Accuracy of Needle Placement into the Intra-Articular Space of the Knee in Osteoarthritis Patients for Viscosupplementation
Manaswini Telikicherla1, Surendra Umesh Kamath2
1 Student, Kasturba Medical College Hospital, Attavar, Mangalore, Manipal University, Manipal, Karnataka, India.
2 Professor and Head, Department of Orthopaedics, Kasturba Medical College Hospital, Attavar, Mangalore, Manipal University, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Surendra Umesh Kamath, Krithika, 5-7-710/2, Near Sathyasai Nursing Home, Dongerkery, Mangalore-575003, Karnataka, India.
E-mail: skamath3@hotmail.com
Introduction
Knee osteoarthritis is characterized by inflammation in the intra-articular space or synovial membrane, breakdown of articular cartilage, and sclerosis of the subchondral bone. Intra-articular injections of Sodium hyaluronate which have viscoelastic and protective effect on articular cartilage and restores normal articular homeostasis. The efficacy of these injections is diminished when they are placed inadvertently outside the joint. For the maximum benefit, injection of hyaluronic acid derivatives needs to be placed accurately into the knee joint.
Aim
The study was performed to know the correct placement of needle inside the knee joint prior to Viscosupplementation by fluoroscopy using a contrast material.
Materials and Methods
The accurate placement of needle was evaluated in a prospective series of 94 consecutive injections in patients without clinical knee effusion. All the injections were performed by single orthopaedic surgeon using a 5 cm 21-gauge needle through anterolateral, and lateral midpatellar portals. The needle placement in the knee joint was confirmed with fluoroscopy using the contrast material.
Results
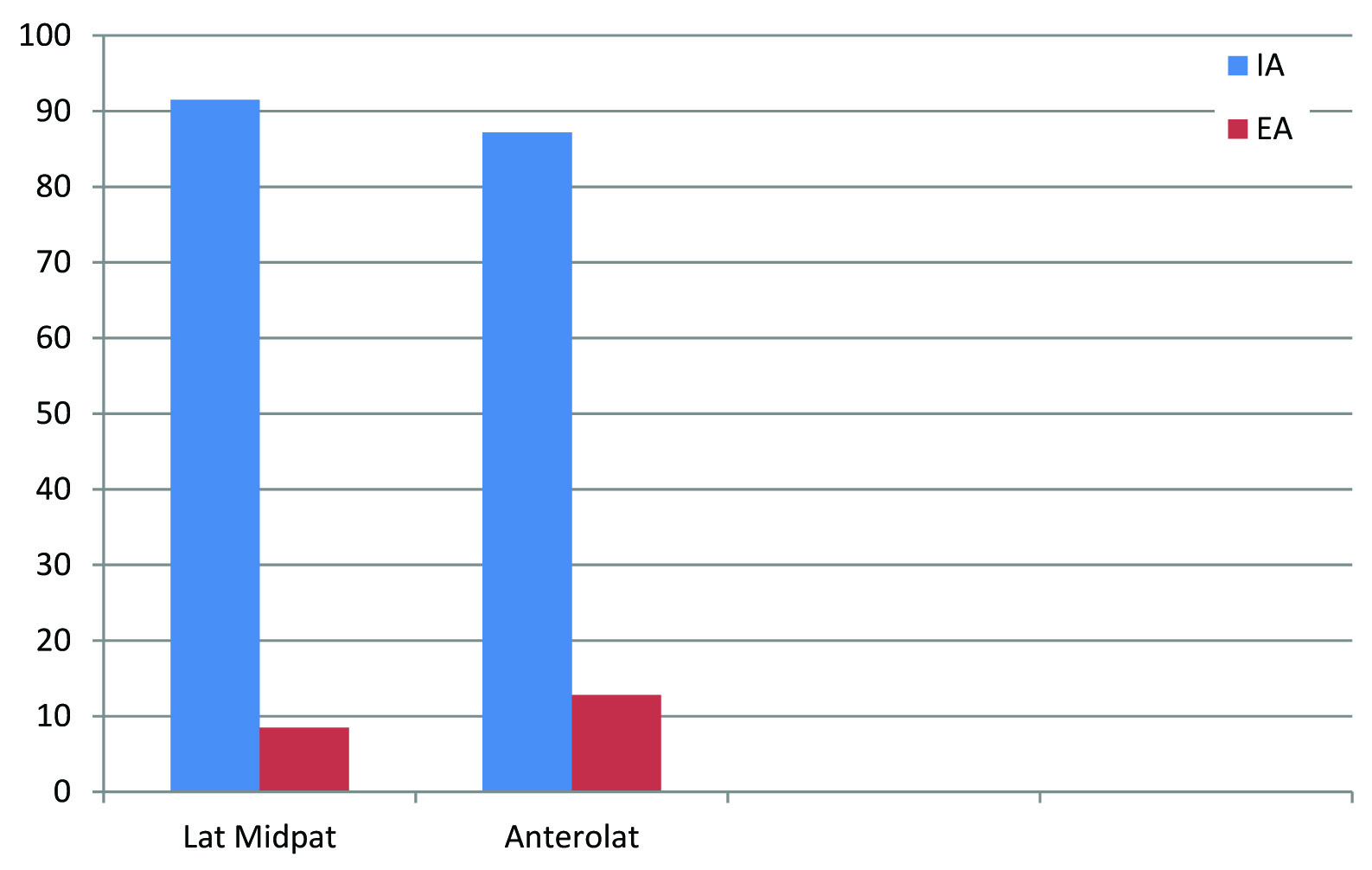
The accuracy rates through Lateral midpatellar and Anterolateral portals were lower than expected rate (100%). A total of 43 out of 47 injections were intra-articular, indicating accuracy of 91.5% through lateral midpatellar portal, 41 out of 47 injections were intra-articular through anterolateral portal with accuracy of 87.4%.
Conclusion
Study showed that the accuracy of needle placement was higher through Lateral midpatellar than the Anterolateral portal.
Anterolateral portal, Corticosteroid, Inflammation, Lateral midpatellar
Introduction
Knee osteoarthritis is characterized by inflammation in the intra-articular space or synovial membrane, breakdown of articular cartilage, and sclerosis of the subchondral bone [1]. The patients may have more severe joint symptoms, such as pain, swelling, stiffness, and limitations in their activities of daily living, if this condition leads to increasingly degenerative changes to the articular cartilage. Osteoarthritis of the knee joint with symptoms is a common presentation in primary care and can be a difficult problem for treating physicians and patients. Based on radiographic features, the Kellgren- Lawrence system classifies the severity of knee Osteoarthritis into 5 grades.
Treatment modalities for osteoarthritis and their benefits are often limited. An intra-articular injection of corticosteroid is commonly used for the treatment of osteoarthritis with inflammation or swelling. If the injected corticosteroid extravasates into the soft tissues, it might be associated with complications such as fat tissue atrophy and changes in skin colour [2,3]. Therefore, it is very essential to inject it into the intra-articular space accurately. Accuracy of needle placement may vary with age, gender and severity of osteoarthritis of knee [4].
In osteoarthritis, the viscosity of the synovial fluid reduces secondary to a decrease in the molecular weight and concentration of hyaluronic acid. An intra-articular injection of Sodium hyaluronate, known as Viscosupplementation, is a recently available option. Viscosupplements have been approved for osteoarthritic joints [1–3]. Intra-articular injections of sodium hyaluronate which have viscoelastic and protective effect on articular cartilage and restores normal articular homeostasis [4]. The efficacy of these injections is diminished when they are placed inadvertently outside the joint [5]. To achieve their maximum benefit, hyaluronic acid derivatives should be injected directly into the knee joint space. In the absence of a knee effusion, needle placement into the intra-articular space is a challenge [4].
Incorrect placement of injections outside the joint can cause a reduced effect [4–6]. Hyaluronic acid will not to have any beneficial effect when applied to the tissue surrounding the joint [7]. As these injections are expensive it is very essential that the injection has to be given accurately inside the joint for a maximum benefit. Injection into a soft tissue injection can cause more discomfort to the patient [8]. Accuracy of needle placement inside the joint can be a challenge in dry knees.
Aim
The study was performed to know the correct placement of needle inside the knee joint prior to Viscosupplementation by fluoroscopy using a contrast material.
Materials and Methods
The study was conducted in a teaching hospital after getting a clearance from institutional ethics committee. All those patients requiring intraarticular injection for therapeutic reasons between August 2014 and October 2014 were included in the study. Those patients who were not willing to sign the informed consent, who had evidence of local infection, who were allergic to contrast dye and elevated creatinine were excluded from the study.
Correct placement of needle was evaluated in a prospective series of 94 consecutive injections in patients without clinical knee effusion. The injections were performed by single orthopaedic surgeon using a 5 cm 21-gauge needle through anterolateral, and lateral midpatellar portals. The needle placement was confirmed with fluoroscopy using contrast material.
Injection through the anterolateral portal was performed with the patient in sitting position with the affected knee flexed to about 90°. After palpating the landmarks, the injection was given inferior to the patella, through the joint line either medial or lateral to the ligamentum patella directing the needle obliquely toward the intercondylar notch [Table/Fig-1].

The lateral midpatellar injections were carried out with the lower limb. The patella was everted and moved laterally, the needle was advanced transversely between the articular surfaces of the patellofemoral joint at the level of midpoint of the patella [Table/Fig-2].
Lateral Midpatellar Portal.

Prior to needle placement, the c-arm of the Fluoroscopy unit was positioned to obtain an initial lateral image to center the knee on the screen. Under aseptic precaution after skin preparation the area was anesthetized by injecting 2% lignocaine onto the skin. The needle was positioned the desired location, and 0.5 mL of contrast material was injected into the knee. A second lateral image was taken to look for the dye dispersion. With correct placement of needle, the dye will get dispersed freely in the joint and will be seen as “coating” the articular surface. With incorrect placement of needle the dye will pool in the fat pad or subsynovial tissues. Dye dispersion was reconfirmed with a repeat Fluoroscopy after the knee was cycled five times through a range of movements.
Statistical Analysis
The collected data was analysed using Statistical Package for Social Sciences(SPSS) version 11.5, for comparison across the groups chi-square test was used where p<0.05 was considered statistically significant.
Results
The anterolateral portal included 47 knees of which there were 31(65.9%) women and 16 (34.1%) men in the age group of 33-82 years. Of these 36 (76.5%) and 11(23.4%) were of Kellegren-Lawrence grade 2 and 3 knees, respectively. The lateral midpatellar portal included 47 knees of which there were 29 (61.7%) women and 18 (38.2%) men in the age group of 33-85 years. Of these, 39 (82.9%) and 8 (17.1%) were of Kellegren-Lawrence grade 2 and 3 knees, respectively. There were no significant differences in demographic data between the groups.
Through lateral midpatellar portal, the accuracy of intra-articular placement for females was 89.7% and males were 94.4% when compared to anterolateral where it was 83.9% and 93.8% for females and males respectively. The accuracy of intra-articular placement for both the portals was compared in terms of K-L grading, which was 86.1% and 90.9% for anterolateral while it was 92.3% and 87.5% for lateral midpatellar portal in K-L grade 2 and 3 respectively. Patients aged <40 and >60 years had an accuracy of 100% and 90% respectively through both the portals while patients in the age group of 41-59 had an accuracy of 84.6% and 91.3% through anterolateral and lateral midpatellar respectively.
The accuracy rates through Lateral midpatellar and Anterolateral portals were lower than expected rate (100%). 43 out of 47 injections were intra-articular, indicating accuracy of 91.5% through lateral midpatellar portal. 41 out of 47 injections were intra-articular through anterolateral portal with accuracy of 87.4%. Therefore, our study showed that the accuracy of needle placement was higher through Lateral midpatellar than the Anterolateral portal, though there was no statistically significant difference as p>0.05 (p=0.503) [Table/Fig 3,4].
Comparison of accuracy rates through each portal.
| Portal | Total No of INJ | Intraarticular | Extraarticular | Accuracy Rate |
|---|
| Lat. Midpatellar | 47 | 43 | 4 | 91.5% |
| Anterolateral | 47 | 41 | 6 | 87.4% |
X2= 0.448 p=0.503 Not Significant.
Comparison between accuracy rates through lateral midpatellar and anterolateral portals.
Discussion
An accurate intra-articular needle placement in the knee joint is important for intra-articular treatment because it helps increase the effectiveness and minimize complications.
Our study evaluated accuracy of needle placement in patients undergoing treatment for Osteoarthritis with the absence of effusion through 2 portals: lateral midpatellar and anterolateral of which the sample subjects were randomly allocated equally into 2 groups. The accuracy rates compared indicated that the injection through Lateral midpatellar portal was more accurate (accuracy of 91.2%). The accuracy through anterolateral portal was 87.4% which was comparatively less than lateral midpatellar portal.
This is consistent to the findings reported in the study conducted by Jackson et al., [4]. The needle passes through a minimal amount of soft tissue to reach the intraarticular space through the lateral midpatellar. They found palpation of landmarks around knee was difficult due to the excess fat and also there was longer distance between skin and joint space. In this study including 80 injections performed through an anterolateral portal, 57 were confirmed to have been placed in the intra-articular space. (accuracy rate of 71%) when compared to 60 of 80 injections through an anteromedial approach (75% accuracy rate), and seventy-four of eighty injections through a lateral midpatellar portal (93% accuracy rate).
Fluoroscopic imaging was done in our study through injection of contrast material to confirm the intra-articular needle placement by documenting the dispersion pattern. However, in a study conducted by Bliddal, the intra-articular therapy was tested by Air-Arthrography reporting that fifty-one of fifty-six injections were intraarticular [7]. The patients with dry Osteoarthritis of the knee were treated with Triamcinolone. Our study showed that there were no significant differences in accuracy rates between approaches for patients classified with Kellgren-Lawrence scale grades II and III similar to the study done by Toda and Tsukimura [9]. The study by Toda and Tsukimura was done in 50 patients. The results of this study had more accuracy with modified Waddell approach (86%) followed by seated AM and lateral patellar approach which had accuracy rates of 62% and 70% respectively. The length of the needle used in our study was around 5cm which was longer as compared to this study (3.2cm) so as to sufficiently reach the intra-articular space as noted by Jackson et al., [4].
In contrast to our study, another study conducted by Park et al., evaluated the accuracy of needle placement through superolateral, midlateral and medial portals for K-L grading knees [10]. This study was conducted in 126 knees with Osteoarthritic knees graded as The Kellgren-Lawrence grade 2 and 3 cases each of which had accuracy rates of 100% and 100%, 97% and 90%, and 77% and 67% for the superolateral, midlateral and medial approaches respectively. Also, intra-articular approaches were sonographically guided. This study therefore showed accuracy between portals in patients classified as Kellengren-Lawrence grade 2 & 3 and highlighted on sonographically guided injections unlike our study.
Some studies have suggested that guidance of intra-articular needle position by imaging techniques may improve the accuracy. The costs and extra time associated with these techniques should be taken into consideration [11].
Some observations made during our study included the complaints of pain and discomfort from the patients during the procedure when there was incorrect extra-articular placement of the needle. This may also be associated with injection failure with reference to treatment especially in cases where hyaluronic acid is used as 100% accuracy is needed for its efficacy unlike corticosteroid injections. However, drug leakage or wrongly placed steroid injections have adverse effects [4,11,12].
The drawback of extra articular placing of injections was overcome by the use of fluoroscopic imaging which was done after injection of contrast material given subsequent to hyaluronic acid or corticosteroids, it confirms 100% intra-articular placement of the needle. Fluoroscopic imaging therefore was noted to have advantage over Sonography, as sonographically guided injections are more observer dependent investigations [12]. A study byDávila-Parrilla et al., suggested that palpation guided intra articular injection was clinically as efficient as image guided one [13]. However, this study did not look into accuracy.
Further studies which include all the 3 portals – anterolateral, anteromedial and lateral midpatellar can be done as our study evaluated accuracy rates only through 2 portals. Also, in our study we could not relate any association between K-L grading and the intra-articular placement which can be a limiting factor, as the approach accuracy might vary depending on the severity of osteoarthritic knees.
Conclusion
Needle placement through lateral midpatellar portal has increased chances of going intra-articular when compared to anterolateral. Guidance of intra-articular needle placements by fluoroscopic imaging techniques enhance the accuracy and thereby reduce the extra-articular needle placement increasing the efficacy of treatment. However, the cost and extra time associated with these techniques must always be taken into consideration for implementation in daily life.
X2= 0.448 p=0.503 Not Significant.
[1]. Kotevoglu N, Lyibozkurt PC, Hiz O, Toktas H, Kuran B, A prospective randomized controlled clinical trial comparing the efficacy of different molecular weight hyaluronan solutions in the treatment of knee osteoarthritisRheumatol Int 2006 26:325-30. [Google Scholar]
[2]. Marshall KW, Intra-articular hyaluronan therapyFoot Ankle Clin 2003 8(2):221-32. [Google Scholar]
[3]. Lussier A, Cividino AA, McFarlane CA, Olszynski WP, Potashner WJ, De Médicis R, Viscosupplementation with hylan for the treatment of osteoarthritis: findings from clinical practice in CanadaJ Rheumatol 1996 23:1579-85. [Google Scholar]
[4]. Jackson DW, Evans NA, Thomas BM, Accuracy of needle placement in the intra-articular space of the kneeJ Bone Joint Surg Am 2002 84-A(9):1522-27. [Google Scholar]
[5]. Abate M, Pulcini D, DiIorio A, Viscosupplementation with intra-articular hyaluronic acid therapy for treatment of osteoarthritis in elderlyCurr Pharm Des 2010 16(6):63 [Google Scholar]
[6]. Daley EL, Bajaj S, Bisson LJ, Cole BJ, Improving injection accuracy of the elbow, knee and shoulder: does injection site imaging make a difference, a systematic reviewAm J Sports Med 2011 39(3):656-62. [Google Scholar]
[7]. Bliddal H, Placement of intra-articular injections verified by mini-air arthrographyAnn Rheum Dis 1999 58:641-43. [Google Scholar]
[8]. Jones A, Regan M, Ledingham J, Pattrick M, Manhire A, Doherty M, Importance of placement of intra-articular steroid injectionsBMJ 1993 307:1329-30. [Google Scholar]
[9]. Toda Y, Tsukimura N, A comparison of intra-articular hyaluronan injection accuracy rates between three approaches based on radiographic severity of knee osteoarthritisOsteoarthritis Cartilage 2008 16:980-85. [Google Scholar]
[10]. Park Y, Lee SC, Nam HS, Lee J, Nam SH, Comparison of Sonographically Guided intra-articular injections at 2 different sites of the kneeJ Ultrasound Med 2011 30(12):1669-76. [Google Scholar]
[11]. Douglas RJ, Aspiration and Injection of the Knee Joint: Approach PortalKnee Surg Relat Res 2014 26(1):1-6. [Google Scholar]
[12]. Hermans, J, Bierma-Zeinstra S, Bos PK, The Most Accurate Approach for Intra-ArticularNeedle Placement in the Knee Joint: A Systematic ReviewSemin Arthritis Rheum 2011 41:106-15. [Google Scholar]
[13]. Dávila-Parrilla A, Santaella-Santé B, Otero-López A, Does Injection Site Matter? A Randomized Controlled Trial to Evaluate Different Entry Site Efficacy of Knee Intra- InjectionsBol Asoc Med PR 2015 107(2):78-81. [Google Scholar]