A bony septum separates the olecranon and coronoid fossae at the lower end of the humerus, between the two epicondyles. The thickness of the bony septum determines its opacity or translucency. A perforation present in this septum results in the formation of supratrochlear foramen (STF). It was first described by Mekel in 1825 [1]. STF has been designated by a variety of names such as intercondylar foramen, olecranon foramen and epitrochlear foramen [2,3]. Hrdlicka referred to it as the septal aperture [4]. The numerous terminologies used to denote the same structure speaks of the lack of understanding of its function and aetiology.
T-Box genes may play a role in STF formation. Genes of the TBX family control the synthesis of proteins known as T-box proteins that are crucial for the development of the limbs and the heart in utero [8]. This concept was furthered by Govonis work which postulated that T box genes effect postnatal development of the limbs [9]. It has been noted by Hirsh in 1972 that the septum is intact and lined by synovial membrane until the age of 7 years. Perforations if any occur only after such time [10]. Since the STF is not present in neonates, it is possible that these genes may play a role in its postnatal development. The STF was a hitherto unimportant descriptive feature of the humerus. Based on orthopaedic surgical experience, it has been noted that STF is associated with a narrow intramedullary cavity [11]. In the paediatric age group the supracondylar fracture is of common occurrence [12]. This is treated by intramedullary nailing which may be compromised by the presence of this aperture. The retrograde nailing is done through the medial and lateral epicondyles or only through the lateral [13]. Nerve injuries become pertinent. Therefore its presence is of utmost importance in planning nailing of fractures of the lower end of the humerus [11,12]. During radiological evaluations of the humerus, presence of STF may result in erroneous interpretation as pathological lesions or cysts [13]. Its incidence varies widely from 0.3 % to 58 % in different races [13–15].
This study aims to describe its prevalence and morphometry in relation to its shape and size and distance from the epicondyles.
Materials and Methods
A prospective study of 244 unpaired humerii, 130 left sided and 114 right sided of unknown age and sex from the bone collection of the Department of Anatomy, Amrita Institute of Medical Sciences, Kochi was conducted over a period of 6 months, between May and November, 2015. The presence of STF and its prevalence were studied. These results were compared to other population studies. Shapes were visualized and classified.
In the oval STF, transverse and vertical diameters were measured. The mean and standard deviation were calculated and compared with other recent studies. In the round STF, diameter was noted. In the triangular STF, the maximum vertical and transverse lengths were considered. In the reniform STF, vertical length at the hilar point and maximum transverse length was measured.
The distance from the nearest margin of the STF to the tip of medial, lateral epicondyles and the lower trochlear margin were measured with digital vernier calipers and averages were calculated. All measurements were tabulated in millimeters. Statistical analysis was done using IBM SPSS 20 version. The mean, standard deviation and p-value were calculated using student’s t-test.
The sieve foraminae were not measured. In specimens where perforation was distinctly absent, presence of translucent septa was sought by holding it against a lighted X-Ray lobby.
Results
Of the 244 humeri studied, 60 showed presence of the foramen, 45 were opaque and 139 showed translucent septa [Table/Fig-1]. The sidewise prevalence of opacity, translucent septum and foraminae were tabulated [Table/Fig-2]. The commonest shape noted was oval. Other shapes such as round, triangular, rectangular, sieve and reniform were visualised [Table/Fig-3].
Frequency of Supratrochlear foramen, Translucent septum and Opacity.
| Sl. No. | Types | Total | Percentage (%) |
|---|
| 1 | Opaque | 45 | 18.44 |
| 2 | Translucent septum | 139 | 56.96 |
| 3 | Foramen | 60 | 24.59 |
Side wise distribution of Supratrochlear foramen, Translucent septum and Opacity.
| Sl. No. | Types | Left sided | Percentage (%) | Right sided | Percentage(%) |
|---|
| 1 | Opaque | 20/45 | 44.44 | 25/45 | 55.55 |
| 2 | Translucent | 69/139 | 49.64 | 70/139 | 50.36 |
| 3 | Foramen | 41/60 | 68.33 | 19/60 | 31.67 |
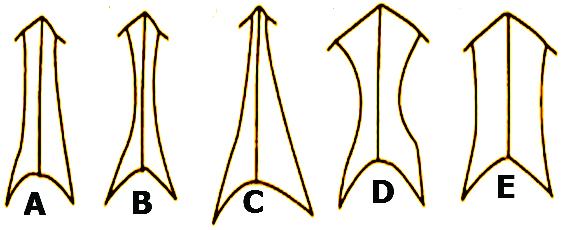
Different shapes of foraminae and their prevalence.
| Sl. No | Shapes | Right | Left | Total | Percentage (%) |
|---|
| 1 | Oval | 8 | 23 | 31 | 51.6 |
| 2 | Round | 5 | 8 | 13 | 21.6 |
| 3 | Reniform | 1 | 6 | 7 | 11.6 |
| 4 | Seive | 1 | 4 | 5 | 8.3 |
| 5 | Triangular | 2 | 1 | 3 | 5 |
| 6 | Rectangular | 1 | 0 | 1 | 1.6 |
In the oval STF [Table/Fig-4], the mean transverse and vertical diameters on the left was 4.9 and 3.27 mm and on the right it was 5.12 and 3.48 mm respectively. The mean diameter of the round foramen [Table/Fig-5] was 3.23 and 4.89 mm for left and right sides respectively. In the triangular type [Table/Fig-6], the mean transverse and vertical lengths were 4.6 and 3.92 mm respectively on the left and 5.58 and 4.30 mm respectively on the right. There was only one sample of the rectangular STF [Table/Fig-7] which was right sided. Its length was 4.1mm and the breadth was 2.27 mm. The reniform type [Table/Fig-8] totalled 7, of which 6 were on the left side. The average vertical length at the hilar point was 4.52 mm and the average transverse measurement was 7.44 mm on the left. The lone right sided reniform STF was smaller with a vertical length of 3.83mm and 6.2 transversely. The present study reports 8.3% sieve STF [Table/Fig-9], that is 5 out of the total 60 obtained. The foramina of the right side were found to be larger, regardless of shape. The mean values of the distance from the medial epicondyle, lateral epicondyle and trochlea to the STF margins were tabulated separately for right and left sides [Table/Fig-10,11]. Of the 244 humeri inspected in the present study, 139 (56.8%) showed translucency [Table/Fig-12]. The prevalence of translucent septum on the left and right side were 69 and 70 respectively.
Oval supratrochlear foramen.
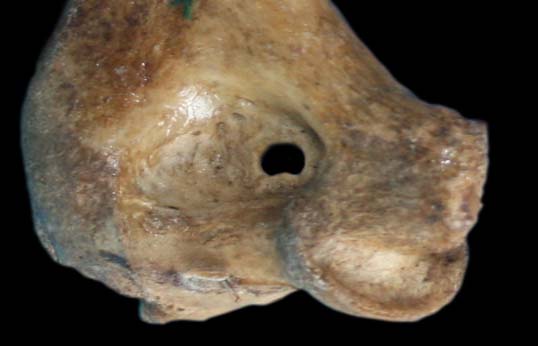
Round supratrochlear foramen.
Triangular supratrochlear foramen.

Rectangular supratrochlear foramen.

Reniform supratrochlear foramen.
Seive supratrochlear foramen.

Average distance of the foramen margin from key points in mm. (p>0.05, independent sample test / Student’s t-test is not significant).
| Point | Left | Right | p-value |
|---|
| Medial epicondyle | 24.39 + 3.15 | 24.91 + 2.93 | 0.559 |
| Lateral epicondyle | 26.92 + 2.46 | 27.2 + 2.95 | 0.705 |
| Lower trochlear margin | 14.41 + 1.62 | 14.29 + 1.58 | 0.787 |
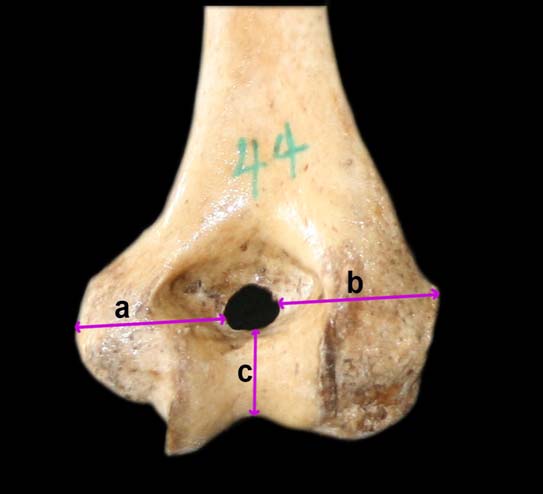
Diagram showing key points of measurements.
(a: tip of medial epicondyle to STF margin, b: tip of lateral epicondyle to STF margin, c: Lower margin of trochlea to STF margin)

Discussion
Foramina are defined as conduits for vessels and nerves, while apertures are merely openings in bones [16]. No anatomical structure is known to pass through the STF and hence does not qualify to be one by definition. Its aetiology and function are largely obscure. Two theories for the formation of this foramen have been proposed.
According to the mechanical theory, propounded by Glanville the foramen is formed as a result of articulations between the humerus and ulna during extremes of flexion and extension [16]. Its presence therefore can be attributed to the functional development of the elbow joint and its variable shapes to the morphometry of the articulating surfaces. Its left side frequency can be explained on the basis of handedness. It is more common on the non-dominant left hand as the dominant right limb has more robust bones [10,17]. The frequency of STF on left side has been reported by many workers [6,16,18,19]. Study done by Nayak et al., however showed a greater prevalence on the right side [12]. In the present study the frequency is more on the left side [Table/Fig-1].
The genetic theory states that STF is an inherited trait [13,20]. Frequencies of occurrence in different populations favour this theory. Studies in Greek population having revealed prevalence as low as 1% and the highest of 52 % have reported in Arkansas Indians [21]. Some of the other populations on which the STF has been studied include American 6.9%, Egyptians 7.9 % and Japanese 18.8% [2,6,22]. This wide variation favours the genetic basis of development. The studies done on Indian population have shown regional variations. The highest of 32 % was seen in Central Indian population [1] while South Indian population recorded 28% [ 7] and North Indians and East Indians were 27.4% and 27% respectively [18, 23]. In the present study of the 244 humeri study STF was observed in 60 of the 244 accounting for prevalence of 24.59 %.
Variability of shapes was also noted. Shapes such as round, oval, triangular, rectangular, reniform and sieve-like have been reported in literature [12,13,15,21,24].
In the present study the oval STF was the commonest type. Bhanu Diwan and Ergdomus reported the oval STF as the commonest variety [14,19,21]. The average transverse diameter of the STF was 4.61mm and 5.04mm, on left and right sides respectively while the vertical diameter was 3.26 mm and 3.68 mm on left and right sides respectively. The results obtained in the present study were compared with that of other authors like Nayak, Krishnamurthy and Veerappan [Table/Fig-13].
Comparative study of mean transverse (TD) and vertical diameters (VD) of oval foramen.
| Sl no. | Authors | Year | Diameters | Left | Right |
|---|
| 1 | Nayak et al., | 2009 | TD | 6.55 ± 2.47 | 5.99 ± 1.47 |
| VD | 4.85 ± 1.64 | 3.81 ± 0.97 |
| 2 | Krishnamurthy et al., | 2011 | TD | 6.5 ± 2.59 | 5.26 ± 2.47 |
| VD | 4.7 ± 1.69 | 4 ± 1.52 |
| 3 | Veerappan et al., | 2013 | TD | 7.53±1.28 | 8.30 ± 1.07 |
| VD | 5.35±1.60 | 4.09±1.13 |
| 4 | Present study | 2015 | TD | 4.88 ± 1.63 | 5.24 ± 1.76 |
| VD | 3.37 ± 1.25 | 3.82 ± 1.07 |
Three noteworthy conclusions were drawn from this comparison.
The dimensions estimated in the present study were smaller than the results obtained by other workers.
While comparing the size of the foramen of the two sides, we noted larger foraminae on the right side whereas all these authors noted the foramen to be larger on the left side. But in all studies the STF was horizontally oval.
The number of foramen reported was more on the left side in the present study as in other studies.
The higher left sided frequency obtained is in keeping with the theory of handedness and relation to robustness and gracility of bone. The larger sized foramen on the right side however points to greater mechanical effect in the production of the aperture in the more used limb.
It was the second most common pattern of STF. This finding is similar to that obtained by Nayak and Ndou [12,13]. In the present study, the frequency was more on the left side, this was as indicated by other authors. When comparing the relative size of two sides, the right foraminae were larger. Therefore the result of this study is inconsistent with the theory that formation of the STF is a result of functional development of the elbow joint. Most of the similar studies show higher values for transverse diameter on the left [11,23–25].
The triangular STF dimensions obtained in this study could not be compared as there was no mention of measurements in any literature review. To be noted is the larger right sided foramen obtained in this study.
The rectangular STF was noted in one case in the present study. The only other mention of rectangular STF was in the study done by Jing et al., who presented it as a new finding. Of the 262 unpaired humerii they studied they reported two instances [26].
In the present study the reniform type totalled 7, of which 6 were of the left side. In the study done by Sunday et al in 65 humeri, 18 STF were recorded in total of which 2 were reniform, there is no mention of the sidewise prevalence or dimensions [15].
The present study reports 5 (8.3%) sieve STF. Jadhav reported 3.22% sieve STF. He studied 76 humeri and reported the presence of STF in 31, of which 1 was sieve while Veerappan et al., reported a 7.14% of sieve STF [27,28]. They were the first to describe this morphology of STF. Average distance from the tip of the medial epicondyle was 24.39 mm and 24.91 mm on left and right respectively. Average distance from the tip of the lateral epicondyle was 26.92 mm and 27.20 mm on left right respectively [Table/Fig-10,11].
On both sides the STF was closer to the medial epicondyle than to the lateral by 2-3 mm. This is in keeping with studies done by Nayak, Ndou, Soni, Veerappan, Krishnamurthy [12,13,25,28,29]. Average distance from trochlear margin was 14.41 mm and 14.29 mm on left and right respectively [Table/Fig-10]. Its closeness to articular ends of the humerus may come of significance in retrograde nailing of supracondylar fractures of humerus.
Of the 244 humerri inspected in the present study, 139 (56.8 %) showed translucency, whereas Ergdomus reported a substantially lower incidence of 17 (10.2%) in the166 bones he studied, of which 10 were observed on the right side [21]. Bhanu reported a 69% presence of translucency, chiefly on the left side [14]. In the present study there was an inconsequential difference in the prevalence of translucent septum between the sides, in that, 69 were on the left side and 70 were on the right side.
Clinical significance
Supracondylar fractures account for approximately 17% of paediatric trauma. Retrograde intramedullary nailing forms the mainstay of treatment [30]. As it is said that STF is associated with a narrow medullary cavity antegrade route may be preferred [11]. So knowledge of its presence helps decide the surgical course of action. STF appears relatively radiolucent and may commonly be confused with osteolytic or cystic lesion [22]. STF shows wide racial differences and hence can be used as a parameter in racial identification. Its link as an evolutionary trait can be used for dating specimens by the anthropologist [7,15].
Limitations
Unpaired dry bone of unknown race, gender and age were considered in the study. The effect of the ulnar morphometry and its bearing on the formation of STF could not be ascertained.
Conclusion
The STF is an entity familiar to the anthropologist and the anatomist, but has not received much notice from the clinician, evidenced by it cursory mention or not at all in most textbooks of clinical practice. As it is not a passage for any neurovascular structure, we propose that the term supracondylar aperture would be more apt terminology. Its existence is important to the orthopaedician in the preoperative planning of nailing fractures of the distal humerus and to the radiologist for differentiating it from an osteolytic or cystic lesion.