Intermittent claudication due to peripheral arterial disease occurs in 3 to 6% of elderly population [1,2]. Clinical evaluation followed by Doppler ultrasound and CT angiogram gives the definitive diagnosis. After the advancement of CT techniques, it is possible to cover entire limbs within a few seconds. Optimization of intravenous contrast with blood flow and CT scanning gives higher spatial resolution and coverage of more than 120cm [2]. Computers with graphics project images in 3D, volume rendered images and curved planar images. Imaging of the entire arterial system is possible using CT angiography and has found excellent concordance with digital subtraction imaging [3]. As there is need of accurate, reliable and reproducible non-invasive evaluation, segmental comparison of peripheral arterial system by Doppler ultrasound (USG) and CT Angiography (CTA) is done.
Materials and Methods
Fifty patients (median age-47.5 years, min-3, max-80; F: M=20:80) were evaluated using duplex Doppler and CT angiography for peripheral arterial system. Each arterial segment was analysed with both modalities. This study was a prospective study involving symptomatic patients of peripheral arterial disease. The study was approved by the academic and ethical committee of the institution. Subjects included were willing to undergo the protocol design after written consent. Patients who are allergic, pregnant, refused the protocol and did not give consent were excluded. After taking a brief history, Doppler USG and CTA were scheduled and instructions were given. CTA was performed after Doppler USG in all patients. The study duration of investigations for each patient was not more than 2 days.
There were 14 patients with upper limb complaints (15 upper limbs) and 36 patients with lower limb complaints (72 lower limbs). One patient had unilateral above knee amputation and two had unilateral below knee amputation.
Duplex DOPPLER evaluation is done using TOSHIBA NEMIO XG ultrasound system (Toshiba Medical Systems). Patients made to lie on USG couch in supine position for evaluation of iliac, femoral, tibial and dorsalis pedis arteries and popliteal artery was evaluated in prone position. Upper limbs were evaluated in supine position. Patients suspected of compression at the thoracic outlet evaluated in different provocative positions (hyperabduction, extension and deep inspiration). Using linear (6-12MHz) transducer, peripheral arteries evaluated in longitudinal and axial sections in B mode, colour flow, power and pulse wave modes in proximal to distal parts. Curvilinear (3-9MHz) transducers were used for iliac arteries. Pulse repetition frequency (PRF) was set optimally to detect best velocity and colour flow.
Normal appearance of arteries was inferred when the lumen appeared clear with thin uniform walls. Areas of soft or calcified atheroma can be seen within vessel lumen. Abnormal dilatations, thrombus and luminal narrowing appreciated from B mode images. The colour image demonstrated pulsatile flow of alternating red and blue colours. Reduced pulsatility indicates diseased proximal segment or low resistant distal segments. Severe stenoses produce a disturbed colour flow pattern beyond the site of lesion. Areas of colour flow disturbance were investigated with spectral Doppler to estimate the haemodynamic alterations. Luminal area compared with normal looking adjacent artery [Table/Fig-1].
Grading of stenosis by Doppler USG and CT Angiography.
| GRADE | CRITERIA |
|---|
| 1 | Normal patency |
| 2 | Mild (≤50% diameter) stenosis |
| 3 | Moderate (≥50 to 70% diameter) stenosis |
| 4 | Severe(≥70% diameter) stenosis |
| 5 | Occlusion |
CT angiography was performed using 64 Slice CT Scanner (SOMATOM Sensation 64; Siemens, Germany). All patients were made to lie in supine position. Patients with lower limb complaints were placed supine, in feet first position. Anatomical position of one upper limb or provocative position of thoracic outlet compression was preferred for upper limbs.
A scout image (tube voltage, 120 kV; tube current, 50 mAs) was followed by plan to include infrarenal aorta in lower limbs and arch of aorta in upper limbs. The mean coverage was 1140mm (range: 1032–1245mm). 70 to 100 ml (mean 80ml) of nonionic iodinated contrast medium (Omnipaque 370mg iodine per mL) administered using 18 or 20G venous catheter, placed in antecubital fossa. The amount of contrast decided to establish bolus duration that was equivalent to scanning time. The contrast administered using automated injector at 4 mL/sec flow rate and followed by 30-mL saline flush. Using bolus tracking technique, a region of interest was set in aorta. Repetitive low-dose monitoring (120 kV, 10 mAs with one second interscan delay) performed two seconds after contrast injection. After reaching contrast threshold of 120 HU, scanning (120 kV and 250mA adults; 150 mA for children) initiated automatically. Data acquisition performed in craniocaudal direction with slice thickness of 0.75mm, table feed of 18mm per rotation and 0.33s gantry rotation time.
Axial sections were reconstructed with a thickness of 1mm and no interslice gap, which resulted in mean of 1500 (range 1400-1700) axial images. The mean total scan time, which was defined as the time from patient entry into the CT suite until scanning was finished, was 6 minutes. No specific complications or technical difficulty encountered. All CTA images transferred to a workstation for 3D reconstructions, maximum intensity (MIP) and volume renderings (VRT) images. Axial and reconstructed images were analysed and graded [Table/Fig-1].
Results
A total of 645 arterial segments were studied in CT angiography and 619 arterial segments studied in Doppler USG. Out of the total (23 iliac and 3 subclavian arteries~4%) arterial segments could not be assessed due to bowel gas and bone interference. So, 619 segments were identified on both Doppler and CTA. In CTA, 226 diseased segments (36.51%) were identified (24 with moderate stenosis, 22 with focal severe stenosis, 56 with diffuse severe stenosis, and 124 with occlusion). Doppler USG overestimated the degree of stenosis by one grade in 47 segments (25 of which were considered normal at CT angiography but were diagnosed as mildly stenosed at Doppler USG), by two grades in 11 segments, by three grades in 30 segments and by four grades in 22 segments. The degree of stenosis was underestimated by one grade in 28 segments, by two grades in 9 segments, by three grades in 5 segments and by four grades in 3 segments [Table/Fig-2].
Cross tabulation of stenosis grade in Doppler and CT Angiography.
| CT ANGIOGRAPHY |
|---|
| DOPPLERUSG | Grade | 1 | 2 | 3 | 4 | 5 | Total |
| 1 | 324 | 4 | 4 | 4 | 3 | 339 |
| 2 | 25 | 4 | 4 | 0 | 1 | 34 |
| 3 | 1 | 0 | 7 | 8 | 5 | 21 |
| 4 | 21 | 7 | 4 | 24 | 12 | 68 |
| 5 | 22 | 9 | 3 | 20 | 103 | 157 |
| Total | 393 | 24 | 22 | 56 | 124 | 619 |
A statistically significant difference (p <0 .05) between Doppler USG and CTA found in all grades of stenosis (p<0.05). The sensitivity, specificity, and accuracy of Doppler USG compared with CTA was 93.36%, 82.44%, and 86.42%, respectively. Agreement was 74.64%.
Considering iliac segments [Table/Fig-3] as a separate group, the sensitivity, specificity and accuracy of Doppler USG were 96.55%, 94.79% and 95.2%. In femoro popliteal segments (common, superficial femoral, and popliteal arteries), the sensitivity, specificity and accuracy of Doppler USG were 88.88%, 92.95% and 91.58%. In the distal arterial segment (tibial and dorsalis pedis arteries), sensitivity, specificity and accuracy were 96.15%, 61.53%, and 78.84%. For the upper limb arteries overall sensitivity, specificity and accuracy were 90.47%, 72.54%, and 77.77%.
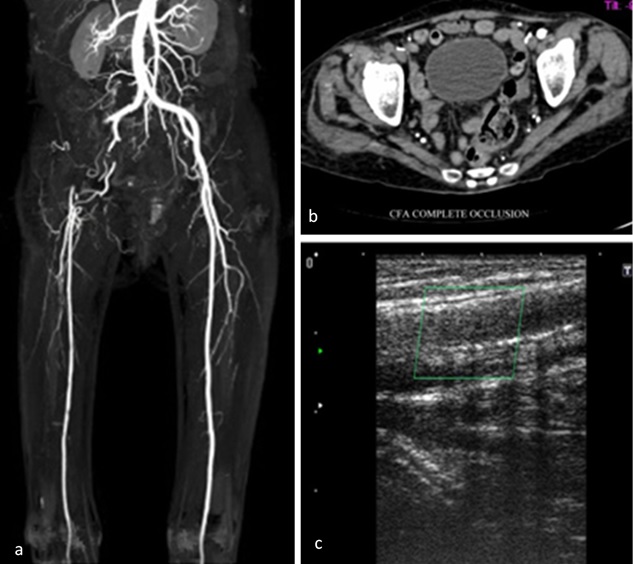
Short segmental complete occlusion of right external iliac and common femoral arteries: (a) Coronal MIP image; (b) axial section at external iliac artery level; and (c) corresponding longitudinal section of right common femoral artery.
Comparisons with previous studies show nearly similar sensitivity of CTA and DSA and lower specificity of Doppler USG with CTA. Findings are tabulated in [Table/Fig-4].
Comparison with previous studies.
| Sensitivity % | Specificity % | Accuracy % | Agreement | Study | Done by |
|---|
| Doppler vs DSA | 86(74-91) | 97(94-99) | NA | | meta analysis | Koelemay et al., [4] |
| 98 | 81 | | k=0.81 | PSV considered | Sensier et al., [5] |
| NA | NA | | k=0.81 | CFI considered | McCarthy et al., [6] |
| CTA vs DSA | 96 | 97 | NA | | n=39, 16 MDCT | Jurgen K et al., [7] |
| 96 | 93 | 94 | NA | n=50,4 MDCT | Carlo Catalano et al., [8] |
| 92 | 93 | NA | NA | Meta analysis | Majanka H. Heijenbrok-Kal et al., [9] |
| NA | NA | NA | 78% | n=35, ?MDCT | B Tins et al., [10] |
| NA | NA | 88-96% | NA | n=17, 16 MDCT | Thomas Schertler et al., [11] |
| Doppler vs CTA | 93 | 82 | 86 | 75% | n=50, 64 MDCT | Our Study |
NA- not available; k-kappa; MDCT –multi detector computed tomography; CTA- CT angiography, DSA-Digital Subtraction Angiography.PSV-Peak systolic velocity, CFI-Colour flow imaging, ?-not known.
There was good agreement between Doppler USG and CTA of upper limbs arteries and proximal outflow arteries of the lower limb. Doppler overestimated stenosis grade predominantly in distal runoff arteries of lower limbs. Doppler USG and CTA findings showed good correlation (74%) in most of the vessels with excellent sensitivity (93%), negative predictive value (95%), specificity (82%) and accuracy (85%). However, Doppler overestimated the grade of stenosis in a significant percentage (18%).
There were 6 patients of traumatic arterial injury (2 upper limbs, 8 lower limbs) having 74 arterial segments. The sensitivity, specificity, and accuracy of Doppler USG compared with CTA were 81.81%, 85.71%, and 85.13%. There was 77.02% (57 of 74 segments) agreement. Doppler USG and CTA evaluation of traumatic arterial injury showed no difference with peripheral arterial disease. 9 arterial grafts (8 occluded, 1 patent) and 2 post traumatic pseudo aneurysms from popliteal artery were correctly identified with both Doppler USG and CT angiography [Table/Fig-5,6 and 7].
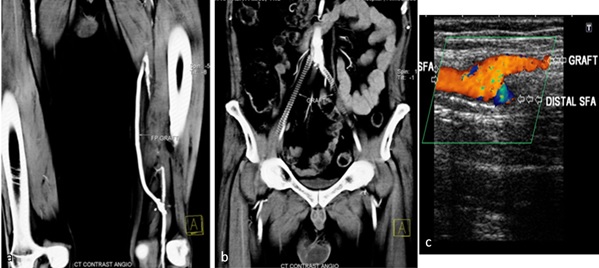
(a&b) Coronal reformatted MIP images showing completely occluded bi iliac graft and functional femero popliteal graft; (c) Spot image of colour Doppler showing left superficial femoral artery patent graft and completely occluded native superficial femoral artery.
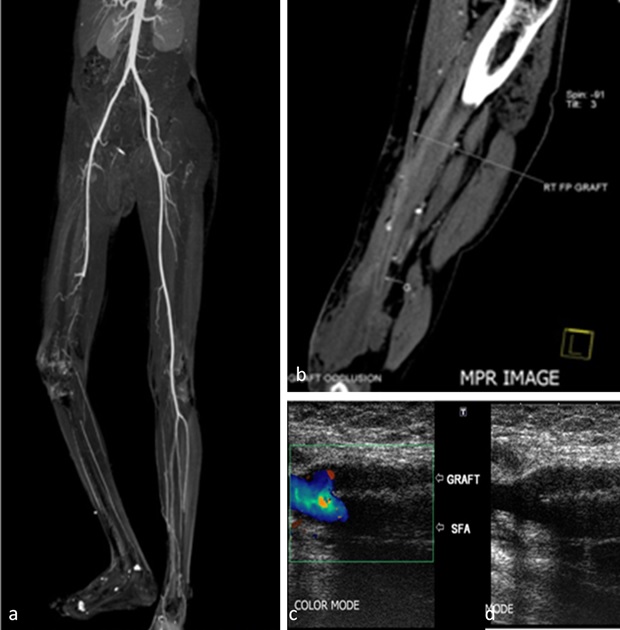
(a&b) Coronal thick MIP image of bilateral lower limbs showing complete occlusion of right distal femoral artery with reformed tibial arteries; (c&d) Selected colour Doppler spot images of right superficial femoral artery showing occluded native vessel and right femoro popliteal graft.
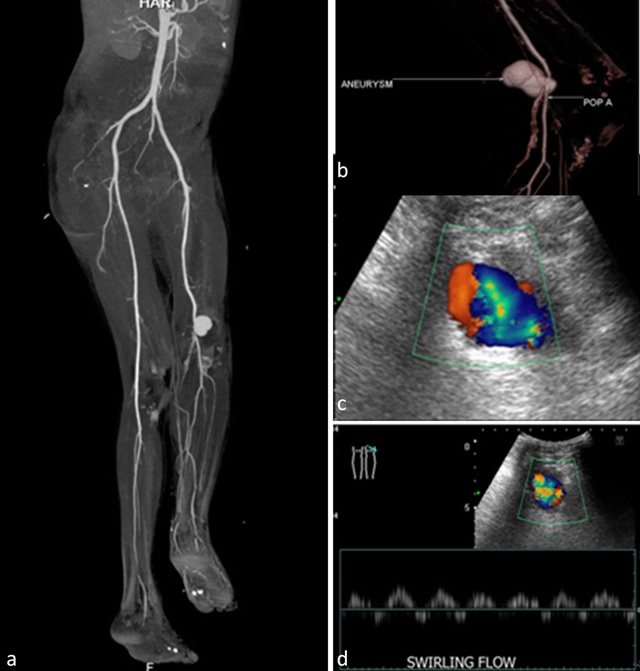
(a&b) Coronal MIP CT angiogram image showing left popliteal artery pseudo aneurysm; corresponding colour Doppler; (c) and pulse wave imaging; (d) depicting aneurysm and swirling flow.
Discussion
Peripheral arterial disease is an important cause of morbidity among elderly males [12]. Other than vascular claudication, several conditions simulate intermittent claudication; hence as preliminary examination, Doppler USG and angiography is indicated for defining anatomy and assessing vascular narrowing [13].
Catheter-based DSA is the reference standard for evaluation of limb ischemia. Spiral CT demonstrating vascular diseases have been well documented since early 1990s. CTA has replaced catheter-based angiography for clinical assessment of the aorta and its branches [3,14,15]. Doppler USG has many advantages, like no radiation, repeatability, functional evaluation of blood flow, velocity quantification and direct measurement of thrombus, dilatation or narrowing. Use of Doppler USG is limited by a small window, wide interobserver variability, limited reproducibility and long examination time. CTA using single shot intravenous injection of non ionic contrast medium reproduces entire arterial anatomy within 2-3 minutes. Interpretation of axial, multiplanar reconstructed images, maximum intensity projection and volume rendered technique requires approximately 10-15 min. Depiction of arterial reformation and collaterals are better with CTA, however limited to ascertain the direction of flow. Radiation, compromised renal function and repeatability also limit its use. In our study, no patients required repeat CT angiography. Arterial narrowing was graded using axial images in CTA and B mode images in Doppler USG.
About 4% (23 iliac and 3 subclavian) arterial segments vessels could not be evaluated by Doppler, due to bowel gas and bones. Thus, Doppler USG can be valuable in the evaluation of infra inguinal region of lower limbs and from 2nd part of the subclavian artery in upper limbs.
Stenosis of peripheral arteries were graded in Doppler USG using peak systolic velocity (PSV) as per Sensier et al., or anatomical imaging from colour flow or power mode as per McCarthy et al., [6,16]. Imaging appearances of vascular tree appear similar to angiography in power mode, and closely reflects similar imaging appearance with CT angiography MIP images. Focused ultrasound gives valuable information regarding the vessel wall in atherosclerotic arterial disease in addition to evaluation of vascular lumen causing stenosis, thrombus, etc. However, dense calcification hinders evaluation of lumen due to acoustic shadowing. Spectral examination was used for correlation of findings in colour flow and power modes. Calcification of vessel wall obscuring lumen evaluation was seen mainly in distal tibial vessels.
Amount of contrast used varies from 20 mL (for a child of 3 y) to 100 mL (for a patient with cardiac disease with low ejection fraction) with mean 70 mL was used. Study covered from xiphisternum to tip of toe in cranial caudal direction; followed by 5 second delayed scan covering below knee portion in caudal cranial direction to assess low flow in distal runoff vessels. In many circumstances, delayed contrast filling of runoff vessels avoided erroneous diagnosis of occlusion. Demographic analysis showed most of the patients were within 45-65 year of age (mean 45.6 y) compared to previous studies by Jürgen K. Willmann et al., (66 y) and Carlo Catalano et al., (67 y) [7,8]. Males had significant association in lower limb vascular disease (external iliac artery p=0.01, common iliac artery p=0.007, superficial femoral artery p=0.021) and females had significant association in upper limb vascular disease (Brachial artery p=0.046, Radial artery p=0.035). Smoking and diabetes showed significant association in diseases of the common femoral artery (p=0.003).
Results from correlation showed Doppler over estimates stenosis in distal tibial vessels. This is possibly due to difficulty to detect tandem lesions in multi segmental occlusive arterial disease or proximal lesions causing reduced flow in distal vessels interpreted as severe narrowing by duplex Doppler examination. A statistically significant difference (p <0 .05) between Doppler USG and CTA was found in all grades of stenosis, so, one investigation is better than the other. Overall, the sensitivity, specificity, and accuracy of Doppler USG compared with CTA were 93.36%, 82.44%, and 86.42%, and agreement was 74.64%. Considering region wise, excellent sensitivity observed in all regions (91-97%), and wide variation in specificity (61-94%) and poor specificity seen in distal runoff arteries of lower limbs (61%) and upper limbs (73%) [Table/Fig-8,9]. Considering excellent sensitivity (93%), good specificity (82%) and 95.5% negative predictive value. Doppler USG can be the first investigation in excluding disease of the peripheral arterial system. Patients with haemangioma, arterial grafts, thrombus and aneurysm [Table/Fig-7] are correctly identified by both modalities. However, further studies required for evaluation of specific diseases. In our experience, assessing luminal narrowing in densely calcified arteries especially chronic diabetics and hypertension is difficult. Patent lumen can be inferred when distal luminal contrast of similar density with no significant collaterals. Subtraction method using plain and contrast sequences were helpful. However, the technique is limited by movement artifacts.
Under and over estimation of stenosis grade, segmental comparison of Doppler and CTA. (DOP-Doppler, CTA- CT angiography, SCA - subclavican, AXA- Axillary, BRA-Brachial, RAA- Radial, ULA- Ulnar, CIA-Common iliac, EIA - External iliac, CFA-Common femoral, SFA-Superficial femoral, POA- Popliteal, ATA-Anterior tibial, PTA- Posterior tibial, DPA- Dorsalis pedis arteries).
Note:-0finding agreed-5,-4,-3,-2,-1-numbers of grades of undergrading.+1,+2,+3,+4,+5-number of grades of over estimation.
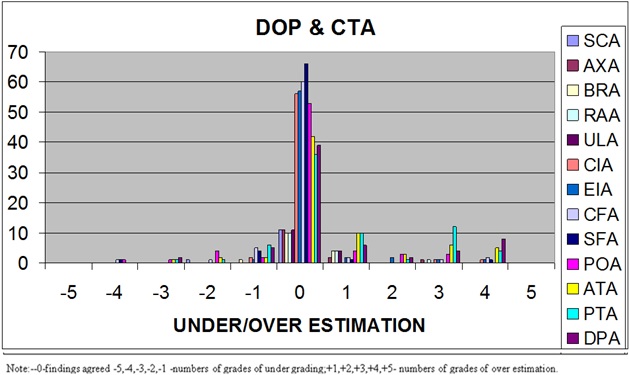
Under and over estimation of stenosis grade, comparing Doppler and CT angiography.
| On Doppler | UNDER ESTIMATION | | OVER ESTIMATION |
|---|
| S.NO | ARTERY | -5 | -4 | -3 | -2 | -1 | 0 | + 1 | + 2 | + 3 | + 4 | + 5 |
| 1 | SCA | 0 | 0 | 0 | 1 | 0 | 11 | 0 | 0 | 0 | 0 | 0 |
| 2 | AXA | 0 | 0 | 0 | 0 | 0 | 11 | 2 | 0 | 1 | 0 | 0 |
| 3 | BRA | 0 | 0 | 0 | 0 | 1 | 10 | 4 | 0 | 0 | 0 | 0 |
| 4 | RAA | 0 | 0 | 0 | 0 | 0 | 10 | 4 | 0 | 1 | 0 | 0 |
| 5 | ULA | 0 | 0 | 0 | 0 | 0 | 11 | 4 | 0 | 0 | 0 | 0 |
| 6 | CIA | 0 | 0 | 0 | 0 | 2 | 56 | 0 | 0 | 1 | 1 | 0 |
| 7 | EIA | 0 | 0 | 0 | 0 | 1 | 57 | 2 | 2 | 1 | 1 | 0 |
| 8 | CFA | 0 | 1 | 0 | 1 | 5 | 60 | 2 | 0 | 1 | 2 | 0 |
| 9 | SFA | 0 | 1 | 0 | 0 | 4 | 66 | 2 | 0 | 0 | 1 | 0 |
| 10 | POA | 0 | 1 | 1 | 4 | 2 | 53 | 4 | 3 | 3 | 0 | 0 |
| 11 | ATA | 0 | 0 | 1 | 2 | 2 | 42 | 11 | 3 | 6 | 5 | 0 |
| 12 | PTA | 0 | 0 | 1 | 1 | 6 | 36 | 10 | 1 | 12 | 4 | 0 |
| 13 | DPA | 0 | 0 | 2 | 0 | 5 | 39 | 6 | 2 | 4 | 8 | 0 |
| TOTAL | 0 | 3 | 5 | 9 | 28 | 462 | 51 | 11 | 30 | 22 | 0 |
Most of the patients with good distal flow in CTA were managed conservatively (36%). Vascular occlusions of large outflow artery were treated with grafting (18%). Diseases of distal vessels involving tibial arteries are managed with amputation (10%) depending upon the clinical condition.
Conclusion
Doppler USG is valuable in the evaluation of infra inguinal region of lower limbs and from 2nd part of the subclavian artery in upper limbs. As there is significant statistical difference between Doppler USG and CTA, suggests one method is better than the other. Doppler USG can be used as the first investigation of peripheral arterial diseases. In multi segmental and distal arterial disease, Doppler USG overestimates the stenosis. Hence CTA has to be preferred.
NA- not available; k-kappa; MDCT –multi detector computed tomography; CTA- CT angiography, DSA-Digital Subtraction Angiography.PSV-Peak systolic velocity, CFI-Colour flow imaging, ?-not known.