Necessity is the Mother of Invention
Ramanand Prasad Sinha1, Shivani Rakesh Kothari2, Ashok Suryakant Thakkar3
1 Assistant Professor, Department of Cardiology, Mahatma Gandhi Cardiac and Critical Care Center, Jaipur, Rajasthan, India.
2 Medical Writer, Department of Clinical Trials, Sahajanand Medical Technologies Pvt. Ltd., Surat, Gujarat, India.
3 Senior Manager, Department of Clinical Trials, Sahajanand Medical Technologies Pvt. Ltd., Surat, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ramanand Prasad Sinha, Assistant Professor, Department of Cardiology, Mahatma Gandhi Cardiac and Critical Care Center, Jaipur-302022, Rajasthan, India.
E-mail: rama100012@yahoo.com
A well executed transseptal puncture is crucial for successful percutaneous transvenous mitral balloon valvotomy. We report a case of accidentally damaged Mullins sheath dilator. Due to immediate unavailability of another dilator at cardiac catheterization laboratory, angioplasty guidewire and balloon was used as an additional assisting armamentarium for successful percutaneous transvenous mitral balloon valvotomy.
Balloon mitral valvotomy, Mullins dilator, Transseptal puncture
Case Report
A 54-year-old lady with severe rheumatic mitral stenosis, presented with dyspnoea and New York Heart Association (NYHA) class III symptoms. The chest skiagram revealed dilated left atrium (LA), dilated pulmonary artery (PA) and features of pulmonary venous hypertension. The two dimensional transthoracic echocardiography (TTE) and Doppler examination revealed dilated LA, severe mitral stenosis with Wilkins Score of 10/16 (leaflet mobility 2/4, valve thickness 3/4, subvalvular thickening 2/4, valvular calcification 3/4), valve area of 0.8 cm2 by planimetry and 0.7 cm2 by pressure half-time. The mean gradient across the mitral valve was 20 mm Hg with peak gradient of 28 mm Hg. The patient had chronic obstructive pulmonary disease and poor lung function. Moreover, the patient’s relatives were not willing for surgery. So, despite of high Wilkins score, the patient was not sent for surgery.
The patient was taken for elective PTMV by Inoue balloon. The transseptal puncture was made using Brockenbrough curved needle through 8-Fr Mullins dilator. The needle entry into LA was confirmed by measuring LA pressure and by contrast injection. Following confirmation, efforts were made to advance Mullins sheath dilator over needle, but the dilator did not advance over the needle. RAO projection view revealed that needle came out of the Mullins dilator, not from the tip of dilator but from a puncture point before the tip of dilator. Multiple unsuccessful attempts were made with same needle and dilator, but every time the needle protruded out from the same puncture point. Whole transseptal system was removed from the body and it was found that Mullins dilator shaft had a large hole before the tip of dilator. BPN needle is a sharp needle and at the time of advancement via sheath dilator, it’s tip did not remain coaxial due to bend at IVC and RA junction and hit the lateral wall of sheath and as a result a hole was created during the procedure.
Tip of the dilator was cut upto the hole of dilator and made blunt [Table/Fig-1a]. Again transseptal puncture was made and needle entered LA but dilator had a problem in advancing over the needle due to its blunt tip.
Blunt tip of Mullins dilator.

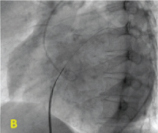
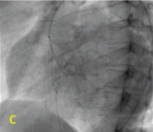
Then 0.0014-inch angioplasty guide wire (BMW, Abbot vascular) was advanced through the needle into left atrium and was stabilized in left superior pulmonary vein [Table/Fig-1b]. Angioplasty wire was left in the left atrium and whole system of transseptal needle and Mullins dilator was removed. A 3 × 20 mm noncompliant coronary balloon was placed over angioplasty wire across inter atrial septum and dilated at 24 mm Hg [Table/Fig-1c]. Followed by balloon dilations, septal dilator was used over angioplasty wire for septal dilation [Table/Fig-1d]. Keeping septal dilator across septum with tip in LA, angioplasty wire was removed and LA wire was passed through septal dilator [Table/Fig-1e]. The remaining procedure eventuated as the usual balloon valvotomy methods [Table/Fig-1f]. Post procedure echo revealed mild mitral regurgitation and mean gradient across mitral valve to be 8 mm Hg. Patient was discharged the following day.
Angioplasty wire in left upper pulmonary vein.
Angioplasty balloon across interatrial septum.
Septal dilation over angioplasty wire

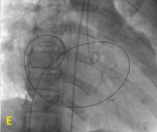
Fully inflated balloon across Mitral valve (valvular Ca++, both side of inflated balloon).

Discussion
The technique of transseptal catherization, developed by Cope and Ross has undergone a tremendous renaissance since its inception [1,2]. It has observed a transition from being an established technique for obtaining accurate left heart coverage to a vital component of percutaneous transvenous mitral balloon Valvotomy (PTMV). Transseptal puncture is a crucial component of balloon mitral valvotomy, which carries the risk of cardiac perforation and a consequent life threatening complications of cardiac tamponade. Moreover, the puncture of inappropriate septal site generates the difficulty in advancing Inoue balloon over mitral orifice. The technique has complication rate of only ~ 1% [3], and is generally safe in experienced hands. Mitral stenosis may be associated with hypertrophy of left or right atrium leading to changes in anatomical position of atrial septum. Therefore, there is no rule of thumb for successful transseptal puncture instead it should take the shape of tailored approach [4].
It has been rightly said, ‘Necessity is the mother of invention’. Our case revolves around this aphorism. The unavailability of another Mullins dilator in lab setting necessitated the technique to be performed with modification. An angioplasty guidewire was advanced over the needle and stabilized in pulmonary vein. An angioplasty balloon was used for dilation of inter atrial septum, instead of transseptal dilator, which would allow easy entry of transseptal dilator through its conical tip. Moreover, if transseptal dilator with blunt tip was used directly there were chances of whole system to come out due to septal resistance. Also, it was practically impossible to advance Inoue balloon over angioplasty wire due to bulky nature. With this in view, angioplasty wire was removed through septal dilator and LA wire was passed through it.
Hildick-Smith et al., have demonstrated enhanced safety of transseptal puncture with the use of angioplasty guide wire [5]. Our technique even uses angioplasty balloon along with angioplasty wire so that blunt tip of transseptal dilator could enter easily through dilated interatrial septum. This modification, which emerged due to necessity, takes the technique of transseptal puncture to a new horizon.
Conclusion
In case of accidental damage or unavailability of Mullins sheath dilator, an angioplasty guidewire and balloon are useful assisting armamentarium for successful percutaneous transvenous mitral balloon valvotomy.
[1]. Cope C, Technique for transseptal catheterization of the left atrium; preliminary reportThe Journal of thoracic surgery 1959 37:482-86. [Google Scholar]
[2]. Ross J, Braunwald E, Morrow AG, Transseptal left atrial puncture: new technique for the measurement of left atrial pressure in manThe American journal of cardiology 1959 3:653-55. [Google Scholar]
[3]. De Ponti R, Cappato R, Curnis A, Della Bella P, Padeletti L, Raviele A, Trans-septal catheterization in the electrophysiology laboratory: data from a multicenter survey spanning 12 yearsJournal of the American College of Cardiology 2006 47:1037-42. [Google Scholar]
[4]. Hung JS, Atrial septal puncture technique in percutaneous transvenous mitral commissurotomy: mitral valvuloplasty using the Inoue balloon catheter techniqueCatheterization and cardiovascular diagnosis 1992 26:275-84. [Google Scholar]
[5]. Hildick Smith D, McCready J, de Giovanni J, Transseptal puncture: use of an angioplasty guidewire for enhanced safetyCatheterization and Cardiovascular Interventions 2007 69:519-21. [Google Scholar]