Images in Medicine: Triplicated Primary Anterior Teeth - A Report of Two Cases
Deepti Thakkar1, Jatinder Kaur Dhillon2, Mridula Goswami3
1 Senior Resident, Department of Pedodontics & Preventive Dentistry, Maulana Azad Institute of Dental Sciences, New Delhi, India.
2 Assistant Professor, Department of Pedodontics & Preventive Dentistry, Maulana Azad Institute of Dental Sciences, New Delhi, India.
3 Professor and Head of Department, Department of Pedodontics & Preventive Dentistry, Maulana Azad Institute of Dental Sciences, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepti Thakkar, Senior Resident, Department of Pedodontics & Preventive Dentistry, Maulana Azad Institute of Dental Sciences, New Delhi, India.
E-mail: dr.deeptithakkar@gmail.com
CBCT, Fusion, Supernumerary tooth, Triple teeth
Fusion is the union of two separate tooth buds during their development. The pulp chamber and root canal may be joined or separated, depending on the stage of development at the time of union [1]. Though fusion between two teeth is a common finding in primary dentition, occurrence of tooth triplet due to fusion of three teeth is a relatively rare occurrence with the reported prevalence of 0.02% in the primary dentition [2]. This paper presents two cases of unilateral triplication of primary anterior teeth due to fusion of primary anterior teeth with a supernumerary tooth.
Case 1
A five year-old male reported with the chief complaint of pain in the upper front tooth region. Intraoral examination revealed that the maxillary left central incisor was carious and larger than normal and lateral incisor was missing. A soft, non-fluctuant, tender swelling of size approximately 1cm x 1cm was also noted suggestive of periapical abscess. An intraoral periapical radiograph of the maxillary anterior region was taken [Table/Fig-1].
Intraoral frontal view showing abscess in relation to grossly decayed tooth and Intra oral periapical radiograph showing fused teeth (Case 1).

The radiograph revealed three distinct crown outlines while the root outlines were indistinguishable. An ill-defined periapical radiolucency extending to the dental follicle of tooth no. 21 was also evident. Since clinical and periapical radiographic findings were inconclusive, a dental CBCT scan (Medium FOV) was performed. Image processing in 3-D was performed with On-Demand 3DTM software [Table/Fig-2].
CBCT images showing fusion between tooth no. 61,62 and supernumerary tooth (Case 1).
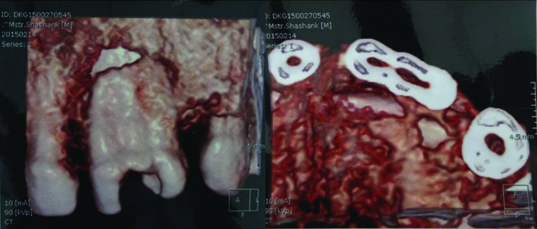
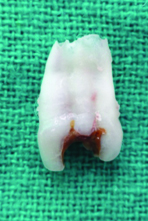
Cross sectional interval was 1.5 mm. It revealed the mesiodistal root width of the macrodont as approximately 9.6 mm with smooth labial and palatal margins and presence of two grooves equidistant to each other. However, the mesiodistal width of the contralateral central incisor was 4.0 mm and lateral incisor was 3.7 mm; thus, indicating that more than two teeth were fused. The diagnosis of triple teeth, i.e., fusion between the maxillary left primary central and lateral incisor along with a supernumerary tooth was confirmed. The treatment plan aimed at removal of the offending tooth under local anaesthesia [Table/Fig-3] followed by anterior space maintainer and regular recall visits [Table/Fig-4].
Extracted tooth showing two distinct grooves demarcating the points of fusion between the three teeth (Case 1).
Postoperative frontal view with functional removable space maintainer in relation to 61,62 (Case 1).

Case 2
A five-year-old male reported to the department and routine intra oral examination revealed the maxillary right central and lateral incisor fused with a supernumerary tooth and a carious lesion on the palatal aspect at the line of fusion of the central incisor with supernumerary tooth. An IOPA radiograph of the maxillary anterior region was taken [Table/Fig-5].
Intraoral view showing maxillary right central and lateral incisor fused with a supernumerary tooth with a carious lesion on the palatal aspect and Intraoral periapical radiograph showing fused teeth (Case 2).
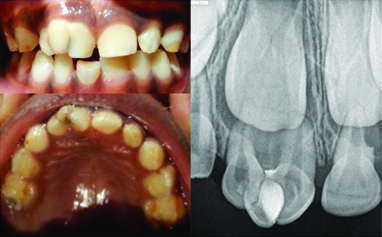
The radiograph revealed three distinct crown and root outlines. The carious lesion was removed and tooth was subsequently restored with composite [Table/Fig-6]. Oral hygiene instructions were given.
Postoperative picture showing composite restoration in relation to the fused tooth.(Case 2)

In the first case, incomplete fusion was seen as evidenced by distinct root canals although the roots and crown structure were fused. A CBCT scan maxilla was done since the clinical and radiographic picture were inconclusive of the nature of the nature of fusion. The CBCT provides a 3-D volumetric data with high image accuracy, lesser scan time, lesser radiation dose as compared to conventional CT scan and a less complicated apparatus thereby reducing the anxiety in children [3]. The second case also represented incomplete fusion joined by dentine with separate pulp chambers and root canals.
Shilpa G and Nuvvula S proposed a classification of triple teeth according to the morphology of teeth involved in fusion as given in [Table/Fig-7] [4]. As per this classification, both cases can be classified as Type Ia where two normal teeth i.e. maxillary central & lateral incisor, are fused with a supernumerary tooth.
Classification of triple teeth [4].
| Type | Description |
|---|
| Type I: Three pulp chambers and three root canals |
| Type Ia | Fusion of two normal teeth with a supernumerary tooth |
| Type Ib | Fusion of three normal teeth |
| Type II: Two pulp chambers and two root canals |
| Type IIa | Fusion of geminated tooth with a supernumerary tooth |
| Type IIb | Fusion of geminated tooth with a normal tooth |
Fused teeth may contribute to esthetic concerns, space problems, oral hygiene maintenance problems, occlusal disturbances and delayed eruption of the permanent successors [5,6].
Management of fused teeth includes observation of normal exfoliation if asymptomatic, restoration of deep grooves, periodontal and orthodontic correction if required, endodontic therapy or extraction if symptomatic with pulpal involvement.
[1]. Neville BW, Damm DD, Allen CM, Bouquot JE, Abnormalities of teethIn: Oral and Maxillofacial Pathology 2005 2nd edNew DelhiElsevier:49-106. [Google Scholar]
[2]. Ravn JJ, Aplasia, supernumerary teeth and fused teeth in the primary dentition. An epidemiologic studyScand J Dent Res 1971 79(1):1-6. [Google Scholar]
[3]. Dhillon JK, Kalra G, Cone beam computed tomography: An innovative tool in pediatric dentistryJournal of Pediatric Dentistry 2013 1(2):27-31. [Google Scholar]
[4]. Shilpa G, Nuvvula S, Triple tooth in primary dentition: a proposed classificationContemp Clin Dent 2013 4(2):263-7. [Google Scholar]
[5]. Yuen SW, Chan JC, Wei SH, Double primary teeth and their relationship with the permanent successors: a radiographic study of 376 casesPaediatr Dent 1987 9:42-48. [Google Scholar]
[6]. Nunes E, de Moraes IG, de Oliviera Novaes PM, de Sousa SMG, Bilateral fusion of mandibular second molars with supernumerary teeth: Case ReportBraz Dent J 2002 13:137-41. [Google Scholar]