Chronic obstructive pulmonary disease (COPD) is a major cause of mortality and morbidity worldwide whose burden is projected to increase in near future [1,2]. Prevalence of COPD ranges from 0.8% to 6.0% globally [3–5]. Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) is an event in the natural course of disease which has significant negative impact on the lung function, quality of life and survival [6–8]. All-cause mortality of these patients is as high as 49% within 3 years after hospitalization for AECOPD [9,10]. Exacerbations also involve enormous cost burden, especially in hospitalized patients [11]. These implications of AECOPD have attracted many researchers to explore ways to predict and prevent this event of paramount clinical importance. Several studies have attempted to predict and thereby prevent the occurrence of AECOPD especially severe forms leading to hospitalization [9,12]. However, when these patients get hospitalized for AECOPD, only limited data are available on how they utilize healthcare facility.
Healthcare utilization by patients admitted for AECOPD is characterized by varying periods of hospital stay, pharmacy consumption, need for various diagnostic modalities and at times ICU admissions with ventilatory or other life support measures. These characteristics, in particular length of hospital stay and ICU admissions, determine the overall outcome of AECOPD in terms of morbidity and mortality [13]. An increased healthcare utilization also means enormous burden to resource limited peripheral centres where these patients may get admitted for AECOPD. In this context, prediction of increased healthcare utilization for AECOPD at the time of admission may be useful for individualizing therapeutic approach and for rational allocation of limited resources to needy patients. This study attempted to characterize the pattern of healthcare utilization by COPD patients hospitalized for acute exacerbation, and to identify clinical and laboratory predictors of ‘prolonged hospital stay’(PHS) and ‘prolonged intensive care’(PIC) which in this study, defined increased health care utilization by these patients.
Materials and Methods
This study involved retrospective analysis of data from patients admitted with a primary diagnosis of AECOPD in a tertiary care teaching hospital in southern India, during a period from August 2012 to July 2013. After obtaining approval from the institutional ethics committee, the data were extracted from electronic medical database of the hospital using ICD-10 codes. Our review of past medical records revealed that the diagnosis of COPD in all patients was made based on spirometry along with characteristic clinical and radiological findings. All admissions for AECOPD were made when the patients had worsening breathlessness along with either increased purulence or quantity of sputum, severe enough to warrant hospitalization. Thus a sample of eligible admissions for AECOPD was identified for data extraction. The extracted data included demographic details, co-morbidities, clinico-laboratory and treatment related variables during admission for AECOPD. Data from hospitalizations which culminated with either of death or discharge against medical advice were excluded for evaluating predictors of PHS but included for PIC. Burden of co-morbidities was quantified by Charlson’s co-morbidity index. Exacerbations were categorized into three types based on the presenting symptoms of worsened breathlessness, sputum purulence and increased quantity of sputum as proposed by Anthonisen NR et al., [14]. Accordingly, type 1 exacerbation was defined when all three symptoms were present at the time of admission, type 2 exacerbation defined by breathlessness along with presence of either sputum purulence or increased quantity of sputum and type 3 exacerbation defined by worsened breathlessness in the absence of other foresaid symptoms. Majority of these patients had their spirometry done more than a year prior to admission and hence were not considered appropriate for defining the baseline severity of disease at the time of admission for AECOPD. Instead, we depended on indirect markers like exercise capacity by modified medical research council (mMRC) grading and chronic respiratory failure prior to hospitalization to define baseline severity of COPD.
Statistical Analysis
The in-hospital outcome variables were “Prolonged hospital stay” (PHS) and Prolonged intensive care” (PIC) which described increased healthcare utilization for AECOPD. PHS was defined by patients’ stay in ward and/or ICU for six or more days corresponding to the 75th percentile. PIC was defined when patients stayed in ICU for more than 48 hours during their hospital stay for AECOPD. The data were expressed as mean and standard deviation for quantitative variables and percentage for categorical variables. Predictors of PHS and PIC for AECOPD were evolved in two stages. Initially, independent variables were explored for their association with outcomes, using univariate analysis. Subsequently, variables significantly associated with outcomes at p ≤ 0.1, were enlisted to stepwise multivariate logistic regression analysis involving important covariates and odds ratio was calculated for significant variables. After identifying the independent risk factors, prediction models were evolved for the outcomes using the unadjusted β-coefficients. For an optimal use in clinical practice, only those variables easily available within few hours of admission were used to construct the prediction models. The discriminative properties of these models were tested using the receiver operating characteristics (ROC) curve and expressed in terms of area under the ROC curve with 95% confidence intervals. A cut-off was derived for each prediction model which had best sensitivity and specificity. All the statistical tests in this study, except univariate analysis, were performed with p< 0.05 considered as statistically significant. Analysis was carried out using statistical software SPSS version 19.5 (IBM corporation).
Results
In all, 255 admissions by 166 patients were found to be eligible for data extraction. Demographic and disease related characteristics during stable state and at the time of admission for AECOPD are summarized in [Table/Fig-1].
Demographic and disease characteristics of study population.
| Variables | N = 255£ |
|---|
| Baseline characteristics |
| Age (in years) | 63.85 ± 9.71 |
| Male gender | 255 (100%) |
| BMI (Kg / m2) | 21.60 ± 4.08 |
| Age of onset of COPD (in years) | 57.26 ± 8.62 |
| Duration of illness (in years) | 6.64 ± 4.92 |
| Smoking (pack years) | 32.57 ± 15.59 |
| History of alcohol intake (past / current)£ | 47 (28.3%) |
| Presence of atleast one co-morbid condition£ | 122 (73.5%) |
| Baseline saturation (SPO2) during stable disease (%) | 94.30 ± 3.92 |
| Baseline exercise capacity (MMRC grade)£ |
| Grade 1 | 1 (0.6%) |
| Grade 2 | 14 (8.4%) |
| Grade 3 | 99 (59.6%) |
| Grade 4 | 52 (31.3%) |
| Characteristics during hospital stay for AECOPD |
| History of fever | 46 (18.0%) |
| Sputum purulence | 106 (41.6%) |
| Increased of sputum quantity | 154 (60.4%) |
| Anthonisen’s type of AECOPD |
| Type 1 | 71 (27.8%) |
| Type 2 | 108 (42.4%) |
| Type 3 | 76 (29.8%) |
| Presence of features of right heart failure | 26 (10.2%) |
| Saturation at the time of admission | 87.07 ± 14.14 |
| Positive isolate in sputum culture | 50 (19.6%) |
£ A total of 166 patients with COPD had 255 admissions for acute exacerbation.
All patients were male and were current or past smokers with a mean smoking pack years of 32.57±15.59. One hundred and twenty two (73.5%) had at least one co-morbid condition. Burden of co-morbidity in these patients was quantified as per Charlson’s Co-morbidity index which indicated the following: eleven (6.8%) patients with score 1; twenty two (13.5%) with score 2; thirty nine (24.0%) with score 3; thirty five (21.6%) with score 4; thirty six (22.2%) with score 5; fourteen (8.6%) with score 6; two (1.2%) with score 7; three (1.8%) patients had a score of 8 and data were missing for 4 patients. A vast majority of patients (91%) had grade 3 or 4 dyspnea as per modified medical research council grading (mMRC) prior to hospitalization indirectly indicating a severe form of disease state at baseline. Fifty admissions (19.6%) were associated with sputum cultures having positive isolates, most commonly Pseudomonas aeruginosa (28.0%) followed by Klebsiella pneumonia (20.0%), Streptococcus pneumonia (16.0%), Candida species (14.0%), Haemophilus influenza (10.0%), Acinetobacter baumanii (6.0%) and other organisms (6.0%). There was no association between positive isolates in sputum culture and sputum characteristics like increased purulence or quantity.
Duration of hospital stay for AECOPD ranged from 3 to 43 days with a mean of 5.39 ± 3.76 days. Hospitalization for 4, 5 and 6 days corresponded to 25th, 50th and 75th percentile respectively. Accordingly, duration of ≥ 6 days was defined as PHS which was observed in 71 (27.8%) admissions. Forty one admissions (16.1%) involved PIC for AECOPD during which time 19 (7.5%) required noninvasive and/or mechanical ventilator support. Results of logistic regression analysis of association between clinico-laboratory variable and outcome variables are summarized in [Table/Fig-2].
Logistic regression analysis of clinico-laboratory variables predicting prolonged hospital stay and prolonged intensive care for AECOPD.
| Variables | Unadjusted odds ratio(95% CI) | Adjusted odds ratio§(95% CI) |
|---|
| Predictors of prolonged hospital stay for AECOPD |
| Body mass index | 1.062 (0.994 – 1.134)# | 1.056 (0.977 – 1.142) |
| Duration of COPD | 1.051 (0.996 – 1.109)# | 1.025 (0.952 – 1.104) |
| Increased sputum production | 1.832 (1.018 – 3.295)* | 1.805 (0.950 – 3.433) |
| Chronic respiratory failure | 2.838 (1.598 – 5.041)**** | 1.980 (1.024 – 3.828)* |
| Saturation at admission for AECOPD | 0.945 (0.924 – 0.966)**** | 0.956 (0.931 – 0.981)*** |
| Total leukocyte count | 1.077 (1.021 – 1.135)** | 1.055 (0.944 – 1.119) |
| Blood sugar on admission | 1.005 (1.001 – 1.009)* | 1.003 (0.999 – 1.008) |
| HbA1c level | 1.722 (1.255 – 2.364)*** | 1.601 (1.097 – 2.337)* |
| Serum creatinine | 2.050 (1.008 – 4.169)* | 1.722 (0.769 – 3.853) |
| Positive isolate in sputum culture | 4.765 (2.483 – 9.146)**** | 4.393 (2.084 – 9.261)**** |
| Predictors of ICU admissions for AECOPD |
| Smoking pack years | 1.028 (1.006 – 1.050)* | 1.021 (0.996 – 1.047) |
| Past history of pulmonary TB | 2.200 (1.087 – 4.453)* | 3.278 (1.410 – 7.621)** |
| Chronic respiratory failure | 3.605 (1.812 – 7.173)**** | 4.927 (1.803 – 10.24)** |
| Saturation at admission for AECOPD | 0.938 (0.911 – 0.986)**** | 0.932 (0.902 – 0.963)**** |
| Total leukocyte count | 1.067 (1.009 – 1.128)* | 1.084 (1.015 – 1.157)* |
| Blood sugar on admission | 1.005 (1.001 – 1.010)* | 1.003 (0.954 – 1.011) |
| HbA1c | 1.425 (1.025 – 1.979)* | 1.381 (0.967 – 1.972) |
| Serum sodium | 0.930 (0.863 – 1.003)# | 0.948 (0.875 – 1.026) |
| Positive isolates in sputum culture | 2.934 (1.412 – 6.090)** | 2.173 (1.001 – 4.930)* |
# P > 0.05 < 0.1; *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001;
§ Adjusted model for age, BMI, baseline exercise capacity (mMRC grade) and Charlson’s co-morbidity index
In multiple logistic regression analysis, chronic respiratory failure at baseline, low saturation at the time of admission for AECOPD, poor glycaemic control (HbA1c) and positive isolates in sputum culture were found to be predicting PHS independent of age, BMI, Charlson’s co-morbidity score and baseline exercise capacity by mMRC grading. Similarly, past history of pulmonary tuberculosis, chronic respiratory failure at baseline, low saturation and high leukocyte count at admission and positive isolates in sputum culture emerged as independent predictors of PIC after adjusting for the co-variates.
Prediction models were derived for prolonged hospital stay and prolonged intensive care, using all significant variables available at admission (i.e., except sputum culture report) and their unadjusted regression coefficient beta. Prediction equation for discriminating patients with prolonged hospital stays as follows:
Score = 4.18 + {0.34 x chronic respiratory failure} – {0.07 x saturation at admission (%)} + {0.43 x HbA1c (%)}
ROC curve analysis of prediction model for PHS showed an AUC of 0.805 (95% CI 0.729 – 0.881) [Table/Fig-3].
ROC curve analysis of prediction model for PHS.
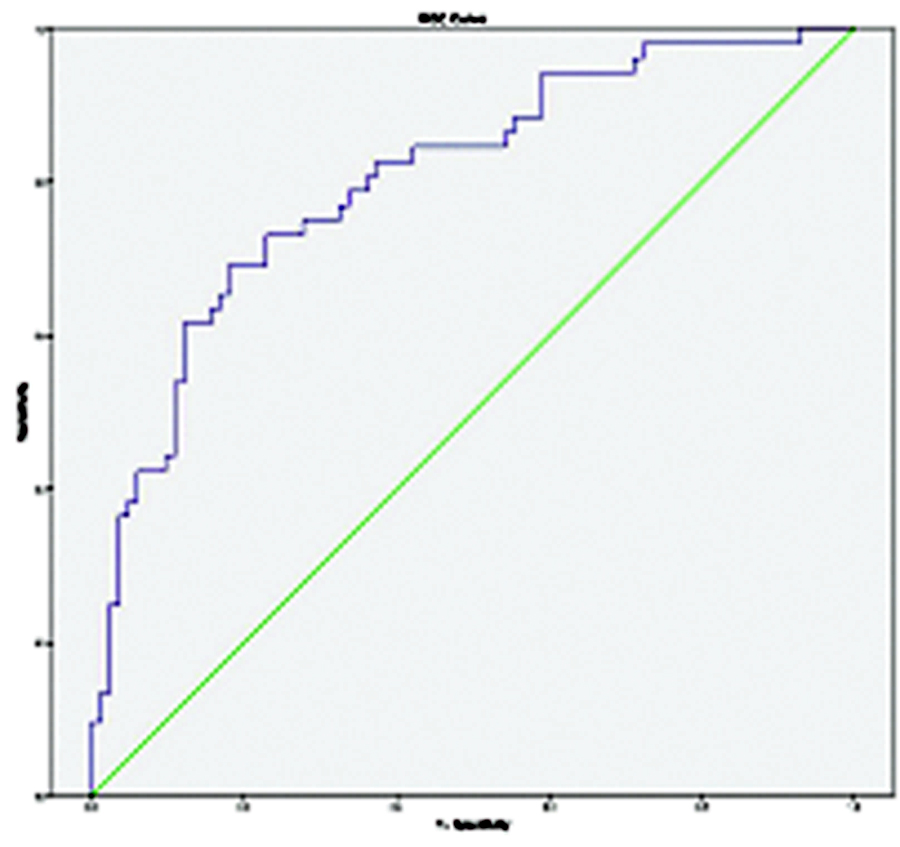
Hosmer – Lemeshow goodness of fit test for the model showed good calibration (p = 0.882). A cut-off score of ≥1 had a sensitivity of 75.0% and specificity of 72.3% for identifying patients at risk for PHS. Prediction equation for discriminating patients requiring prolonged intensive care as follows:
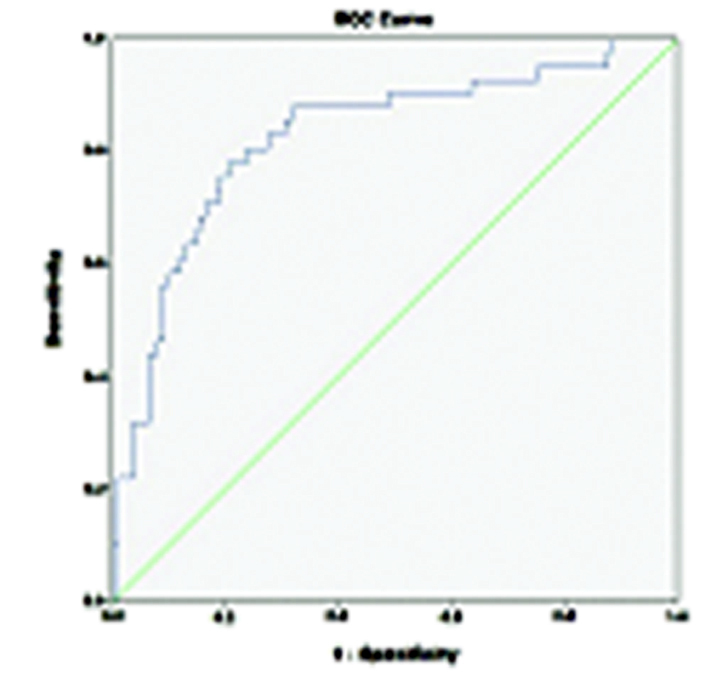
Score = 4.4 + {1.2 x past h/o pulmonary TB} + {0.74 x chronic respiratory failure} – {0.051 x saturation at admission (%)} + {0.06 x total leucocyte count per μL}
ROC analysis of prediction model for PIC had an AUC of 0.825 (95% CI 0.75 – 0.90) [Table/Fig-4]. Hosmer – Lemeshow goodness of fit test for the model showed good calibration (p = 0.396). A cut-off score ≥ 1 had sensitivity and specificity of 80.5% and 76.1% respectively for identifying patients at risk for PIC.
ROC analysis of prediction model for PIC.
Discussion
This study has identified various clinical and laboratory predictors of increased healthcare utilization for AECOPD, defined in terms of ‘prolonged hospital stay’ and ‘prolonged intensive care’. We believe that the findings of our study represented a typical Indian scenario of healthcare utilization by COPD patients admitted for acute exacerbations. It is noteworthy to highlight differences in health delivery system of Indian subcontinent compared with that of the western world, such as socioeconomic and cultural differences, high turnover of patients, limited access to mediclaim and other social security schemes etc. In this context, the mean length of hospital stay in our study was shorter than what was reported in many studies from the western world [15,16]. The defining cut-off (≥6 days at 75th percentile) for ‘prolonged hospital stay’ was shorter in our study which we consider appropriate for a setting with limited resources and high patient turnover. We found several variables predicting prolonged hospital stay and prolonged intensive care, independent of cofounders like age, BMI, co-morbidities and baseline exercise capacity.
Low oxygen saturation during AECOPD predicted prolonged hospital stay and prolonged intensive care in our study population. Soltani A et al., who prospectively evaluated the outcomes of 218 hospitalizations for AECOPD and found low oxygen saturation at admission predicting longer hospital stay and in-hospital mortality [17]. We could not study the effects of hypoxemic or hypercapnic respiratory failure on the outcome variables since arterial blood gas values were missing in a significant proportion of cases. Patients with chronic respiratory failure during stable state were also found to be more likely have prolonged hospital stay and prolonged intensive care for AECOPD. Studies have shown that chronic respiratory failure during stable COPD is associated with prolonged hospital stay for AECOPD whereas use of LTOT (length of oxygen therapy) shortened the length of hospital days [18]. Ringbaek TJ et al., evaluated the pattern of healthcare utilization by 246 COPD patients with respiratory failure and found that these subjects had prolonged hospital stay for AECOPD when they never used LTOT and shorter hospital stay for exacerbations when they started using LTOT [19]. This benefit of LTOT on length of hospital stay was found by the authors irrespective of duration of oxygen use in a day (continuous or nocturnal). In our study, 26 patients (15.6%) had baseline saturation ≤88% in room air, identifying them as eligible candidates for home oxygen therapy. However, data on their compliance with home oxygen therapy were missing or too unreliable to be used for analysis.
Glycaemic profile is a well-known predictor of morbidity and mortality in COPD. Several studies have substantiated the association between hyperglycaemia and adverse outcomes of AECOPD [17, 20]. Baker EH et al., retrospectively analysed 284 patients admitted for AECOPD and found that blood glucose of ≥ 7 mM was significantly associated with increased risk of mortality and prolonged hospital stay independent of age, gender, diabetes and severity of COPD [21]. However, this study could not fully elucidate the relative contribution of stress due to acute illness, steroid therapy and underlying diabetes mellitus. Parappil A et al., in their retrospective study of 246 admissions for AECOPD, found a trend towards statistical significance in association between co-morbid diabetes and prolonged hospital stay and mortality [22]. However, this association did not withstand adjustment with important confounders. Hyperglycaemia at admission and overall glycaemic control of diabetic patients were not analysed in this study. In our study blood sugar level at admission i.e., measured before initiation of steroid therapy, did not predict prolonged hospital stay or prolonged intensive care when adjusted for confounders. However overall glycaemic control (HbA1c) was independently associated with prolonged hospital stay but not prolonged intensive care. Our subjects were 1.60 times more likely to have prolonged hospital stay for AECOPD for every 1 standard deviation above the mean HbA1c level. Poor glycaemic indices may contribute to adverse outcomes in AECOPD by facilitating pulmonary infections. Moretti et al., speculated that outcomes of AECOPD like late NIV failures and mortality in subjects with hyperglycaemia may be contributed by pulmonary infections [20]. In our study, neither blood glucose at admission nor HbA1c was found to be associated with any of the variables indicative of infection, like fever, sputum characteristics nor does positive culture isolate in sputum. Thus we speculate that unknown mechanisms other than infection could have contributed to prolonged hospital stay in our patients with AECOPD and poor glycaemic control.
Past history of pulmonary tuberculosis was shown in this study, to be independent predictor of prolonged intensive care but not the length of hospital stay. Prevalence of coexisting pulmonary TB sequalae in our study (25.4%) was similar to that reported by other studies from India [23,24]. None of our patients had active TB during their admission for AECOPD. Chronic sequalae of TB like fibrosis and bronchiectasis is known to alter the phenotype of COPD and its outcomes [25]. Poorer lung function due to such sequalae of past tuberculosis could have rendered a subset of our patients vulnerable for early decompensation and delayed recovery in ICU. In countries like India with high burden of tuberculosis, this intriguing association warrants consideration while predicting outcomes of AECOPD.
Role of bacterial infection in AECOPD has been extensively studied especially in the context of outcomes and antibiotic use for managing exacerbations [26,27]. Outcomes of AECOPD in hospitalized patients appear to be affected neither by the infective etiology of the event nor by antibiotic usage. At least two studies have denied any association between bacterial infection and length of hospital stay or need for intensive care [28,29]. In our study, positive isolate in sputum culture and high total leukocyte counts as laboratory markers of bacterial infection were significantly associated with prolonged hospital stay and prolonged intensive care. However, we could not find any association between the outcome variables and clinical markers of infection like fever and sputum characteristics.
Our prediction models showed good discriminative properties in identifying patients at risk for prolonged hospital stay for ≥ 6 days and prolonged intensive care for ≥ 48 hours. These models were evolved with information available from history or basic diagnostic tests and thus making them useful even in settings with limited resources and expertise like primary health centers and smaller hospitals. All predictors included in these models can be made available within few hours of patients’ arrival at emergency room so that decision on admission or transfer to higher centers is possible without delay. Our prediction models require further validation for its optimal use in clinical practice.
Limitation
Other limitations in our study are inherent for any retrospective data analysis. Due to missing values, we could not include in data analysis, several important variables like spirometry, arterial blood gas analysis, details on home oxygen therapy, mortality outcomes etc. These variables could have added significant value to the results of this study.
Conclusion
In conclusion, the purpose of this retrospective data analysis was to identify predictors of increased healthcare utilization for AECOPD namely prolonged hospital stay and prolonged intensive care. We found that a significant proportion of patients admitted for AECOPD have increased utilization of healthcare facility. The present study has evolved simple prediction models that involve clinical and inexpensive laboratory variables, thus enabling their use even in health care settings with limited resources and expertise. These models have shown good discriminative properties in identifying patients at risk for PHS and PIC, soon after their entry to healthcare facility for AECOPD. Such predictions are useful for rational allocation of limited resources while managing these patients. We recommend prospective validation of these models in larger samples to facilitate their use in clinical practice.
£ A total of 166 patients with COPD had 255 admissions for acute exacerbation.
# P > 0.05 < 0.1; *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001;
§ Adjusted model for age, BMI, baseline exercise capacity (mMRC grade) and Charlson’s co-morbidity index