Autotransplantation of a Buccally Erupted Matured Mandibular Third Molar to Replace a Grossly Decayed Second Molar
Sukhwant Singh Yadav1, Ranjeet Bodh2, Aishvarya Kaushik3, Sangeeta Talwar4
1 Senior Resident, Department of Conservative Dentistry & Endodontics, Maulana Azad Institute of Dental Sciences, New Delhi, India.
2 Senior Resident, Department of Oral & Maxillofacial Surgery, Maulana Azad Institute of Dental Sciences, New Delhi, India.
3 Senior Resident, Department of Conservative Dentistry & Endodontics, Maulana Azad Institute of Dental Sciences, New Delhi, India.
4 Professor and Head, Department of Conservative Dentistry & Endodontics, Maulana Azad Institute of Dental Sciences, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sukhwant Singh Yadav, 3rd Floor, Maulana Azad Institute of Dental Sciences, Mamc Complex, B.S. Jafar Marg, New Delhi-02, India.
E-mail: sukhwant.yadav@gmail.com
Autotransplantation can be a treatment option for tooth loss as an alternative to fixed or implant-supported prostheses. It has predictable results comparable to implants, with reported success rates often greater than 90%. In present case, buccally erupted matured third molar was autotransplanted in extraction socket of grossly carious mandibular second molar. The tooth was splinted for 1 week followed by root canal treatment. After 12 months follow up, tooth was in perfect state of function and aesthetic with healthy periapical and periodontal architecture. High success rate was found in immature tooth transplantation in previous case reports. This case report describes that even matured tooth can also be used as donor if atraumatic extraction is possible and endodontic treatment is well performed.
Atraumatic extraction, Endodontic treatment, Implant
Case Report
A 28-year-old woman was referred to the Department of Conservative Dentistry & Endodontics, Maulana Azad Institute of Dental Sciences, for evaluation of the right mandibular second molar. The medical history was non-contributory. On clinical examination, extensive caries in tooth 47, buccally erupted third molar in same quadrant and healthy oral soft tissues was found. Considering the poor prognosis of 47, availability of donor tooth and the involved treatment costs of alternative treatment options like implant, autotransplantation of third molar was planned. Clinical [Table/Fig-1a] and radiological [Table/Fig-2a] examinations confirmed the feasibility of the donor and recipient sites.
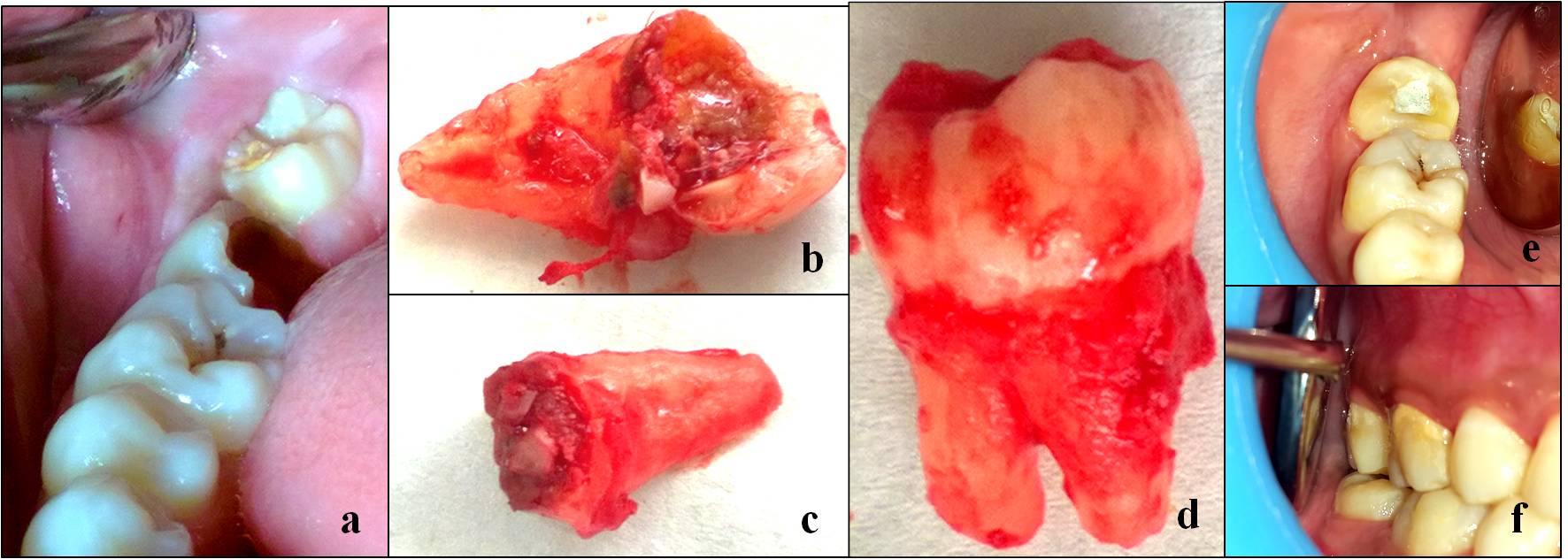
a) Preoperative picture showing grossly decayed second molar and buccally erupted third molar; b&c) extracted roots of second molar; d) extracted third molar; and e&f) 12 months follow up picture showing healthy autotransplanted third molar in occlusion
a) Preoperative radiograph depicting grossly decayed second molar and matured third molar with straight roots; b) postoperative radiograph showing well obturated root canals and extruded metapex in periapical tissues; c) 12 months follow up with healed socket and healthy periodontal tissues around transplanted tooth.

Tooth 47 was extracted in two pieces [Table/Fig-1b&c] under local anaesthesia under aseptic conditions. Buccally erupted third molar extraction [Table/Fig-1d] was done thereafter and placed immediately in extraction socket. There was no need for adaptation or socket preservation due to the smaller size of the wisdom tooth compared to the second molar. Implanted tooth was splinted for 1week. Occlusal adjustments were done after 24 hours. Endodontic treatment was performed under rubber dam (Hygienic Dental Dam, Coltène/ Whaledent Inc., Cuyahoga Falls, USA) after one week. Two canal orifices (mesial and distal) were located with an endodontic explorer (DG-16). The working length was determined with electronic apex locator (J. Morita USA, Inc.: Root ZX II) and confirmed radiographically. Canals were prepared with protaper rotary file system with crown down pressure-less technique. The root canals were copiously irrigated with 5.25% sodium hypochlorite solution (Hyposol, Prevest Denpro Limited, Jammu, India). Intracanal medicament metapex was placed for two weeks. Obturation was performed in next visit with gutta-percha and AH Plus (Dentsply Limited, Surrey, United Kingdom) using a warm vertical condensation technique [Table/Fig-2b]. The patient was recalled for periodic follow-ups. The recall examination after 12 months revealed asymptomatic and healthy periodontal conditions. At this time, the tooth showed no sensitivity to palpation or percussion and the probing depth was normal. No abnormality was detected in radiography [Table/Fig-2c] and the tooth was completely functional [Table/Fig-1e&f].
Discussion
Management of grossly decayed teeth with questionable restorability is a big challenge in dentistry. It can be replaced by removable or fixed partial denture. Removable prosthesis cause discomfort to patient, while fixed partial denture leads to tooth preparation of healthy teeth. Implant is a reliable substitute for missing tooth but as it involves lot of risk factors and long span of treatment, auto transplantation can be considered as a good treatment option. Autogenous tooth transplantation or autotransplantation is the surgical movement of a tooth from one location in the mouth to another in the same individual. It has achieved high success rates and is an excellent option for tooth replacement [1]. Some preoperative and postoperative factors including root development, position of the tooth, and surgical technique influence the prognosis of successful autotransplantation [2].
Mandibular third molar used as a donor for transplantation was buccally erupted and out of occlusion. Such teeth which are not in function can be used as donor teeth. Recipient site has an extensively carious non-restorable molar. Tooth agenesis (especially of premolars and lateral incisors), traumatic tooth loss, ectopic eruption of canines, root resorption, large endodontic lesions, cervical root fractures, localized juvenile periodontitis are the other indications for auto transplantation [3]. Third molar can be autotransplanted for closure of oro-antral communications [4]. Successful transplantation depends on specific requirements of the patient, the donor tooth, and the recipient site. Patient should be healthy, free of systemic diseases and compliant for follow ups [1]. Immature teeth with more than two third root formation are better than matured teeth as donors [5]. Vertical bone growth can also occur in matured donors if viability of the periodontal ligament cells is maintained [6]. A tooth with complete or near complete root formation will generally require root canal therapy, while a tooth with an open apex will remain vital and continue root development after transplantation. Atraumatic surgical extraction should be performed to preserve viable periodontal ligaments. Recipient site should have adequate bone support and should be free from inflammatory and infected tissue for better success of transplantation [7]. Inflammatory root resoprtion is the complication of this procedure which can lead to failure of transplant [8]. Calcium hydroxide based medicament should be placed intracanal to prevent resorption [9]. Yoshino et al., found that periodontal attachment loss (54.9%), root resorption (26.5%), dental caries (4.0%), root fracture (2.9%) and others (11.8%) are causes of autotransplanted tooth loss [10]. Long follow ups are required to check the clinical and radiographical success of autotransplantation. Implants are better option than autotransplants because of their high success rate and feasibility. But autotransplantation is an economical option for an edentulous space or grossly decayed tooth because the procedure is performed in one stage and no prosthesis is required [11]. Successful tooth auto transplantation offers improved aesthetics, arch form, dentofacial development, mastication, speech and arch integrity. Maintenance of the morphology of alveolar ridge through proprioceptive stimulation is main advantage over implant [12]. Unavailability of donor tooth and absence of long term success in literature as compared to implant are some limitations of autologous autotransplantation.
Conclusion
Autotransplantation when feasible is a viable economical option for grossly decayed teeth but its high success in matured donor teeth is yet to be established.
[1]. Clokie CML, Yau DM, Chano L, Autogenous tooth transplantation: an alternative to dental implant placement?J Can Dent Assoc 2001 67:92-96. [Google Scholar]
[2]. Schwartz O, Bergmann P, Klausen B, Autotransplantation of human teeth: a life-table analysis of prognostic factorsInt J Oral Surg 1985 14:245-58. [Google Scholar]
[3]. Kristerson L, Lagerström L, Autotransplantation of teeth in cases with agenesis or traumatic loss of maxillary incisorsEur J Orthod 1991 13:486-92. [Google Scholar]
[4]. Nagori SA, Jose A, Bhutia O, Roychoudhury A, A case of oro-antral communication closed by autotransplantation of third molarJ Maxillofac Oral Surg 2015 14(Suppl 1):448-51. [Google Scholar]
[5]. Andreasen JO, Autotransplantation of molarsIn: Atlas of replantation and transplantation of teeth 1992 PhiladelphiaWB Saunders Company:111-34. [Google Scholar]
[6]. Kim S, Lee SJ, Shin Y, Kim E, Vertical bone growth after autotransplantation of mature third molars: 2 case reports with long-term follow-upJ Endod 2015 41:1371-74. [Google Scholar]
[7]. Northway WM, Konigsberg S, Autogenic tooth transplantation the “state of the art”Am J Orthod 1980 77:146-62. [Google Scholar]
[8]. Teixeira CS, Pasternak B, Vansan LP, Sousa-Neto MD, Autogenous transplantation of teeth with complete root formation: two case reportsInt Endod J 2006 39:977-85. [Google Scholar]
[9]. Trope M, Yesilsoy C, Koren L, Moshonov J, Friedman S, Effect of different endodontic treatment protocols on periodontal repair and root resorption of replanted dog teethJ Endod 1992 18:492-96. [Google Scholar]
[10]. Yoshino K, Kariya N, Namura D, Noji I, Mitsuhashi K, Kimura H, A retrospective survey of autotransplantation of teeth in dental clinicsJ Oral Rehabil 2012 39:37-43. [Google Scholar]
[11]. Baviz JB, Autotransplantation of teeth: a procedure that gets no respectOral Surg Oral Med Oral Pathol Oral Radiol Endod 2010 110:441 [Google Scholar]
[12]. Hernandez SL, Cuestas-Carnero R, Autogenic tooth transplantation: a report of ten casesJ Oral Maxillofac Surg 1988 46:1051-55. [Google Scholar]