Glycopeptide antibiotics remain the drug of choice for infections caused by resistant Enterococcus species and Methicillin Resistant Staphylococcus aureus (MRSA). Enterococci with a MIC of ≥32μg/ml are classified as vancomycin resistant Enterococci(VRE). Staphyloccus aureus isolates with a MIC of 4-8μg/ml are termed as Vancomycin Intermediate Staphyloccus aureus (VISA) and those with a MIC of ≥16μg/ml are termed as Vancomycin Resistant Staphylococcus aureus (VRSA). Vancomycin resistant Enterococci have emerged as important nosocomial pathogens in the last two decades throughout the world [1]. VRE are associated with many infections ranging from mild to life threatening. Extensive use of vancomycin to treat infections with MRSA has led to decreased susceptibility to vancomycin among Staphylococcus aureus. As of today very limited options are available for treating serious infections caused by VRE and VRSA [1].
VISA, VRSA and VRE are important nosocomial emerging pathogens resulting in treatment failures. This study was undertaken to detect vancomycin resistance among Staphylococcus aureus and Enterococcus faecalis isolates by both phenotypic and genotypic methods.
Materials and Methods
Study Isolates
The study was conducted in a 1850 bedded university teaching hospital from November 2013 to April 2014. Institutional ethics committee approval was obtained. Bacterial isolates consisting of non-repetitive, consecutive clinically significant Staphylococcus aureus(109) and Enterococcus faecalis(124) were included in this study. Staphylococcus aureus isolates were collected from blood(8), respiratory(2) and exudative(99) samples. The Enterococcus faecalis were collected from urine(57) and exudative(67) samples.
The exclusive criteria included the isolates from non admitted patients and the isolates which were not clinically significant. The isolates were speciated by using routine biochemicals and automations. (Microscan Walk Away 96).
Antibiotic Susceptibility
Disc Diffusion
Antibiotic susceptibility was tested with gentamycin (10μg), ciprofloxacin (5μg), erythromycin (10μg), clindamycin (2μg), teicoplanin (30μg) and linezolid (30μg) for Staphylococcus aureus by disc diffusion method according to Clinical Laboratory Standards Institute (CLSI) guidelines [2]. For Enterococcus faecalis, antibiotic susceptibility was tested with high level gentamycin (120μg), ciprofloxacin (5μg), vancomycin (30μg), teicoplanin (30μg) and linezolid discs (30μg) for all isolates, erythromycin (10μg) for exudative isolates, nitrofurantoin (300μg) for urinary isolates by disc diffusion method [2]. All the discs were procured from Hi-media laboratories, Mumbai, Maharashtra, India.
Minimum inhibitory concentration
MIC of vancomycin for all the test isolates was determined by agar dilution method; the range tested being 0.008μg/ml to 256μg/ml in accordance to CLSI guidelines [2].
Phenotypic Tests
Induced resistance for clindamycin was detected by D test. Methicillin resistant Staphylococcus aureus (MRSA) was screened using cefoxitin disc (30 μg).
Molecular Detection of Genes
All the isolates were subjected to PCR targeting van A and van B. Staphylococci isolates were tested for mec A also. A single colony was inoculated in Luria-Bertini broth and incubated for 20 hours with shaking in between and 1.5 ml of this was centrifuged for 5 minutes. The pellets were suspended in 500 μl of distilled water and lysed by heating at 95°C for 5 minutes and centrifuged for 1 minute. Fiveμl of this extract was used as a template for amplification. The following is the list of primers used [Table/Fig-1].
Primer Sequence for van A, van B and mec A [3]
| Primer | Primer sequence 5’–3’) | Product size | annealing temperature |
|---|
| van A | P1 = GCT ATTCAG CTG TAC TCP2 = CAG CGG CCA TCA TAC GG | 783 bp | 56°c |
| van B | P1 = CAT CGC CGT CCC CGA ATT TCA AAP2 = GAT GCG GAA GAT ACC GTC GCT | 297 bp | 56°c |
| Mec A | F = ATC GAT GGT AAA GGT TGG CR = AGT TCT GCA GTA CCG GAT TTG C | 530 bp | 58°c |
PCR Conditions: Initial denaturation - 95oC - 3 min
Denaturation - 94oC - 1 min
Annealing - 56oC - 1 min (van A & van B)
Extension - 72oC - 1 min
Final Extension - 72oC - 5 min
PCR Product: PCR Product of 782 bp (van A) & 297 bp (van B) were visualised by Agarose gel electrophoresis.
Results
Disc Diffusion (Staphylococcus aureus)
Fifty four isolates were resistant to cefoxitin disc (MRSA). The resistance to gentamycin, ciprofloxacin, erythromycin are 36.6%, 57.7% and 41.2% respectively. Constitutive resistance to clindamycin was 20.1%. All isolates were susceptible to teicoplanin and linezolid. By D test 10% of the isolates exhibited inducible resistance to clindamycin.
Disc Diffusion (Enterococcus faecalis)
The resistance to high level gentamycin, ciprofloxacin, erythromycin and nitrofurantoin were 45.6%, 79.03%, 76.19% and 38.18% respectively. Vancomycin and teicoplanin resistance was exhibited in 12.9%(16) and 3.2%(4) isolates respectively. All isolates were susceptible to linezolid.
Minimal Inhibitory Concentration
Staphylococcus aureus
MIC of vancomycin ranged from 0.125μg/ml to 2μg/ml.MIC50 was 1μg/ml. There was no resistance observed to vancomycin.
Enterococcus Faecalis
MIC ranged between 0.25-256 μg/ml. MIC50 was 1 μg/ml.4 isolates were resistant to vancomycin. Two of them had MIC of >256μg/ml, one with a MIC of 256μg/ml and one with a MIC of 128μg/ml. Two were in the intermediate range with a MIC of 8 μg/ml and 16μg/ml.
Polymerase Chain Reaction
Staphylococcus aureus
Mec A gene was detected in 15 isolates. None of the isolates were positive for van A and van B.
Enterococcus faecalis
Two isolates harboured van A and seven isolates harboured van B. In one isolate both van A and van B genes were detected [Table/Fig-2].
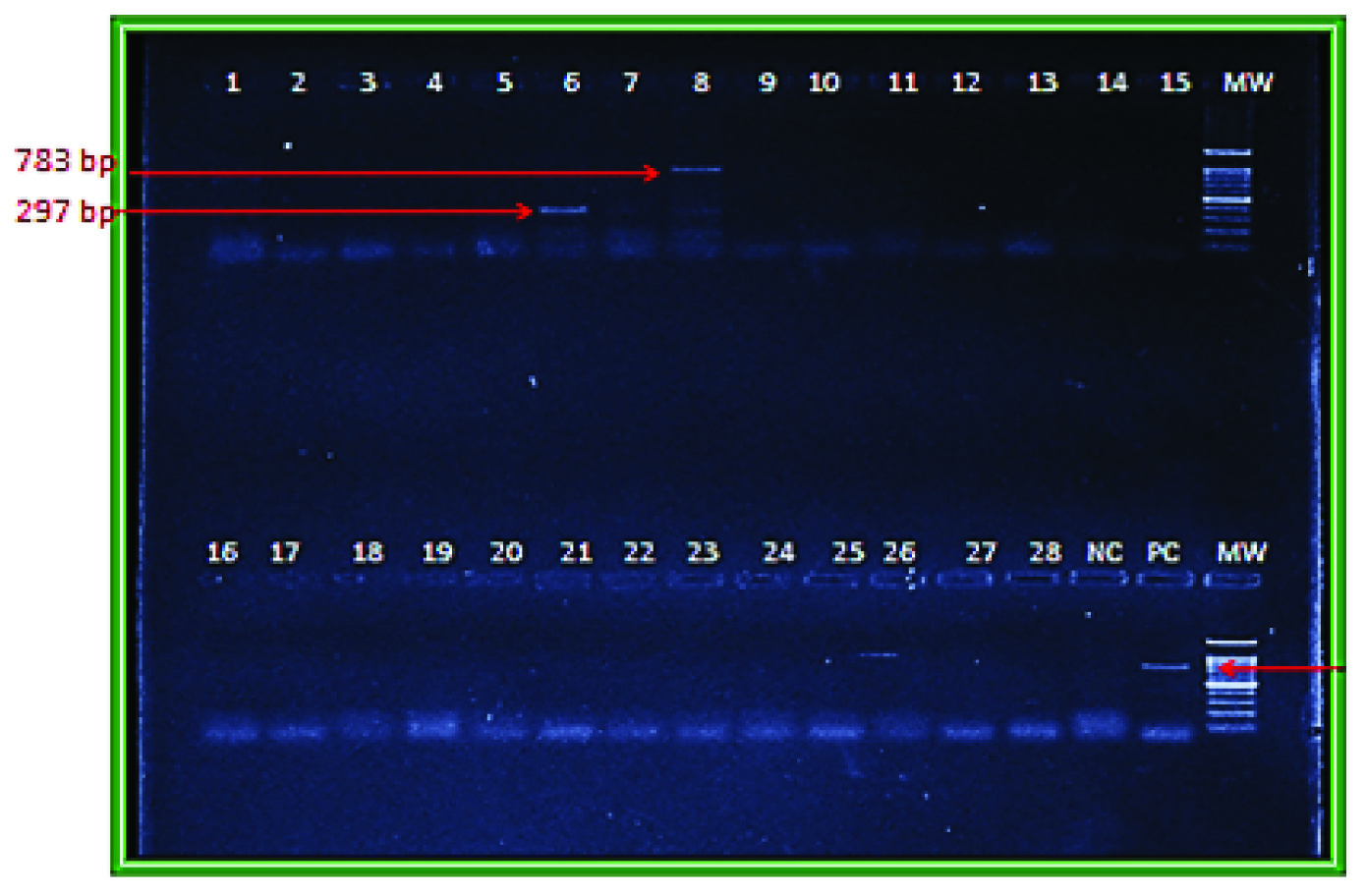
Detection of van A and van B gene by PCR
Lane 6: band for van B at 297 bp
Lane 8: band for van A at 783 bp
MW: Molecular Ladder
Comparitive Results of MIC and PCR
Out of 4 isolates which were resistant by MIC, one isolate (MIC>256μg/ml) was positive for van A. Other three were neither van A nor van B positive. Out of 2 isolates with van A, one had MIC in resistant range (256μg/ml), other with MIC in intermediate range (16μg/ml). All seven isolates with van B had MIC in a susceptible range (1μg/ml). The isolate with both van A and van B had a MIC in intermediate range (8 μg/ml).
Discussion
Vancomycin is a glycopeptide discovered as early as 1950. It acts by preventing synthesis of peptidoglycan precursors of cell wall by blocking transglycosylation and transpeptidation steps essential for cross linking. Site of action is on D-ala D-ala residue of the polypeptide [1]. Vancomycin has been used as the drug of choice in serious infections caused by MRSA and resistant Enterococci. Resistance of these organisms to vancomycin is being reported since last two decades. Vancomycin intermediate Staphylococcus aureus was first reported by Hirmatsu et al., from Japan in a four month old infant with pulmonary atresia in 1997 [4]. Tiwari and Sen were the first to report VISA strains from Indian subcontinent [5]. However, a fully resistant strain of Staphylococcus aureus to vancomycin was reported only in 2002 from Michigan, US [6].
This study included a total of 109 Staphylococcus aureus isolates from various samples. Fifty four isolates (49%) out of them were MRSA by cefoxitin disc diffusion method. Joshi et al., reported MRSA prevalence of around 40% [7]. Another study from Hyderabad reported MRSA as high as 79.6% [8]. Fifteen of the cefoxitin resistant isolates carried mecA. According to one study strains phenotypically resistant to cefoxitin but mec A negative may probably due to mec C [9]. The other 39 cefoxitin resistant isolates have to be further screened for mec C and other non mecA mediated resistance. The resistance to gentamycin, ciprofloxacin, erythromycin are 36.6%, 57.7% and 41.2% respectively.
All isolates of Staphylococcus aureus were susceptible to vancomycin with MIC50 of 1μg/ml, None of the isolates harboured van A or van B by PCR. This was similar to another study conducted in South India which also reported no resistance to vancomycin by MIC [10]. Thati et al., reported 1.9% VRSA and 4.46% VISA isolates by MIC [8]. Their study also revealed high percentage of resistance among VRSA isolates to other antimicrobials also. A van gene negative VRSA was also reported by them. Tiwari and Sen also reported a van gene negative VRSA from northern part of India [5].
Enterococci, apart from being a part of normal microbiota also cause nosocomial infections. The first VRE was reported by Uttley et al., in 1977 from Great Britain [11]. In India, the first VRE was reported by Mathur et al., in 1999 [12]. Our study included 124 Enterococcus faecalis isolates 67 0f which were from exudates and 57 from urine. The resistance to high level gentamycin, ciprofloxacin, erythromycin and nitrofurantoin were 45.6%, 79.03%,76.19% and 38.18% respectively. Another study reported resistance of 37%, 74.38% and 29% to high level gentamycin, ciprofloxacin and nitrofurantoin among Enterococci [13].
Van A and Van B are the most common genotypes among Enterococci. Van A is associated with high level resistance to both vancomycin (MIC≥64μg/ml) and teicoplanin (MIC≥16μg/ml). Van B is associated with varying levels of resistance to vancomycin alone(MIC 4 -1000 μg/ml) with susceptibility to teicoplanin [14]. In this study, by MIC determination four isolates were vancomycin resistant and one isolate exhibited intermediate susceptibility to vancomycin. The isolate that harboured the van A gene had a MIC of 256μg/ml. The other three neither carried van A nor van B. They have to be screened for other van genes (van D, van E, van J, van L, van M) for further characterization [1]. By PCR two isolates were van A Positive. One had a MIC of 256μg/ml. Other had a MIC of 16 μg/ml showing low level resistance to vancomycin. Such van A genotype –van B phenotype incongruency has also been reported in other studies in Enterococcus faecalis and Enterococcus faecium [13,15,16]. Park et al., suggested presence of insertion sequence IS 1216v in coding region of van S gene as a probable reason for this incongruency [16]. According to other authors this is due to mutations in van A gene cluster or in van S regulatory element [17,18].
Seven isolates were positive for van B. All of them had a susceptible MIC of 1 μg/ml. Van B VRE with susceptible MIC were already reported in few studies in Enterococcus faecium [19,20]. The reason for this phenotype-genotype incongruence is not known. One isolate which carried both van A and van B had an MIC of 8μg/ml. By PCR, 8% of all Enterococcus isolates are VRE. Another study conducted in South India reported 8.7% VRE [11]. van B was the most common phenotype. This is in contradiction to many studies which report van A as the commonest phenotype [13,19].
Conclusion
Resistance to vancomycin was not detected among isolates of Staphylococcus aureus both phenotypically and genotypically. However, MIC creep is a cause for concern. Among Enterococcus faecalis isolates, 8% were VRE by PCR. High resistance percentage to other antibiotics among Enterococcus faecalis isolates was also recorded. van A genotype –van B phenotype incongruence was observed in two of the test isolates. Another important finding is VRE isolates with susceptible MIC. van B was the commonest genotype. PCR remains the gold standard for diagnosis of vancomycin resistance. Emerging vancomycin resistance among Enterococcus faecalis is a cause for concern as this leads to a great difficulty in treating the serious infections caused by them. Prudent use of antibiotics with good infection control practices will help to retain their susceptibility.