Acute Myoclonic Jerk Terminated by A Simple Procedure – A Case Report
Manigandan Gopi1, Aashish Arumugam2
1 Assistant Professor, Department of General Medicine, Mahatma Gandhi Medical College and Research Institute, Pondicherry, India.
2 Assistant Professor, Department of General Medicine, Melmaruvathur Adhiparasakthi Institute of Medical Sciences and Research, Melmaruvathur, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manigandan Gopi, 33 B, Thesai Street, Walajapet-632513, Tamilnadu, India.
E-mail: lyfdiver@gmail.com
Myoclonic jerks are brief involuntary twitching of a muscle or a group of muscles. It is a medical sign and not a diagnosis of a disease. It occurs in number of secondary conditions like hepatic failure, renal failure, dyselectrolytaemia, etc in addition to the physiologic, epileptic, essential and psychogenic causes. Myoclonic jerks secondary to uraemia usually occur in the end stage renal failure and is resolved by renal replacement therapy. Here we report a case of uremic myoclonic jerk presented to our emergency department which occurred secondary to obstructive uropathy secondary to neurogenic bladder caused by old traumatic paraparesis and it was resolved by simple and timely intervention by bladder catheterization and it prevented the patient from going into uremic encephalopathy.
Obstructive uropathy, Neurogenic bladder, Uraemia
Case Report
A 60-year-old male came with complaints of muscle twitches on the face since one day prior to the day of admission. He also had nausea and vomiting for two days prior to this onset of muscle twitches. Patient also gave history of trauma in the past before one year which was described as a fall from a 10 feet height building accidentally, followed by girdle pain around the umbilicus and disability to use his both the lower limbs and became bedridden. He developed urinary incontinency associated with disturbance in bowel control for the past three months prior to which it was normal and controlled. The urinary incontinency was described by patient as increased frequency and precipitancy of micturition and feeling of an incomplete evacuation of bladder with residual urine whenever he micturates.
At the time of presentation his clinical examination showed exaggerated knee and ankle jerks with bilateral positive babinski sign suggestive of pyramidal tract involvement. Among the superficial reflexes patient had normal upper abdominal reflex with loss of lower abdominal reflex, positive beevors sign with intact cremasteric reflex. Patient also had loss of touch, pain and temperature sensation below the umbilicus. The positive beevors sign, girdle pain at the level of umbilicus, absence of lower abdominal reflexes and exaggerated knee and ankle jerk wit bilateral positive babinski sign localized the lesion as a compressive myelopathy at the level of below T10 (due to presence of upper abdominal reflex) and above L1 (intact cremasteric reflex).
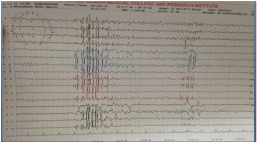
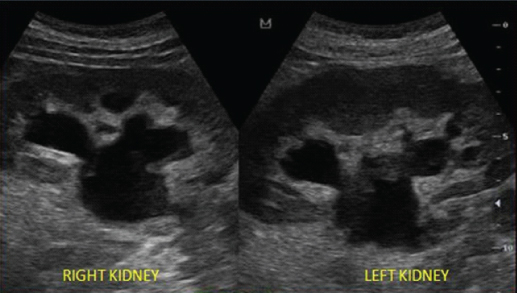
Patient had elevated renal parameters (Blood Urea-210 and Serum Creatinine-6) with elevated total count of 20,500 (neutrophils-94%, Lymphocytes-6%) with elevated ESR(1/2 h -52 mm, 1h -106 mm) and urine routine showed plenty of pus cells with bacteria 2+. Emergency EEG of the Brain showed Brief bursts of high potential spikes and polyspikes from both the cerebral hemispheres for each muscle twitch appeared and it was suggestive of cortical myoclonus [Table/Fig-1]. Emergency USG abdomen showed bilateral dilated renal calyces with pelvis and bilateral ureters with normal prostate and no calculus with renal Cortical thinning suggestive of bilateral hydroureteronephrosis secondary to Obstructive Uropathy due to bladder outlet obstruction [Table/Fig-2].
EEG picture showing brief bursts of high potential spikes and poly spikes from both cerebral hemispheres suggestive of cortical myoclonus.
USG picture showing dilated renal calyces with dilated renal pelvis and proximal ureter in both the kidneys.
The problem list of patient includes-
1. Compressive myelopathy with loss of bowel and bladder control.
2. Obstructive uropathy with elevated renal parameters.
3. Cortical myoclonic jerks.
Here the cortical myoclonic jerk is attributed to metabolic cause (uraemia) caused by bladder outlet obstruction secondary to neurogenic bladder caused by compressive myelopathy. Patient was catheterized immediately with Foleys catheter and drained about 400 ml of frank pus [Table/Fig-3] followed by 600 ml of urine. Patient myoclonic jerk disappeared slowly in next two hours. Patient was admitted and on adequate hydration and antibiotic coverage and his renal parameters came down to normal base line value and myoclonic jerks completely resolved after five days of hydration and antibiotic therapy. Review EEG was taken and was normal without any spikes. MRI spine showed compressive fracture of T11 vertebra [Table/Fig-4] causing myelopathy with retropulsive fragment causing compression of T11 & T12 roots. Urodynamic flow studies done by urologists and was found to have hyper reflexic bladder with sphincter dyssynergia and later discharged with clean intermittent catheterization and anticholinergics (oxybutinin) for neurogenic bladder as patient was not willing for surgery for cord compression. Patient was followed up after one month and subsequently then once in three months patient renal parameters were within normal limits and had no myoclonic jerks.
Picture showing 400 ml of frank pus in uroflowmeter and in urobag when patient was catheterized with Foleys.

MRI picture showing vertebral fracture at T 11 vertebra.

Discussion
Myoclonic jerks are a type of movement disorder which manifest as sudden brief shock like jerks [1]. Myoclonic jerks are not particular to a disease and it should be considered as a medical sign as it occurs in a number of medical conditions. Anatomically based on the site of origin its classified as cortical, subcortical, spinal and peripheral [2]. The face and the distal muscles of the upper limb occupy a major cortical representation and hence the cortical myoclonic jerks are commonly seen in those areas. Myoclonic jerk can be grouped as essential, physiological, secondary, epileptic, and psychogenic based on the aetiology [1]. In relation to muscle tone myoclonic jerks can be classified as positive myoclonus (brief burst of muscular activity) and negative myoclonus(brief cessation of ongoing muscular activity) [3]. In the above case anatomically it is a cortical myoclonus (based on EEG), aetiologically secondary myoclonus secondary to uraemia and a positive myoclonic jerk. Renal failure resulting in uraemia produces a number of neurologic complications involving central nervous system and peripheral nervous system starting from diffuse encephalopathy, seizures, stroke, sleep alterations, polyneuropathy, mononeuropathies, and myopathy in addition to uremic myoclonic jerks [4].
The pathophysiology of myoclonic jerks in renal failure [Video-1] is due to the accumulation of guanidino compound methyl guanidine along with the other organic compounds like urea and uric acid as a consequence of decreased elimination secondary to the injury to kidney [5]. The methyl guanidine causes excitation of the excitatory neurotransmitter(NMDA-N Methyl D Aspartate) and inhibition of the inhibitory tranmsmitter (GABA) in the central nervous system, there by resulting in myoclonic jerk [5]. Secondary hyperparathyroidism is also found to be involved indirectly in pathogenesis of uremic myoclonic jerk [5]. Asterixis, muscle cramps and tremor are seen in early stage of uremic encephalopathy while myoclonic jerks are manifested in the later stage of uremic encephalopathy [5]. But in our case myoclonic jerk appeared in the early stage without a usual uremic encephalopathy early stage symptoms like tremors and asterixis and it acted as an index sign to the development of uremic encephalopathy. The identification of the secondary cause of the myoclonic jerk as uraemia due to obstructive uropathy and intervention done in right time prevented the patient from entering in to uremic encephalopathy.
Conclusion
Myoclonic jerks are rare presentation to the emergency department, even then the encountering physicians should have a thorough knowledge of the causes as timely identification based on the clinical scenario and intervention as explained in this case report can avoid dreadful complications.
Declaration
This case had been presented as a paper in GAMET -2014 (Global Annual Meet on Emergency medicine and Trauma) conference held in Global hospitals Chennai, India.
[1]. Kojovic M, Cordivari C, Bhatia K, Myoclonic disorders: a practical approach for diagnosis and treatmentTher Adv Neurol Disord 2011 4(1):47-62. [Google Scholar]
[2]. Burn D, Oxford Textbook of Movement Disorders 2013 1 edUnited KingdomOxford University Press:375 [Google Scholar]
[3]. LeDoux MS, Movement Disorders: Genetics and Models 2005 1 edLondonAcademic Press:822 [Google Scholar]
[4]. Burn D, Bates D, Neurology and the kidneyJ Neurol Neurosurg Psychiatry 1998 5(6):810-21. [Google Scholar]
[5]. Engel J, Pedley TA, Aicardi J, Epilepsy: A Comprehensive Textbook 2008 PhiladelphiaLippincott Williams & Wilkins:1036 [Google Scholar]