectal carcinoma cells. The study by Gemia M et al., showed that CD66c expression was significantly higher in colorectal cancer specimens compared with that of adjacent normal tissue. The expression also showed a gradient increase from normal tissue to adenoma and from adenoma to cancerous tissue [13]. Similarly in the present study, the intensity of CD66c marker expression showed a gradient increase from normal to adenoma to carcinoma. In mucin secreting moderately differentiated adenocarcinoma, the mucin secretions took up the stain where as the tumour cells were negative for CD66c marker expression by immunohistochemistry.
Conclusion
CD66c can be specifically used for colon carcinoma and may be a novel marker for colon carcinoma stem cell isolation. The quantification of CD66c can be further verified by flow cytometry and RT-PCR. Further studies can be carried out using CD66c alone or in combination with other marker to develop cancer stem cell directed therapy.
[1]. Dong Y, Yu J, Ng SS, Micro RNA dysregulation as a prognostic biomarker in colorectal cancerCancer Manag Res 2014 6:405-22. [Google Scholar]
[2]. Zhou F, Mu YD, Liang J, Liu ZX, Chen HS, Zhang JF, Expression and prognostic value of tumour stem cell markers ALDH1 and CD133 in colorectal carcinomaOncol Lett 2014 7(2):507-12. [Google Scholar]
[3]. Nautiyal J, Kanwar SS, Yu Y, Majumdar AP, Combination of dasatinib and curcumin eliminates chemo-resistant colon cancer cellsJ Mol Signal 2011 6:7 [Google Scholar]
[4]. Maruthur NM, Bolen S, Gudzune K, Brancati FL, Clark JM, Body Mass Index and Colon Cancer Screening: A Systematic Review and Meta-AnalysisCancer Epidemiol Biomarkers Prev 2012 21(5):737-46. [Google Scholar]
[5]. Thenappan A, Li Y, Shetty K, Johnson L, Reddy EP, Mishra L, New Therapeutics Targeting Colon Cancer Stem CellsCurr Colorectal Cancer Rep 2009 5(4):209 [Google Scholar]
[6]. Oliver JA, Ortiz R, Melguizo C, Alvarez PJ, Gómez-Millán J, Prados J, Prognostic impact of MGMT promoter methylation and MGMT and CD133 expression in colorectal adenocarcinomaBMC cancer 2014 14:511 [Google Scholar]
[7]. Navarro-Alvarez N, Kondo E, Kawamoto H, Hassan W, Yuasa T, Kubota Y, Isolation and Propagation of a Human CD133-Negative Colon Tumour Derived Cell Line with Tumourigenic and Angiogenic PropertiesCell Transplant 2010 19(6):865-77. [Google Scholar]
[8]. Hibi K, Sakata M, Kitamura YH, Sakuraba K, Shirahata A, Goto T, Diabetes Promotes DMH-Induced Colorectal Cancer by Increasing the Activity of Glycolytic Enzymes in RatsAnticancer Res 2009 29(6):2235-37. [Google Scholar]
[9]. Rey T, Morrison SJ, Clarke MF, Weissman IL, Stem cells, cancer and cancer stem cellsNature 2001 414:105-11. [Google Scholar]
[10]. Tirinato L, Liberale C, Di Franco S, Candeloro P, Benfante A, La Rocca R, Lipid Droplets: A New Player in Colorectal Cancer Stem Cells Unveiled by Spectroscopic ImagingStem Cells 2015 33(1):35-44. [Google Scholar]
[11]. Thompson J, Seitz M, Chastre E, Ditter M, Aldrian C, Gespach C, Down-regulation of carcinoembryonic antigen family member 2 expression is an early event in colorectal tumourigenesisCancer Res 1997 57(9):1776-84. [Google Scholar]
[12]. Kinugasa T, Kuroki M, Takeo H, Matsuo Y, Ohshima K, Yamashita Y, Expression of four CEA family antigens (CEA, NCA, BGP AND CGM2) in normal and cancerous gastric epithelial cells: up-regulation of BGP and CGM2 in carcinomasInt J Cancer 1998 76(1):148-53. [Google Scholar]
[13]. Gemei M, Mirabelli P, Di Noto R, Corbo C, Iaccarino A, Zamboli A, CD66c is a novel marker for colorectal cancer stem cell isolation, and its silencing halts tumour growth in vivoCancer 2013 119(4):729-38. [Google Scholar]
[14]. Takahashi H, Okai Y, Paxton RJ, Hefta LJ, Shively JE, Differential Regulation of Carcinoembryonic Antigen and Biliary Glycoprotein by gamma-InterferonCancer Res 1993 53(7):1612-19. [Google Scholar]
[15]. Schölzel S, Zimmermann W, Schwarzkopf G, Grunert F, Rogaczewski B, Thompson J, Carcinoembryonic antigen family members CEACAM6 and CEACAM7 are differentially expressed in normal tissues and oppositely deregulated in hyperplastic colorectal polyps and early adenomasAm J Pathol 2000 156:595-605. [Google Scholar]
[16]. World Health OrganizationInternational histological classifications of tumours. No 15Histological typing of intestinal tumours 1976 WHO, Geneva [Google Scholar]
[17]. Pantic I, Cancer stem cell hypotheses: Impact on modern molecular physiology and pharmacology researchJ Biosci 2011 36(5):957-61. [Google Scholar]
[18]. Zou J, Yu XF, Bao ZJ, Dong J, Proteome of human colon cancer stem cells: A comparative AnalysisWorld J Gastroenterol 2011 17(10):1276-85. [Google Scholar]
[19]. Todaro M, Francipane MG, Medea JP, Stassi G, Colon cancer stem cells: A promise of targeted therapyGastroenterology 2010 138:2151-62. [Google Scholar]
[20]. Regenbrecht CR, Lehrach H, Adjaye J, Stemming Cancer: Functional Genomics of Cancer Stem Cells in Solid TumoursStem Cell Rev 2008 4(4):319-28. [Google Scholar]
[21]. Nollau P, Scheller H, Kona-Horstmann M, Rohde S, Hagenmüller F, Wagener C, Expression of CD66a (Human C-CAM) and Other Members of the Carcinoembryonic Antigen Gene Family of Adhesion Molecules in Human Colorectal AdenomasCancer Research 1997 57(12):2354-57. [Google Scholar]
[22]. Hasegawa T, Isobe K, Tsuchiya Y, Oikawa S, Nakazato H, Nakashima I, Nonspecific cross reacting antigen (NCA) is a major member of the carcinoembryonic antigen (CEA)-related gene family expressed in lung cancerBr J Cancer 1993 67(1):58-65. [Google Scholar]
[23]. Hauck W, Stanners CP, Control of carcinoembryonic antigen gene family expression in a differentiating colon arcinoma cell line, Caco-2Cancer Res 199 51(13):3526-33. [Google Scholar]
[24]. Nollau P, Prall F, Helmchen U, Wagener C, Neumaier M, Dysregulation of Carcinoembryonic Antigen Group Members CGM2, CD66a (Biliary Glycoprotein), and Nonspecific Cross-Reacting Antigen in Colorectal CarcinomasAm Pathol 1997 151(2):521-30. [Google Scholar]
[25]. Chao C, Carmical JR, Ives KL, Wood TG, Aronson JF, Gomez GA, CD133+ colon cancer cells are more interactive with the tumour microenvironment than CD133- cellsLab Invest 2012 92(3):420-36. [Google Scholar]
[26]. Kodera Y, Isobe K, Yamauchi M, Satta T, Hasegawa T, Oikawa S, Expression of carcinoembryonic antigen (CEA) and nonspecific crossreacting antigen (NCA) in gastrointestinal cancer; the correlation with degree of differentiationBr J Cancer 1993 68(1):130-36. [Google Scholar]