Uric acid (UA) and bilirubin are the final catabolic products of purine and heme metabolism respectively. It is hypothesized that uric acid is evolutionary substitute for loss of ability to synthesize ascorbate in humans. Uric acid exists in blood plasma at maximum level of solubility. This is also true for bilirubin in status of hyperbilirubinaemia [1]. There are some evidences that oxidative stress may have a role in atherosclerosis and pathogenesis of coronary artery disease (CAD) [2]. Uric acid is the main quantitative determinant of total antioxidant capacity of plasma (TAOC), and hence expected to protect against progression of atherosclerosis [3,4]. In other hand, it is a component of the metabolic syndrome and associates to CAD positively [5,6].
Many epidemiologic studies over the past 50 years have confirmed an association of elevated serum UA level with the incidence of CAD, but the results have not been entirely consistent [6,7]. While some studies show an independent association [8–12], others suggest that the association is due to confounding by other risk factors related to the multiple metabolic syndrome including hypertension, insulin resistance, hyperlipidaemia, obesity and diuretic use [13,14]. Some studies have also shown the associations only among women but not in men [15] or only among alcohol abstainers [16]. This study was performed to investigate the association of UA with CAD and the role of TAOC and metabolic syndrome in patients who underwent coronary angiography.
Materials and Methods
Experimental design, subjects and angiographic assess-ment: The experimental design, angiographic assessment and anthropometrics measurements were as described previously [17]. In brief, the study population consisted of 148 men and 152 women aged 35-76 years who were suspicious in CAD and consecutively referred and underwent their first coronary angiography at Zahra hospital of university of Mazandaran. The subjects were excluded from the study that had a recent history of acute myocardial infarction, precutaneous transluminal coronary angioplasty, infectious or inflammatory disease, severe liver or renal disease, neoplasm and haematologic disorders. Subjects with one or more lesions that narrowed the lumen of any coronary artery significantly (>70%) were considered to be CAD cases, whereas those without any narrowing (<10%) were taken as controls. The severity of coronary occlusion was scored on the basis of the number and the extent of lesions as: 1 (normal); 2 (mild); 3 (moderate); and 4 (severe) [18].
Biochemical and haematological measurements: Blood samples collection, plasma preparations and the measurements of lipids are described in reference 17. All measurements were done on fresh serum, plasma or whole blood. TAOC was assayed using the method of FRAP and UA by uricase method, Pars-Azmon (Tehran, Inc) [19]. All other biochemical and haematological parameters were measured by routine laboratory methods.
Statistical Analysis
The results are presented as the mean±SD and median (interquartile range) for normal and skewed distributed variables respectively. Serum UA was categorized into tertiles based on the cut-points of the entire distribution and the patients’ characteristics were calculated accordingly. Proportions and means (or median) were calculated for baseline risk factors. The significance of any differences in proportions or medians was tested with Kruskal-Wallis test, and in means using analysis of variance (ANOVA). All p-values are two-tailed and differences were considered significant if p-values were <0.05. A multivariate logistic regression analysis with conditional forward approach was carried out to find out the independency of the correlations (SPSS version 15). The prevalence of CAD was entered as dependent variable and the criteria for entrance and removal of the variables to regression equation were 0.05 and 0.1 respectively. The biochemical parameters were entered in the form of continuous variables and the odds ratios were presented as the standardized regression coefficients by the term of Exp (β), associated with 1 SD changes in the risk factor. The results of multivariate analysis were expressed as odds ratio with 95% confidence intervals. Bivariate and partial correlation analyses were used to assess the correlation between UA and other variables. In analysis of partial correlation the association adjusted for other variables.
Results
Demographic and clinical parameters of the subjects: The prevalence of cigarette smoking, diabetes mellitus and hypertension was more in CAD cases than control subjects [Table/Fig-1]. There were significant differences in consuming antilipidemics, nitrates, beta-blockers, calcium antagonists and aspirin between two groups. Patients with CAD compared with the controls had increased levels of serum glucose, triglycerides, creatinine, uric acid and TAOC and decreased levels of HDL cholesterol. Erythrocyte sedimentation rate (ESR) and platelets counts were also different between two groups significantly. There were no any significant differences in the levels of bilirubin and albumin between two groups.
Demographic and clinical characteristics in CAD controls and patients.
| Without CAD (n=64) | With CAD (n=174) | p |
|---|
| Clinical characteristics |
| Age, year | 52.6 ± 10.5 | 58.9 ± 9.5 | 0.001 |
| Gender, male%(n) | 35.9 (23) | 60.3 (105) | 0.001 |
| BMI, kg/m2 | 27.3 ± 4.2 | 26.9 ± 4.2 | 0.537 |
| Physical inactivity, %(n) | 56.3 (36) | 52.3 (91) | 0.363 |
| Smoking, %(n) | 7.8 (5) | 20.7 (36) | 0.030 |
| Diabetes mellitus, %(n) | 15.6 (10) | 33.9 (59) | 0.009 |
| Systolic pressure | 111.8 ± 13.8 | 118.0 ± 19.0 | 0.011 |
| Diastolic pressure | 68.9 ± 10.3 | 72.4 ± 11.1 | 0.034 |
| Hypertension, %(n) | 43.8 (28) | 69.0 (120) | 0.001 |
| Drugs |
| Hypoglycemic, %(n) | 14.1 (9) | 17.2 (30) | 0.839 |
| Antilipidemic, % (n) | 34.4 (22) | 50.0 (87) | 0.033 |
| Diuretics, %(n) | 12.5 (8) | 11.5 (20) | 0.645 |
| Nitrates, %(n) | 23.4 (15) | 52.9 (92) | 0.001 |
| Beta-blockers, %(n) | 40.6 (26) | 58.1 (101) | 0.046 |
| Calcium antagonists, %(n) | 1.6 (1) | 14.4 (25) | 0.006 |
| ACE-inhibitors, %(n) | 11.8 (6) | 16.1 (28) | 0.289 |
| Aspirin, % (n) | 46.9 (30) | 70.1 (122) | 0.003 |
| Biochemicals |
| Glucose, mg/dL | 104.5 ± 28.5 | 123.1 ± 56.6 | 0.001 |
| Triglycerides, mg/dL | 141.7 (93.0–1949) | 157.3 (116.8–2315) | 0.051* |
| Total cholesterol, mg/dL | 190.7 ± 47.1 | 185.8 ± 49.2 | 0.402 |
| HDL-C, mg/dL | 44.9 ± 11.8 | 39.5 ± 10.5 | 0.002 |
| LDL-C, mg/dL | 113.4 ± 38.7 | 110.1 ± 43.8 | 0.584 |
| BUN, mg/dL | 17.1 ± 5.5 | 18.3 ± 8.7 | 0.225 |
| Creatinine, mg/dL | 0.9 ± 0.2 | 1.1 ± 0.8 | 0.003 |
| Bilirubin, mg/dL | 0.04 ± 0.02 | 0.04 ± 0.02 | 0.741 |
| Uric acid, mg/dL | 4.3 ± 0.9 | 4.9 ± 1.1 | 0.001 |
| Females | 4.1 ± 0.8 | 4.5 ± 1.1 | 0.024 |
| Males | 4.7 ± 0.9 | 5.2 ± 1.1 | 0.023 |
| TAOC, g/L | 605.0 ± 89.6 | 644.6 ± 128.2 | 0.009 |
| Albumin, g/dL | 4.6 ± 0.3 | 4.5 ± 0.3 | 0.742 |
| Leukocyte counts (cells/nL) | 8.2 ± 1.9 | 8.8 ± 2.2 | 0.089 |
| Erythrocytes counts (cells/nL) | 4.6 ± 0.5 | 4.6 ± 0.7 | 0.775 |
| Platelets counts ×109/L | 264.1 ± 70.1 | 255.6 ± 74.2 | 0.032 |
| ESR (mm/h) | 12 (1–61) | 14 (1–90) | 0.059* |
The continuous and categorical variables were compared by t- and χ2-tests, respectively. The 48 subjects with mild CAD were not included in the analysis. The number in each group has shown in parentheses. The results are presented as the means ± SD and median (interquartile range). Mann-Whitney test (*). ACE: angiotensin-converting enzyme, BMI; body mass index, BUN; blood urea nitrogen, CAD; coronary artery disease, ESR; erythrocyte sedimentation rate, TAOC; total antioxidant capacity.
Characteristics of the study participants according to UA tertiles: The prevalence and severity of CAD and odds ratios for CAD were associated with the tertiles of UA significantly [Table/Fig-2]. Cigarettes’ smoking, male sex and hypertension were more, whereas diabetes mellitus was less prevalent in the top relative to bottom tertile of UA. Subjects with UA levels in the upper tertile had significant higher levels of serum triglycerides, BUN, creatinine and TAOC and lower levels of glucose and HDL-C.
Anthropometrics and biochemical characteristics of the study participants according to the tertiles of UA.
| Variables | Uric acid tertiles (mg/dL) | p |
|---|
| < 4.12 | 4.12 – 5.04 | > 5.04 |
|---|
| Anthropometrics: |
| Frequency of CAD, %(n) | 48.0 (47) | 51.0 (49) | 77.2 (78) | 0.001 |
| CAD severity | 1.6 ± 1.2 | 1.6 ± 1.3 | 2.3 ± 1.0 | 0.002 |
| Relative Odds | 1.0 | 0.8 | 3.2 | 0.007 |
| Age (yr) | 57.1 ± 8.3 | 57.0 ± 10.9 | 58.1 ± 10.8 | 0.358 |
| Sex (male) %(n) | 24.5 (24) | 47.9 (46) | 74.3 (75) | 0.001 |
| Physical inactivity, %(n) | 52 (51) | 55.2 (53) | 51.7 (52) | 0.652 |
| Smoking, %(n) | 11.5 (11) | 12.8 (12) | 25.7 (26) | 0.007 |
| Diabetes mellitus, %(n) | 41.7 (40) | 27.6 (27) | 19.8 (20) | 0.002 |
| Hypertension, %(n) | 58.3 (56) | 55.1 (54) | 68.3 (69) | 0.038 |
| Drugs: | | | | |
| Diuretics, %(n) | 5.1 (5) | 7.3 (7) | 17.8 (18) | 0.006 |
| Hypoglycemic, %(n) | 25.5 (25) | 15.6 (15) | 8.9 (9) | 0.015 |
| Biochemicals: | | | | |
| Glucose, mg/dL | 129.1 ± 60.2 | 117.1 ± 50.5 | 108.7 ± 34.6 | 0.024 |
| Triglycerides, mg/dL | 136.3 (102.0–1907) | 150.4 (98.9–2267) | 168.8 (116.2–2343) | 0.038 |
| Total cholesterol, mg/dL | 183.4 ± 46.1 | 190.3 ± 43.3 | 188.3 ± 51.5 | 0.661 |
| HDL-C, mg/dL | 42.2 ± 10.7 | 42.7 ± 10.9 | 39.5 ± 10.6 | 0.043 |
| LDL-C, mg/dL | 109.7 ± 37.9 | 111.3 ± 39.4 | 110.8 ± 44.2 | 0.841 |
| BUN, mg/dL | 15.6 ± 4.9 | 17.5 ± 7.3 | 20.0 ± 9.4 | 0.001 |
| Creatinine, mg/dL | 0.9 ± 0.2 | 1.1 ± 0.8 | 1.2 ± 0.8 | 0.003 |
| Bilirubin, mg/dL | 0.03 ± 0.02 | 0.04 ± 0.02 | 0.04 ± 0.02 | 0.063 |
| TAOC, g/L | 523.0 ± 85.8 | 626.4 ± 68.9 | 729.7 ± 99.4 | 0.001 |
| Albumin, g/L | 4.5 ± 0.3 | 4.6 ± 0.3 | 4.6 ± 0.3 | 0.222 |
| Leukocyte counts (cells/nL) | 8.5 ± 1.9 | 8.4 ± 2.0 | 8.9 ± 2.2 | 0.132 |
| Erythrocytes counts(cells/nL) | 4.5 ± 0.6 | 4.6 ± 0.6 | 4.7 ± 0.7 | 0.215 |
| ESR (mm/h) | 15 (10–253) | 12 (6–22) | 14 (9–243) | 0.132 |
The total 300 subjects were divided into tertiles according to UA distribution and the significance of any differences in means or proportions were tested with analysis of variance (ANOVA) and Kruskal-Wallis tests respectively. The results are presented as the means ± SD and median (interquartile range). BUN; blood urea nitrogen, CAD; coronary artery disease, ESR; erythrocyte sedimentation rate, TAOC; total antioxidant capacity.
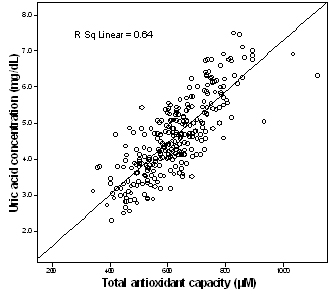
Correlation of UA with other risk factors: Different analyses were performed to address the correlation of UA with other risk factors [Table/Fig-3]. In bi-variate correlation analysis, UA correlated with the prevalence of male sex, cigarette smoking positively and diabetes mellitus negatively and significantly. Serum UA levels were also high positive correlate of serum total and LDL-cholesterol, triglyceride, creatinine, BUN, bilirubin, TAOC and were negative correlate of glucose and HDL-C. [Table/Fig-4] shows that UA has a strong association with TAOC (r =0.799, p=0.001).
The correlation coefficients of uric acid relative to other risk factors. Bivariate correlation analysis was performed using SPSS software. BUN; blood urea nitrogen, CAD; coronary artery disease, TAOC; total antioxidant capacity.
| Variables | Correlation coefficients (r) | p |
|---|
| Incidence of CAD | 0.243 | 0.001 |
| Severity of CAD | 0.278 | 0.001 |
| Sex | 0.396 | 0.001 |
| Smoking | 0.148 | 0.023 |
| Diuretics | 0.168 | 0.008 |
| Hypertension | 0.090 | 0.127 |
| Diabetes Mellitus | -0.177 | 0.007 |
| Glucose | -0.161 | 0.007 |
| Triglyceride | 0.143 | 0.008 |
| Total cholesterol | 0.206 | 0.001 |
| LDL-C | 0.256 | 0.001 |
| HDL-C | -0.148 | 0.001 |
| BUN | 0.296 | 0.001 |
| Creatinine | 0.225 | 0.001 |
| Bilirubin | 0.120 | 0.041 |
| TAOC | 0.799 | 0.001 |
| Leukocyte counts | 0.124 | 0.035 |
| Erythrocytes counts | 0.129 | 0.028 |
Scatter plot for the association of TAOC with UA. There was one outlier value in TAOC data that was excluded from the study. P < 0.001.
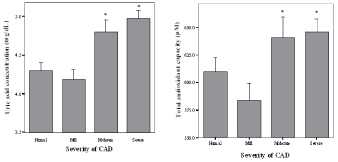
Association of plasma analytes with the severity of CAD: Plasma TAOC {F(3,274)= 4.1, p=0.007} and its major determinant uric acid {F(3,279)= 9.8, p<0.001} exhibited significant association with the severity of CAD [Table/Fig-5]. Serum glucose {F(3,271)= 3.2, p=0.02}, creatinine {F(3,278)= 3.0, p=0.03}, potassium {F(3,276)= 3.7, p=0.01} and HDL-C {F(3,276)= 5.6, p=0.01} also showed significant association with the severity of CAD (results not shown). No any other biochemical parameters had significant association with the severity of CAD.
Association of uric acid and TAOC with the severity of CAD.
The severity of CAD was scored on the bases of the number and the extent of lesions in coronary arteries as described in methods section. The value of each variable in any group were calculated and presented as the mean + SE. * indicates p < 0.01.
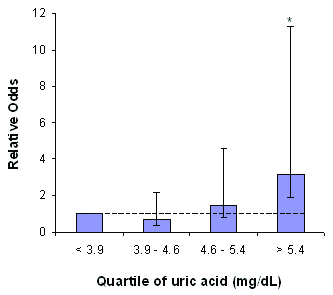
Association of variables with the incidence of CAD: Both uni- and multi-variate logistic regression analyses with conditional approach were performed to test the independency of the correlations between risk factors and CAD. The criteria for entrance and removal of the variables into regression equation were 0.05 and 0.1 respectively. In univariate analysis, UA correlated with CAD by the odds ratio (OR) of 1.77 (1.31-2.39), p<0.001, TAOC by OR of 1.003 (1.000-1.005), p=0.03 and glucose by OR of 1.011 (1.002-1.020), p=0.02. Although creatinine showed significant association with the severity of CAD, it did not remain in regression equation even as a single variable. The relative odds of UA in the top relative to the bottom quartile was also 3.14 (1.22-8.12), p=0.01 in univariate analysis [Table/Fig-6].
Relative odds for CAD associated with quartiles of uric acid.
There are 76 patients in each group. Error bars show 95% confidence intervals for risk estimates. * indicates p < 0.01.
Major classical risk factors as well as UA, TAOC, glucose, BUN and creatinine were included in the multivariate conditional forward analysis. If hypertension is not included in analysis UA but not TAOC would remain with the OR of 1.57 (1.07-2.29), p=0.02. Glucose and UA were excluded from the regression equation after adjustment for diabetes and hypertension respectively. Finally, male sex, age, diabetes, hypertension, total- and HDL- cholesterol were kept in the model significantly [Table/Fig-7].
Multivariate conditional forward logistic regression analysis. In each model a new variable was added to the previous variables and the data of the last model with six parameters and one constant has been presented.
| Model | Included variables | -2LL | Cox-Snell R- square | OR Exp (β) | 95% CI | Predictive value | p |
|---|
| 1 | Age | 227.8 | 0.088 | 1.08 | 1.04 – 1.13 | 76.0 | 0.001 |
| 2 | + HDL-C | 212.4 | 0.149 | 0.92 | 0.88 – 0.96 | 78.3 | 0.001 |
| 3 | + Male sex | 203.6 | 0.182 | 5.16 | 2.25 – 11.79 | 80.1 | 0.001 |
| 4 | + Hypertension | 191.0 | 0.227 | 4.74 | 2.07 – 10.85 | 81.0 | 0.001 |
| 5 | + Cholesterol | 185.3 | 0.247 | 1.01 | 1.002 – 1.021 | 81.9 | 0.034 |
| 6 | + Diabetes mellitus | 181.2 | 0.261 | 2.50 | 1.00 – 6.29 | 82.4 | 0.051 |
R: multiple correlation coefficient of each model, OR: odds ratio and CI: confidence interval, LL: Log of likelihood
Discussion
The findings of the current study indicate that the plasma TAOC and its major determinants UA but not bilirubin and albumin are significantly associated with the prevalence and severity of CAD. But the correlation was not independent, so that it will weaken if the results were adjusted for the classical risk factors especially hypertension.
Serum Uric Acid and Cad
Some studies have found that higher concentrations of UA is an independent risk factor for CAD [8–12], whereas others have concluded that the association was confounded by the relationship of UA with established risk factors [13,14]. They have postulated that elevated serum UA is a physiological marker of hypertension, insulin resistance, obesity and hyperlipidaemia rather than a direct cause of atherosclerotic disease. Uric acid level also tended to be higher among those who were current smokers [14]. In the current study, UA showed significant and independent correlations with male sex, diabetes mellitus, hypertension, triglyceride, TAOC and using of diuretics [Table/Fig-3]. It has demonstrated a direct correlation between hypertension and UA, as the hypertension is more severe; hyperuricaemia will be present more likely [1,20,21]. It is recognized for more than three decades that diuretics increases the incidence of gouty attacks [1]. In our study, the correlation of UA with serum BUN and creatinine reveals the involvement of the kidney [21,22].
Kim et al., determined the mean risk of CAD associated with hyperuricaemia in a meta-analysis of 26 cohort studies of about 400,000 adults [6]. They reported that UA was associated with CAD by the relative risk of 1.46 (1.20-1.73), but after adjustment for confounders the association was lessened to 1.09 (1.03-1.16). Whealer et al., in a more recent meta-analysis using the data of 16 prospective studies have found the odds ratio of 1.13 (1.07-1.20) but it weakened to 1.02 (0.91-1.14) when the results were adjusted for confounding factors [7].
Blood antioxidant enzymes, MDA, total bilirubin and CAD
We also measured malondialdehyde (MDA) and antioxidant enzymes glutathione peroxidase, catalase and superoxide desmutase (results not shown). However no significant differences have seen between two groups. Flores-Mateo et al., in a meta-analysis of 11 case-control and prospective studies has shown the inverse relationship between the activity of antioxidant enzymes and incidence of CAD [22,23]. Bilirubin at a high concentration protects against CAD in Gilbert syndrome [24], but it does not have any association with CAD at normal level [25] as seen in the current study. The findings are also inconsistent regarding to the association of MDA with CAD [26,27].
Plasma Total antioxidant capacity (TAOC) and CAD
There are conflicting results about the association of TAOC and incidence of CAD [26–32]. In a cross-sectional study of 968 adults, there were not any significant differences in TAOC and the activity of anti-oxidant enzymes but UA and MDA were increased in CAD group [28]. TAOC did not change significantly between control and CAD groups in a small sample study in Istanbul [26]. In three separate studies, the lipid peroxides had increased significantly but TAOC decreased in CAD patients group [27–30]. Nieto et al., in a case-control prospective study of 150 patients found that only TAOC but not anti-oxidant vitamins were increased between two groups [31]. The plasma of NIDDM patients with CAD had also significant higher values of TAOC relative to patients without CAD [32]. The results of the present study showed that TAOC was higher in CAD group and the changes occurred totally in UA. TAOC and UA also showed significant correlation not only with the occurrence but also with the severity of CAD. This finding is in accord with the results of Nieto et al., [31]. We measured TAOC as ferric reducing ability of plasma (FRAP), but others used Randox method as total radical trapping potential (TRAP) [26–32]. It is recommended to measure TAOC instead of individual antioxidants, because it covers total antioxidant potential of plasma. More than 60% of TAOC is attributed to UA in the method of FRAP [33]. In general, the results are not matched for different methods to measure plasma TAOC [33]. The new method of potentiometery is preferred to the procedures of TRAP and FRAP [34].
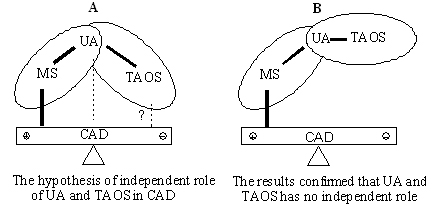
Uric acid as two edged blade: determinant of antioxidant or metabolic syndrome [Table/Fig-8].
Dual probable functions of uric acid in CAD.
Uric acid (UA) participates both in metabolic syndrome (MS) and in total antioxidant system (TAOS). The seesaw diagram shows the opposite roles of MS and TAOS in atherosclerosis. Solid lines indicate independent correlation between two parameters. (A) As the initial hypothesis, antioxidant system may have a direct independent role in CAD. (B) The present results indicate that the correlation of UA and TAOC with CAD is dependent via metabolic syndrome.
UA is the main quantitative determinant of plasma TAOC [3,4]. If UA played a role as an antioxidant in CAD, it would be expected to decrease in CAD patients. Inversely, both UA and TAOC were significantly increased in patients with CAD [Table/Fig-1]. In the multivariate analysis of our results in the absence of hypertension, UA was associated with the occurrence of CAD by the odds ratio of 1.57 (1.07-2.29). The association was weakened and UA was excluded from the regression equation after adjustment for hypertension [Table/Fig-7]. The correlation of TAOC with CAD was yet weaker than UA. The strong correlation of UA with plasma BUN and creatinine implies the involvement of the kidney [Table/Fig-3]. It has been proposed that UA have a casual role in hypertension [1]. The mechanisms whereby UA causes hypertension are oxidative stress, endothelial dysfunction, activation rennin angiotensin system and decrease in renal blood flow [20,21]. Onat et al., in a cohort study showed that hyperuricaemia correlates with pro-inflammatory state and HDL dysfunction in nondiabetic people [35]. Nevertheless, the hypothesis of uric acid-hypertension have challenged by some evidence [36].
Limitation
The limitation of the current study is attributed to its cross-sectional nature, so that a causal relation cannot be established. In addition, we measured TAOC by the method of FRAP, in which UA contributes more quantitatively. TAOC can be assayed by the new method of potentiometery that remains to be studied.
Conclusion
It could be concluded that, the relation of UA with CAD is attributed to the components of metabolic syndrome especially hypertension. The measurement of UA and TAOC will not improve the prognostic power beyond the classical risk factors. On the other hand, the increase in UA and TAOC may have a defense and protective mechanism against the progression of atherosclerosis in CAD patients.
The continuous and categorical variables were compared by t- and χ2-tests, respectively. The 48 subjects with mild CAD were not included in the analysis. The number in each group has shown in parentheses. The results are presented as the means ± SD and median (interquartile range). Mann-Whitney test (*). ACE: angiotensin-converting enzyme, BMI; body mass index, BUN; blood urea nitrogen, CAD; coronary artery disease, ESR; erythrocyte sedimentation rate, TAOC; total antioxidant capacity.
The total 300 subjects were divided into tertiles according to UA distribution and the significance of any differences in means or proportions were tested with analysis of variance (ANOVA) and Kruskal-Wallis tests respectively. The results are presented as the means ± SD and median (interquartile range). BUN; blood urea nitrogen, CAD; coronary artery disease, ESR; erythrocyte sedimentation rate, TAOC; total antioxidant capacity.
R: multiple correlation coefficient of each model, OR: odds ratio and CI: confidence interval, LL: Log of likelihood