Martin–Gruber Anastomosis- A Cadaveric Study in North Indian Population
Neelamjit Kaur1, Rajan Kumar Singla2, Jagdev Singh Kullar3
1 Associate Professor, Department of Anatomy, Maharishi Markandeshwar Medical College & Hospital, Solan, India.
2 Professor and Head, Department of Anatomy, Government Medical College, Patiala, India.
3 Additional Professor, Department of Anatomy, Government Medical College, Amritsar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Neelamjit Kaur, Associate Professor, Department of Anatomy, Maharishi Markandeshwar Medical College & Hospital, Solan, India.
E-mail: neelamjit@yahoo.co.in
Introduction
Communications between peripheral nerves are important in the light of the fact that these are responsible for a myriad of clinical symptoms. Communication between the median nerve and ulnar nerve (Martin-Gruber anastomosis) is a frequent finding observed anatomically in 10%-30.6% subjects and physiologically in 5-40%. It may lead to exacerbated or attenuated clinical symptoms.
Aims & Objectives
To find out the incidence of Martin-Gruber anastomosis in North Indian population by cadaveric dissection.
Materials and Methods
The material comprised of 60 upper limbs belonging to 30 cadavers (M:F::28:2) which were dissected to find out incidence of Martin-Gruber anastomosis.
Results
Martin-Gruber anastomosis was encountered in 7(11.6%) limbs of the present study. It was seen more frequently unilaterally (16.6%) than bilaterally (3.3%) and only in males. Classification of limbs into various patterns and types was done. Further its ontogeny, phylogeny, genetic inheritance and clinical implications are discussed in detail.
Conclusion
To conclude, in North Indian population, the Martin-Gruber anastomosis is encountered in 11.6% limbs.
Median nerve, Nerve communications, Ulnar nerve
Introduction
Brachial plexus and its branches depict numerous variant which have been reported by different workers [1,2]. One such variant is crossing over of nerve fibres between different branches of brachial plexus like between median nerve and musculocutaneous nerve and between median nerve and ulnar nerve. The communicating ramus in the later group i.e. between median nerve & ulnar nerve may be of following types-:
(a)A communicating ramus from median nerve to ulnar nerve in the forearm, the so called Martin-Gruber anastomosis.
(b)Ulnar to median nerve communication in the forearm, so called reversed Martin-Gruber Anastomosis or Marinacci communication.
(c)The Riche-Cannieu anastomosis occurs in the palm between recurrent branch of median nerve & deep branch of ulnar nerve.
(d) The communicating ramus between the common digital nerves that arise from ulnar & median nerve in the palmar surface of hand is known as Berretini anastomosis [3].
Out of these four types, the first i.e. Martin-Gruber anastomosis is commonest and most important too. It was first described by the Swedish anatomist Martin [4] and later by Gruber [5] and thus named as Martin-Gruber Anastomosis. It consists of a communicating ramus which leaves either the main trunk of median nerve or its anterior interosseous branch and join the main trunk of ulnar nerve to ultimately innervate the intrinsic hand muscles [6]. Its incidence varies between the anatomical & physiological studies. In anatomical studies it is found in 10%-30.6% [7–11] while in physiological studies the range becomes wider to 5%-40% [12–14]. It has been also noted that the unilateral Martin-Gruber anastomosis is more often seen on right side as compared with left side [8,12,10]. However, no sexual dimorphism is seen [6], though an autosomal dominant inheritance is observed [13].
Clinically the Martin-Gruber anastomosis may lead to misdiagnosis of conditions affecting the nerve supply of upper limb muscles like carpal tunnel syndrome, cubital tunnel syndrome and leprosy neuropathy. Understanding the existence of this variation, its location and its possible presentation is important for correct patient assistance [15]. Similarly, in lesions proximal to the communication, the motor and sensory innervation remains normal and also in complete lesion of median nerve some muscles innervated by median nerve may not be paralysed leading to erroneous conclusion [16]. Martin-Gruber anastomosis has also been implicated clinically in anomalous innervations of muscle or skin and in anomalous nerve conduction observed during electrophysiological studies. If the anaesthetized nerve has intramuscular course then it is a potential compression site and thus carries additional clinical implication [17,18].
Thus an anatomical investigation of topography of Martin-Gruber anastomosis is very important for understanding motor, sensory and autonomic dysfunctions. So this study was designed on embalmed cadavers to find out the incidence and topography of this variant in North Indian population.
Materials and Methods
The material of the present study comprised of 60 upper extremities of 30 well embalmed adult human cadavers (M:F::28:2) obtained from Department of Anatomy, Government Medical College, Amritsar during the period from 2007-2009. These were serialized from 1-30 with suffix ‘R’ for right and ‘L’ for left extremity and M or F for male and female sex respectively. The median nerve was exposed from formation till termination as per the dissection steps given in Cunningham’s Manual of Practical Anatomy [19]. Similiarly ulnar nerve was traced till its termination. The Martin-Gruber anastomosis was identified, cleared and photographed where ever possible.
Results
Out of the 30 cadavers, in one cadaver (17M), Martin-Gruber anastomosis was found in both the upper limbs (3.33%). Apart from this in five more limbs it was found unilaterally. Out of these five limbs three belonged to the right side and two belonged to the left side. Thus in toto out of 60 limbs of the present study it was seen in seven limbs (11.6%).
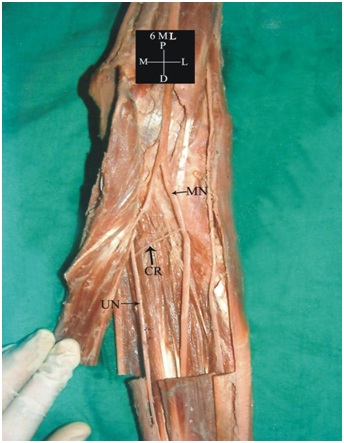
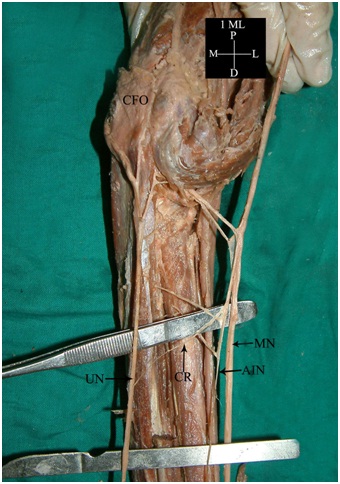
Out of the seven limbs with Martin-Gruber anastomosis, in two limbs (6ML&17MR) it was located in the forearm between main trunk of median nerve and main trunk of ulnar nerve [Table/Fig-1] while in the rest, it was from anterior interosseous nerve to ulnar nerve [Table/Fig-2]. The course of communicating ramus was oblique starting from median nerve or anterior interosseous nerve proximally and going to ulnar nerve distally in all the variant limbs [Table/Fig-1,2].
Communicating ramus (CR) (Martin-Gruber Anastomosis) from main trunk of median nerve (MN) to main trunk of ulnar nerve (UN).
Communicating ramus (CR) (Martin-Gruber Anastomosis) from anterior interroseous nerve (AIN) to main trunk of ulnar nerve (UN). {Branches from anterior interroseous nerve (AIN) to Flexor digitorum profundus (FDP) are also seen}.
Discussion
As observed earlier, Martin-Gruber anastomosis was seen more frequently unilaterally (16.6%) as compared with bilaterally (3.3%). In unilateral limbs, it was found more on right side as compared with left side. This was in consonance with the earlier studies that unilateral Martin-Gruber anastomosis is more common on right side [8,10,12]. All the limbs in which Martin-Gruber anastomosis was seen belonged to male sex but it could be attributed to the fact that out of 30 cadavers of the present study, 28 belonged to the male sex. It was seen in seven (11.6%) limbs of the present study. [Table/Fig-3] compares its incidence with the earlier studies.
Incidence of martin-gruber anastomosis.
| S.No | Authors | Year | Number Of Limbs Studied | Incidence (%) |
|---|
| 1. | Gruber [5] | 1870 | 250 | 15.2% |
| 2. | Kayamori [20] | 1987 | 1200 | 9.7% |
| 3. | Nakashima [7] | 1993 | 108 | 21% |
| 4. | Prates et al., [21] | 2003 | 64 | 7.8% |
| 5. | Felippe et al., [22] | 2012 | 30 | 10% |
| 6. | Present study | 2015 | 60 | 11.6% |
Nidenfuhr et al., (based on a study of 70 human cadavers) have classified Martin-Gruber anastomosis in 2 patterns with each pattern further subdivided into 3 types as follows [23]:
Pattern I-Anastomosis made by only one branch.
Pattern II- Anastomosis made by two branches.
Both these patterns are further classified into 3 types, each depending upon origin of communicating ramus from median nerve or its branch as follows:
Type a-Communicating ramus originates from branch to superficial forearm flexors-47.3%.
Type b-Communicatng ramus originates from main trunk of median nerve-10.6%.
Type c- Communicatng ramus originates from anterior interosseous nerve-31.6%.
Accordingly in the present study, only Pattern I was seen and within this pattern two limbs (28.5%) fall into Pattern I type b & five limbs (71.4%) in pattern Ic, with no limb in Pattern Ia. [Table/Fig-4] compares the incidence of different patterns and types as reported by earlier workers.
Incidence of martin-gruber anastomosis.
| Author | Year | Pattern I (%) | Type Ia (%) | Type Ib (%) | Type Ic (%) | Pattern II (%) |
|---|
| Gruber [5] | 1870 | 95 | 13 | 8 | 74 | 5 |
| Thomson [24] | 1893 | 100 | 3 | 19 | 78 | 0 |
| Hirsawa [25] | 1931 | 50 | 15.40 | 0 | 34 | 50 |
| Srinivasan & Rhodes [26] | 1981 | 100 | 6 | 3 | 91 | 0 |
| Nakashima [7] | 1993 | 95.95 | 0 | 4.35 | 91.30 | 4.35 |
| Taams [8] | 1997 | 100 | 7 | 0 | 93 | 0 |
| Shu et al., [10] | 1999 | 64 | 0 | 17.60 | 47.10 | 35.30 |
| Niendefuhr et al., [23] | 2002 | 89.50 | 47.3 | 10.60 | 31.60 | 10.50 |
| Prates et al., [21] | 2003 | 100 | 0 | 20 | 80 | 0 |
| Present Study | 2015 | 100 | 0 | 28.50 | 71.40 | 0 |
Ontogeny- The variations in the nerve patterns may be a result of the altered signalling between the mesenchymal cells and neuronal growth cones and once formed antenatally persist postnatally [27,28] or these may be due to circulatory factors at the time of fusion of brachial plexus cords [29]. Random factors influencing the mechanism of formation of limb muscles and the peripheral nerves during the embryonic life may be accredited to the occurrence of communication. The human brachial plexus is known to appear as a single radicular cone in the upper limb bud which divides longitudinally into ventral and the dorsal segments. The ventral segments gives roots to the median and the ulnar nerves with musculocutaneous nerve arising from the median nerve. The possibility of failure of differentiation may be a cause for some of the fibres taking an aberrant course as communicating branch [30].
Phylogeny- Martin-Gruber anastomosis may be of phylogenetic importance as it is seen in many mammals including primates which show similar connections between median nerve and ulnar nerve [31]. Studies have shown a high incidence of Martin-Gruber anastomosis in apes [32] & monkeys [33,34].
Genetic Inheritance- Srinivasan & Rhodes examined congenitally abnormal embryos with trisomy 21 and found Martin-Gruber anastomosis in all of them in both the forearms [26]. So they linked it with trisomy 21. Also Crutchfield & Gutmann found Martin-Gruber anastomosis in 62% of family members of five propositi of the patients who had shown this anomalous connections & suggested that it is hereditory, probably autosomal dominant [13,35].
Clinical Implications- A positive aspect of Martin-Gruber anastomosis is that it can provide another motor and sensory innervation during a defect in these nerves after a trauma [36]. On the other hand these may also result in misdiagnosis during the assessment of nerve injuries [37], carpal tunnel syndrome [38], cubital tunnel syndrome [39] and leprosy neuropathy [40]. In such cases, identification of Martin-Gruber anastomosis becomes very crucial because it not only generates exacerbated or attenuated clinical symptoms, different from the usual ones [22] but also mode of treatment differs accordingly. However, nerve conduction study remains a reliable tool for its diagnosis [41].
Conclusion
To conclude, in North Indian population, the Martin-Gruber anastomosis is encountered in 11.6% limbs with no statistically significant difference between right and left sides. This variation is equated phylogenetically with apes and monkeys. A genetic inheritance with autosomal dominance is also suggested.
[1]. Kerr AT, The Brachial plexus of nerves in man, the variations in its formation and branchesAm J Anat 1918 23(2):285-395. [Google Scholar]
[2]. Hollinshed WH, General survey of the upper limbIn: Anatomy of surgeons. The back and limbs 1958 3New YorkPaul B. Hoeber Inc. Med Book Deptt of Harper and Brothers:225-228. [Google Scholar]
[3]. Dogan NU, Uysal I, Seker M, The communications between the ulnar and median nerves in upper limbNeuroanat 2009 8:15-19. [Google Scholar]
[4]. Martin R, Tal om Nervus allmanna Egenskaperi Mannisikans kropp 1763 StockholmLars Salvius (cited by Gruber) [Google Scholar]
[5]. Gruber Über die Verbindung des Nervus medianus mit dem Nervus ulnaris am Untearm des Menschen und der SäugetiereArch Anat Physiol 1870 37:501-22. [Google Scholar]
[6]. Erdem HR, Ergun S, Erturk C, Ozol S, Electrophysiological evaluation of the incidence of Martin-Gruber anastomosis in healthy subjectsYonsei Med J 2002 43:291-95. [Google Scholar]
[7]. Nakashima T, An anatomic study on the Martin-Gruber anastomosisSurg Radiol Anat 1993 15:193-95. [Google Scholar]
[8]. Taams KO, Martin-Gruber connections in South Africa: An anatomical studyJ Hand Surg 1997 22B:328-30. [Google Scholar]
[9]. Kawashima T, Sato K, Sasaki H, Stratification of the flexor retinaculum and the course and distribution of the ulnar, median and palmar digital nerves: an anatomical studyClin Anat 2004 17:643-50. [Google Scholar]
[10]. Shu H, Chantelot C, Oberlin C, Alnot JY, Shao H, Martin-Gruber communicating branch: Anatomical and histological studySurg Radio Anat 1999 21:115-18. [Google Scholar]
[11]. Rodriguez-Niedenfuhr M, Vazquez T, Parkin I, Logan B, Sanudo JR, Martin-Gruber anastomosis revisitedClin Anat 2002 15:129-34. [Google Scholar]
[12]. Sarikcioglu L, Sinde LM, Ozkaynak S, Aydin H, Median and ulnar nerve communication in the forearm:an anatomical and electrophysiological studyMed Sci Monit 2003 9:351-58. [Google Scholar]
[13]. Crutchfield CA, Gutmann L, Hereditary aspects of median ulnar nerve communicationsJ Neurol Neurosurg Psychiatry 1980 43:53-55. [Google Scholar]
[14]. Lee KS, Oh CS, Chung IH, Sunwoo IN, An anatomic study of the Martin-Gruber anastomosis: electrodiagnostic implicationsMuscle Nerve 2005 31:95-97. [Google Scholar]
[15]. Tagil SM, Bozkurt MC, Ozcakar L, Ersoy M, Tekdemir I, Elhan A, Superficial palmar communications between the ulnar and median nerves in Turkish cadaversClin Anat 2007 20:795-98. [Google Scholar]
[16]. Gumusburun E, Adiguzel E, A variation of the brachial plexus characterized by the absence of musculocutaneous nerveSurg Radio Anat 2000 22(1):63-65. [Google Scholar]
[17]. Sonck WA, Francx MM, Engels MM, Innervation anomalies in upper and lower extremities: potential clinical implications, how to identify with electrophysiologic techniquesElectromyogr Clin Neurophysiol 1991 31:67-68. [Google Scholar]
[18]. Sunderland S, The median nerve: Anatomical and physiological featuresIn: Nerves and Nerves Injury 1978 2nd EditionEdinburg, LondonChurchill Livingstone:672-727. [Google Scholar]
[19]. Romanes GJ, The pectoral region and axilla, the arm and the forearm and handIn: Cunninghams Manual of practical Anatomy 1986 Vol.115th Edition(1)Edinburgh, LondonThe English Language Book Society and Oxford University Press:28-89. [Google Scholar]
[20]. Kayamori R, Electrodiagnosis in Martin-Gruber anastomosisJ Jpn Ortho Assoc 1987 861:1367-72. [Google Scholar]
[21]. Prates LC, Carvalho VCD, Prates JC, Langone F, Esquisatto MAM, The Martin-Gruber anastomosis in Brazilians-An anatomic studyBraz J Morphol Sci 2003 20(3):177-80. [Google Scholar]
[22]. Felippe MM, Telles FL, Soares ACL, Felippe FM, Anastomosis between median nerve and ulnar nerve in the forearmJ Morphol Sci 2012 29(1):23-26. [Google Scholar]
[23]. Neidenfuhr MR, Vazquez T, Ferreira B, Parkin I, Nearn L, Sanudo JR, Intramuscular Martin-Gruber anastomosisClin Anat 2002 15:135-38. [Google Scholar]
[24]. Thomson A, Third annual report of the committee of collective investigations of the anatomical society of great Britain and Ireland for the year 1891-1892J Anat 1893 27:183-94. [Google Scholar]
[25]. Hirasawa K, Undersuchungen uber das perphere Nervenssystem, Plexus brachialis and die Nerven der oberen extremitatArb Anat Inst Kaiserlichen Univ Kyoto 1931 A2:135-36. [Google Scholar]
[26]. Srinivasan R, Rhodes J, The median ulnar anastomosis in normal and congenitally abnormal fetusesArch Neurol 1981 38:418-19. [Google Scholar]
[27]. Abhaya A, Khanna J, Prakash R, Variation of the lateral cord of brachial plexus piercing coracobrachialis muscleJ Anat Soc Ind 2003 52(2):168-70. [Google Scholar]
[28]. Sannes HD, Reh TA, Harris WA, Axon growth and guidanceIn:Development of nervous system 2000 9th EditionNew YorkAcademic Press:189-97. [Google Scholar]
[29]. Kosugi K, Mortia T, Yamashita H, Branching pattern of musculocutaneous nerve-Cases possessing normal biceps brachiiJikeakai Med J 1986 33:63-71. [Google Scholar]
[30]. Iwata H, Studies on the development of the brachial plexus in Japnese embryoRep Dept Anat Mie Perfect Univ Sch Med 1960 13:129-44. [Google Scholar]
[31]. Leibovic SJ, Hastings H, Martin-Gruber revisitedJ Hand Surg 1992 17:47-53. [Google Scholar]
[32]. Hepburn D, Comparitive anatomy of the muscles and nerves of the superior and inferior extremities of the anthropoid apesJ Anat Physiol 1892 26:149-356. [Google Scholar]
[33]. Sperino G, Anatomia Del chimpanzeeTorino:U.T.E.T. 1888 [Google Scholar]
[34]. Mannerfelt L, Studies on the hand in ulnar nerve paralysis: a clinical experimental investigation in normal and anomalous innervationsActa Orthopaedica Scandinavica 1966 87(2):19-29. [Google Scholar]
[35]. Piza-Katzer H, Familial occurrence of Martin-Gruber anastomosisHandchirurgie 1976 8:215-18. [Google Scholar]
[36]. Aktan ZA, Oztork L, Bilge O, Ozer MA, Pinar YA, A cadaveric study of the anatomic variations of the brachial plexus nerves in the axillary region and armTurk J Med Sci 2001 31:147-50. [Google Scholar]
[37]. Van Tieghan J, Vandendriessche G, Vanhecke J, Martin-Gruber anastomosis: the explanation for late diagnosis of severe ulnar nerve lesions at the elbowElectromyogr Clin Neurophysiol 1987 27:13-18. [Google Scholar]
[38]. Gutmann L, Median-ulnar nerve communications and carpal tunnel syndromeJ Neurol Neurosurg Psychiatry 1977 40:982-86. [Google Scholar]
[39]. Uchida Y, Sugiota Y, Electrodiagnosis of Martin-Gruber anastomosisJ Hand Surg 1992 17:47-53. [Google Scholar]
[40]. Brandsma JW, Birke JA, Sims DS, The Martin-Gruber innervated handJ Hand Surg 1986 11A:536-39. [Google Scholar]
[41]. Azhagiri R, Rajendran S, Martin-Gruber Anastomosis-Its morphology and clinical significanceInternat J of Anatom Sci 2012 3(1):19-21. [Google Scholar]