Implant – Supported Full Mouth Rehabilitation: A Guided Surgical and Prosthetic Protocol
Segin Chandran1, Nasil Sakkir2
1 Associate Professor, Department of Oral and Maxillofacial Surgery, SMCSI Medical College, Karakonam, Thiruvananthapuram, Kerala, India.
2 Private Practice, Department of Endodontics and Implantology, Kamala Dental Speciality Hospital, Thiruvananthapuram, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Segin Chandran, Aardram”, Tc 16/686 (1) Kochar Road, Jagathy JN., Thiruvananthapuram, Kerala-695014, India. E-mail : seginchandran@gmail.com
CAD - CAM restorations, Dental implants, Flapless implant surgery, Surgical template, Stereolithography
Introduction
A 60-year-old female patient presented with multiple missing teeth and advanced periodontal disease. Preoperative clinical and radiographic examination revealed that all her remaining teeth were periodontally compromised with Grade III mobility [Table/Fig-1]. She had no history of allergies or any other medical illness. The treatment plan was extraction of all her teeth and its replacement with maxillary and mandibular removable complete dentures. The patient was very keen on having a fixed prosthesis in order to avoid wearing the conventional removable dentures. A total extraction of all her teeth was performed along with alveolectomy and ridge reduction to obtain an optimum prosthetic platform. After initial healing period of 2 weeks, the impressions were taken and an interim denture was made. The transition of interim denture to Procera Implant Bridge (PIB) took around 40 days to complete stereolithographic surgical template, guided surgery and prosthetic rehabilitation.
Preoperative OPG showing mutilated dentition.

Treatment Planning for Guided Surgery
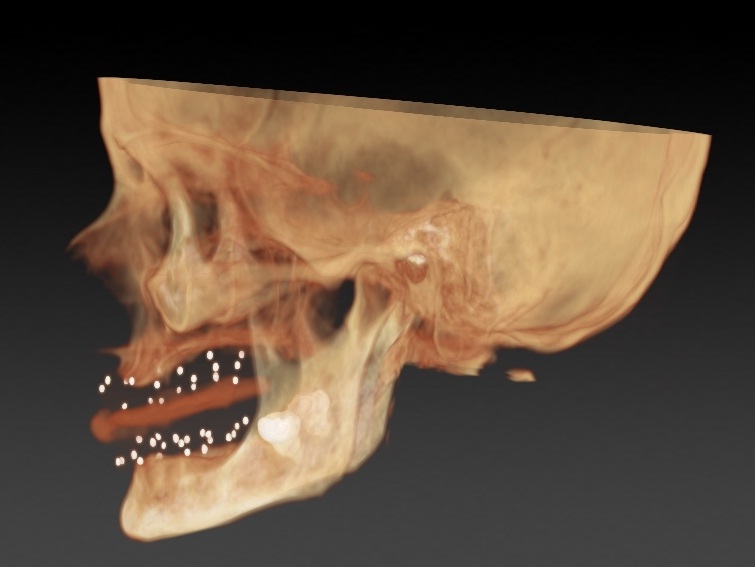
The interim complete dentures were duplicated and six holes of 1.5 mm diameter and 1 mm depth were made at different heights on both upper and lower dentures on both flanges – labial & lingual. Gutta percha was used to fill these holes, so as to precisely locate the position of denture and teeth during the CT scan. From the existing complete dentures, bite registration was carried out using Vinyl poly siloxane bite registration paste with 2 mm spacing (O–bite, DMG, Hamburg). The dentures were attached to the bite registration during the three dimensional scanning of the patient. In the primary scan, the bone window of the patient’s jaws and gutta percha markings of dentures were visible [Table/Fig-2]. Another CT scan of maxillary and mandibular dentures was made separately (Double-scan technique). This enabled visualization of dentures with gutta percha markings. These markings were used to over lay the visible denture on to the bone window of the jaws.
CT image showing radiographic markers.
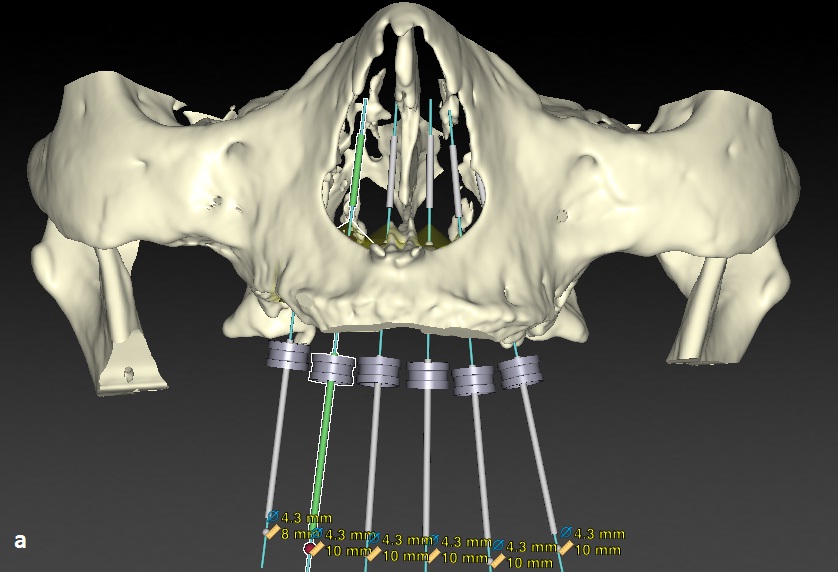
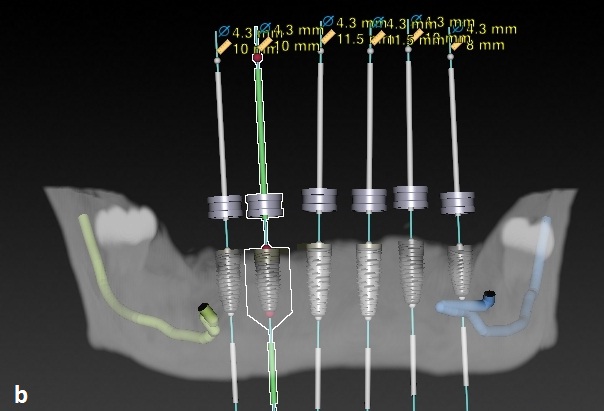
The implant planning software (Nobel Clinician, Nobel Biocare, Switzerland) merges the scanned image of the denture and the bone window of the jaws in a DICOM (Digital Imaging and Communication in Medicine) format. With reference to the teeth position in denture, the locations, sizes of implants in the bone were determined for better prosthetic outcome. The depth, diameter and parallelism were reassessed and corrected using the software [Table/Fig-3a&b]. Once implant selection and positioning were confirmed, the data was send to a rapid prototyping centre in Sweden to fabricate a stereolithographic surgical guide.
Virtual implant placements in maxilla.
Virtual implant placements in mandible.
Surgical Procedure
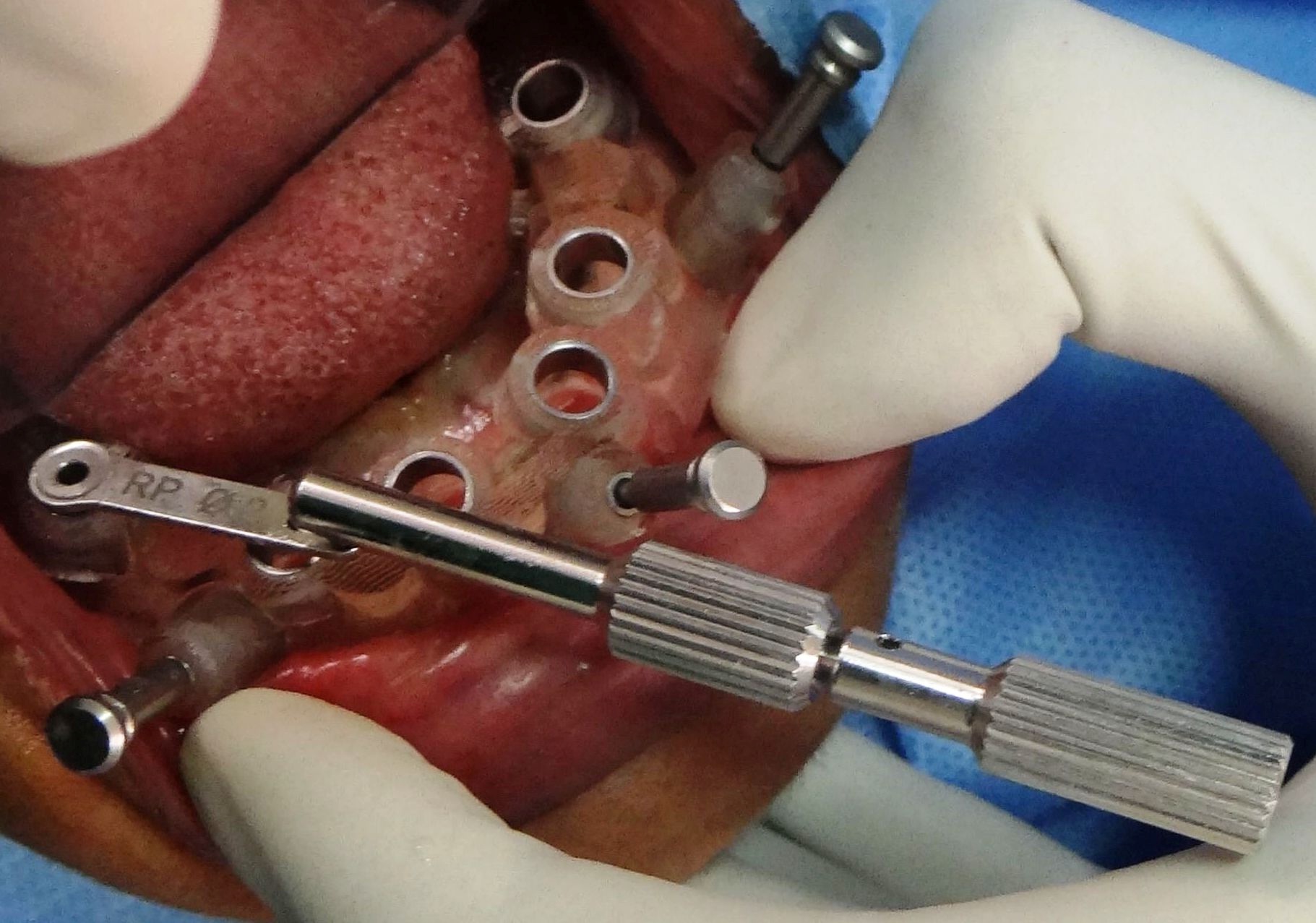
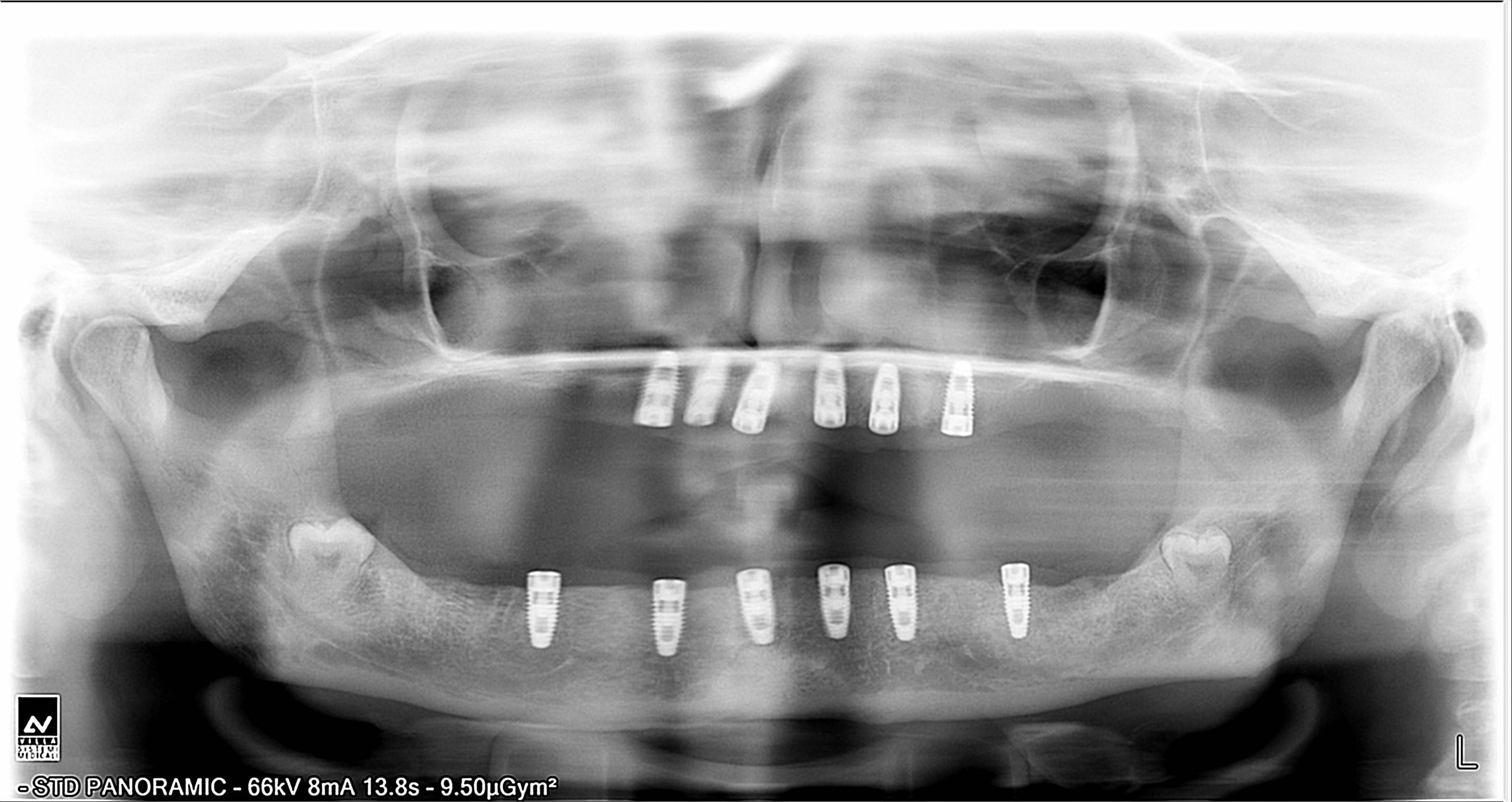
After anaesthesia, the maxillary surgical guide was secured over the edentulous maxilla by transfixing the guide flanges through gingival tissues using stabilizing pins. Implant osteotomy was carried out in a sequential manner starting from 2 mm pilot drill with corresponding drill reducer over layed on the drill housing. Six Nobel Biocare Groovy implants (Regular Platform - 4.3mm) were placed in the final osteotomy sites. Because of good bone quality and precise osteotomy, the insertion torque for all implants were in a range of 45-60N. The cover screws were torqued to 15N and the surgical guide was removed. The same procedure was carried out in the mandible and six Nobel Biocare Groovy implants (Regular Platform - 4.3mm) were placed [Table/Fig-4,5]. The immediate post-surgical OPG confirms the accurate placement of implants [Table/Fig-6]. The surgical duration was less than 30 minutes for each jaw and there was faster uneventful healing.
Mandibular surgical template with drill reducer.
Flap-less implant placements in mandible.

OPG after implant placements.
Prosthetic Procedure
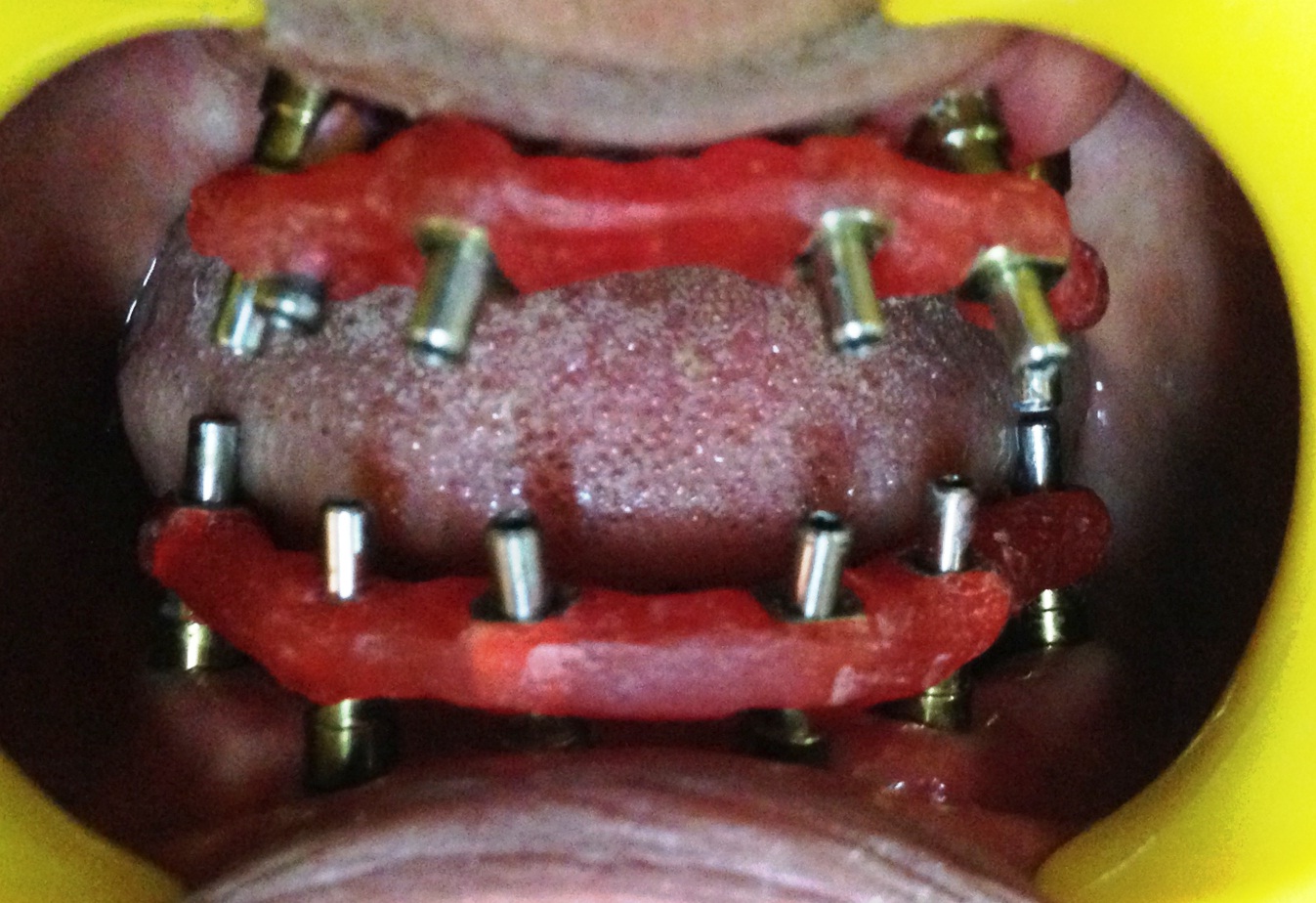
Open tray impressions were taken with impression copings splinted together using pattern resin [Table/Fig-7]. The lab analogues were attached and the impressions were send to the lab. The positioning jig received from the lab was tried in the patient’s mouth to confirm its accuracy [Table/Fig-8]. The double tray wax rims were used to determine the jaw relation and sealed using O-bite, bite registration paste. The same was transferred to a semi adjustable articulator. The scanned master cast along with bite registration was send to CAD-CAM milling centre to make a Procera Implant Bridge (PIB) framework. The framework was then acrylized to obtain the final screw retained prosthesis. The finished prosthesis was temporarily fixed to verify the implant protected occlusion in centric relation [Table/Fig-9]. The precise fit of the prosthesis was verified radiographically [Table/Fig-10].
Open tray impression copings in mandible.

Pattern resin jig trial in patient’s mouth.
Final hybrid prosthesis in place.


Discussion
Computer-aided design (CAD)/computer-aided machining (CAM) based surgical templates that incorporate drill housings helps in precise placement of implants even without flap elevation [1]. Less intraoperative bleeding, decreased postoperative patient discomfort and better wound healing are the advantages of flapless implant procedure [2,3]. The Procera Implant Bridge (PIB) made of titanium was used for prosthetic rehabilitation. CAD-CAM based restoration using PIB ensures high levels of prosthetic accuracy compared to conventional casted frameworks [4].
[1]. Jabero M, Sarment DP, Advanced surgical guidance technology: A reviewImplant Dent 2006 15:135-42. [Google Scholar]
[2]. Fortin T, Bosson JL, Isidori M, Blanchet E, Effect of flapless surgery on pain experienced in implant placement using an image guided systemInt J Oral Maxillofac Implants 2006 21:305-13. [Google Scholar]
[3]. Orentlicher G, Abboud M, Guided surgery for implant therapyDent Clin North Am 2011 55:715-44. [Google Scholar]
[4]. Drago C, Howell K, Concepts for designing and fabricating metal implant frameworks for hybrid implant prosthesisJ Prosthodont 2012 21(5):413-24. [Google Scholar]