Introduction
The principle behind the generation of the Korotkoff sounds is the turbulence of blood flowing through a partially occluded area in the artery. With increasing age, the vascular wall compliance is expected to decrease, which is due to the thickening of the vessel wall, due to which the amplitude of the transmitted Korotkoff sounds is decreased. There is also an accompanying rise in the systolic B.P. and pulse pressure.
Aim
To record and compare the amplitudes of the intermediate Korotkoff sounds and the blood pressures in individuals of the two age groups, and calculate the pulse pressure and determine whether they vary in relation to the amplitude of the intermediate Korotkoff sounds recorded.
Materials and Methods
The cross-sectional study was conducted on 50 young subjects (15-25 years) and 50 older subjects (50-70 years). The mid arm circumference was measured using a tape. A phonoarteriogram was placed over the left brachial artery and the sphygmomanometer cuff was tied 2cm above the cubital fossa of the left arm. The blood pressure was recorded using the Lab Tutor software. The Korotkoff sounds picked up and transmitted by the phonoarteriogram are represented as distinct lines on the graphical recording.
Statistical Analysis
Independent samples t-test to look for significant mean amplitude differences and for correlating mean amplitude and pulse pressure. Null hypothesis rejected at p<0.05. Data analysed using the SPSS software version 20.0 (SPSS Inc.).
Results
There was a significant difference in the mean amplitudes of Korotkoff sounds among the different age groups (p=0.001) and subject categories (p=0.043 among males, p=0.037 among females). A significant difference in pulse pressures was also seen among different age groups and subject categories. The decrease in the amplitudes of Korotkoff sounds in the older age group accompanies the increase in pulse pressures seen in this group and the same was seen among the different age groups within each sex (r=-0.574, p=0.001 among males) and (r=-0.449, p=0.002 among females).
Conclusion
Measuring the amplitude of Korotkoff sounds can give us an idea of the nature of the arterial wall as shown by a decrease in amplitude in older individuals when compared to the younger individuals and of the volume of blood flowing through the artery as shown by the higher amplitudes observed in males when compared to females.
Arteriosclerosis, Pulse pressure, Phonoarteriogram
Introduction
The use of sphygmomanometer for the measurement of blood pressure has been widely practiced for a long time. The auscultatory method of measuring blood pressure involves the auscultation of Korotkoff sounds by means of a stethoscope. The principle behind the generation of the Korotkoff sounds is the turbulence of blood flowing through a partially occluded area in the artery. The Equation of Continuity and the Law of Conservation of Energy are used to explain the role of vascular compliance in the production of the Korotkoff sounds [1]. Accordingly, it can be stated that, the more compliant an artery is, the better is the production of Korotkoff sounds since the more elastic walls flutter due to turbulent blood flow at intermediate pressures produced by the sphygmomanometer cuff used in measuring B.P.
The Korotkoff sounds are used mainly to detect the values of systolic B.P. and diastolic B.P. This is done by noting the levels at which the Korotkoff sounds initially appear and then disappear respectively. The intermediate Korotkoff sounds are generally ignored in routine studies. However, the nature of the intermediate Korotkoff sounds can give us a clue about the degree of compliance of the vascular wall [1].
The vascular wall compliance is expected to decrease with increasing age [2], which is due to the thickening of the vessel wall [3]. Due to reduced compliance, the amplitude of the transmitted Korotkoff sounds is decreased. There is also an accompanying rise in the isolated systolic B.P. and pulse pressure [4,5]. This is because, as the arterial compliance decreases, there is an increase in the pulse wave velocity. The pulse wave rapidly rebounds from the branching points in the artery and superposes earlier during systole resulting in systolic pressure augmentation.
Thus, the relatively inelastic arterial walls are the causes of both the increased pulse pressure due to the isolated rise in systolic B.P. and the reduced flutter at intermediate cuff pressures with the possible reduction in the amplitude of the Korotkoff sounds.
By using a phonoarteriogram, one can detect the amplitude of the Korotkoff sounds produced [6]. The experiment is carried out in the laboratory by making use of the laboratory instruments (AD Instruments) and software (Lab Tutor). The Korotkoff sounds detected and the sphygmomanometer cuff pressure are converted into electrical inputs which are shown as a graphical recording by the software.
As opposed to detecting the Korotkoff sounds using the software, in the regular measurement of blood pressure, the sounds heard are classified based on the intensity of the sounds heard which is subjective to the examiner’s hearing. The laboratory analysis, however, gives an objective outlook to these sounds and this can be made use of.
The purpose of this study was to determine whether a relation can be established between the pulse pressure and amplitude of the Korotkoff sounds in older individuals as compared to those of the younger individuals. If it is possible to ascertain a correlation between an increase in pulse pressure and an expected decrease in amplitude of Korotkoff sounds - both of which can be attributed to decreased vascular compliance that occurs with ageing [2], then it would have prognostic implications in situations where there is a pathological alteration in the blood vessel and its properties.
Aim
To record the amplitudes of the intermediate Korotkoff sounds and compare them in individuals of two age groups. Also to record the blood pressure of the individuals of the two age groups, and calculate the pulse pressure and determine whether they vary in relation to the amplitude of the intermediate Korotkoff sounds recorded.
Materials and Methods
The cross sectional study was conducted on 50 young individuals (25 males and 25 females) and 50 old individuals (25 males and 25 females). Simple random sampling was employed
Inclusion Criteria
Individuals over two different age groups were selected. One group consisted of individuals between 15-25 years of age. The second group consisted of individuals above 50 years of age: this was because age related changes in the vasculature could be compared.
Mid arm circumference as specified by National Health Statistics Reports - 2008 [7] with values taken between 15 & 85 percentiles for the specified age groups: this was because, within the same age group, an individual with more muscle mass has a greater blood flow and this may interfere with the test results. Mid arm circumference values also help in the inclusion of well-nourished individuals.
Exclusion Criteria
Individuals with history of diabetes, hypertension, peripheral vascular disease or peripheral neuropathy: this may interfere with the test results due to its independent effect on vascular compliance [1].
Female subjects who were pregnant: this may interfere with the test results due to its effect on volume of blood flow [1].
Signed informed consent forms were taken from every individual. Data collection forms were used. Laboratory equipments included sphygmomanometer, phonoarteriogram, pressure transducer and measuring tape. Data analysing software used was Lab Chart software and AD Instruments (these instruments analyse data from the blood pressure cuff and the phonoarteriogram and the software helps plot graphs from the appropriate readings taken) were used. The equipment along with the associated Lab chart software was made available at the Electrophysiology Lab at Osmania Medical College, Hyderabad.
A subject was made to sit comfortably. Age and gender of the subject was noted. The mid arm circumference of the subject was measured using tape. The left brachial artery was located by palpation and the phonoarteriogram was placed on the site and was secured by a Velcro. The sphygmomanometer cuff was tied 2cm above the cubital fossa of the left arm. The blood pressure was recorded using the Lab Chart software. The Korotkoff sounds picked up and transmitted by the phonoarteriogram were represented as distinct lines on the graphical recording.
Since it was not possible to determine using the software, which two lines exactly correspond to the beginning and end of the Korotkoff sounds, the procedure was repeated using a stethoscope instead of the phonoarteriogram. Using the values of the systolic and diastolic blood pressures obtained by auscultation, the corresponding points were then marked on the graph [Table/Fig-1].
Recording of blood pressure (red) and Korotkoff sounds (blue) obtained using the Lab Tutor software. The black points mark the beginning and end of the Korotkoff sounds as recorded by auscultation.
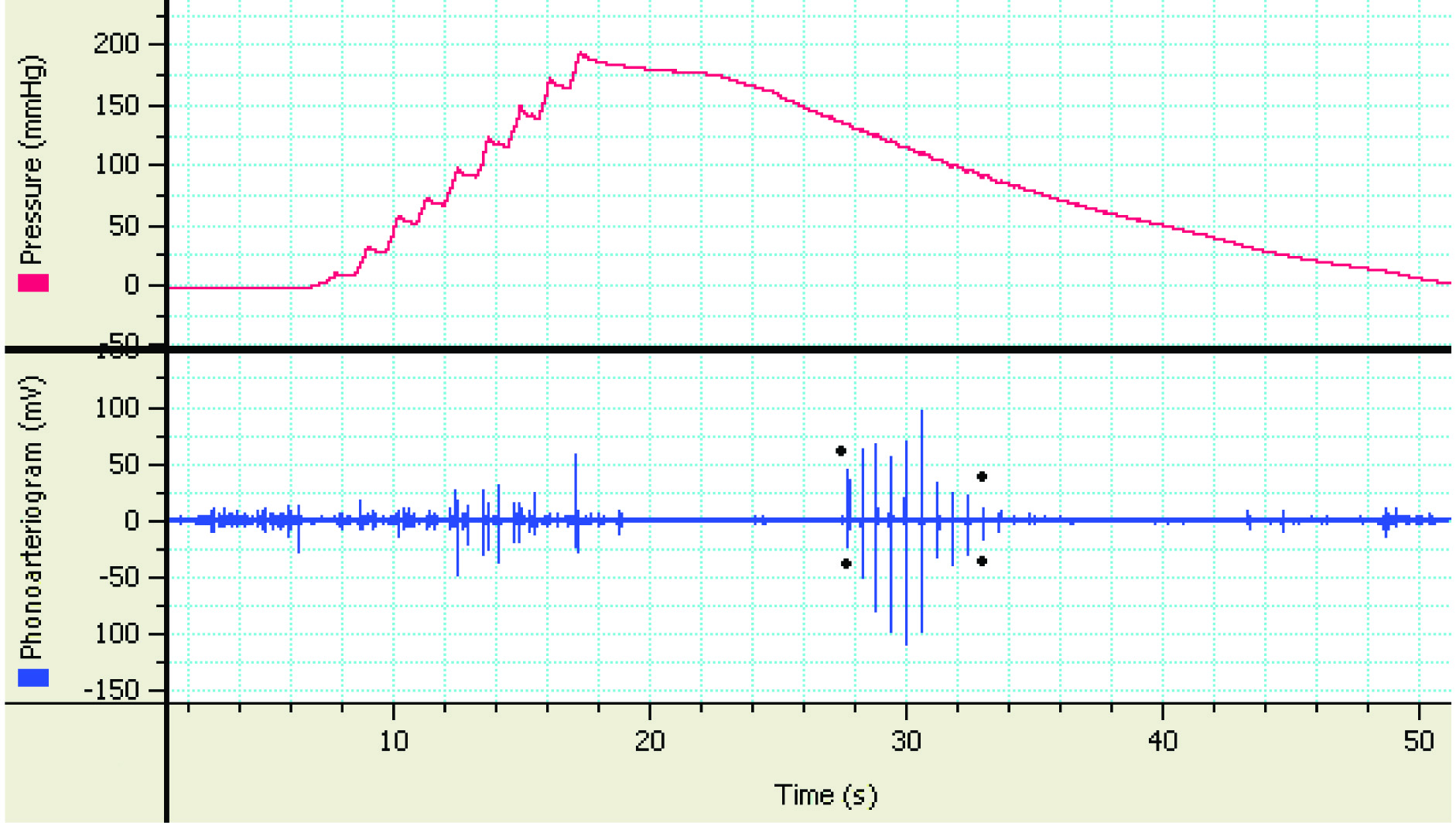
The length of each line in the recording was calculated in millimeters and the average of the length of all the lines was taken as the average amplitude of the Korotkoff sounds recorded for that subject. Although the scale on the y-axis showed the amplitude in millivolts (mV), the lengths were taken in millimeters (mm) for the ease of calculation and comparison.
Statistical Analysis
The mean values of the average amplitudes of the subjects of the following categories were obtained - young males, young females, old males, and old females. The mean values are compared for any significant differences using independent samples t-test. The unpaired samples t-test was done and correlational coefficient was calculated to look for significance in the variations in mean amplitudes in relation to variations in pulse pressures in the different age groups. Null hypothesis was eliminated at p<0.05. Data was analysed using the SPSS software version 20.0 (SPSS Inc.).
Results
There was a significant difference in the mean amplitudes of Korotkoff sounds among the different age groups and subject categories and by using the independent samples t-test, the significance of the difference in mean amplitudes for the different categories was analysed and the p-values obtained [Table/Fig-2,3]. A significant difference in pulse pressures was also seen among different age groups and subject categories. The decrease in the amplitudes of Korotkoff sounds in the older age group accompanies the increase in pulse pressures seen in this group [Table/Fig-4] and the same was seen among the different age groups within each sex [Table/Fig-5]. For correlating the variations in the pulse pressure with average amplitude in the different age groups among the sexes, the unpaired samples T-test was employed to calculate the correlation coefficient and the significance was determined by the p-value and a significant correlation was seen in both males [Table/Fig-6] and females [Table/Fig-7].
Table showing age distribution among the subjects in the study.
| Age Distribution among Young Subjects |
|---|
| Age(Years) | 15-16 | 17-18 | 19-20 | 21-22 | 23-25 |
|---|
| No. of Subjects | Male | 6 | 4 | 5 | 6 | 4 |
| Female | 4 | 4 | 6 | 5 | 6 |
| Age Distribution among Old Subjects |
| Age(Years) | 50-51 | 52-53 | 54-55 | 56-57 | 58-59 | 60-61 | 62-63 | 64-65 | 66-67 | 68-70 |
| No. of Subjecs | Male | 2 | 3 | 2 | 2 | 3 | 3 | 3 | 2 | 3 | 2 |
| Female | 3 | 3 | 3 | 2 | 3 | 2 | 2 | 3 | 2 | 2 |
Comparison between mean amplitudes (in mm) of the two age groups among males, females and overall (we can see that a relatively constant ratio between the mean amplitudes is being maintained among the two age groups).
| Amplitudes (mm) | Young | Old | Ratio of means | p-value |
|---|
| Males | 14.49±3.55 | 8.39±2.65 | 1.727 | 0.043 |
| Females | 6.28±2.46 | 3.65±1.46 | 1.722 | 0.037 |
| Overall | 10.39±5.13 | 6.02±3.20 | 1.726 | 0.001 |
Comparison of mean pulse pressures and mean amplitudes of the two age groups.
| Age | Group |
|---|
| Mean Pulse Pressure (mm Hg) | Mean Amplitude (mm) |
|---|
| Young | 44.72±3.42 | 10.39±5.13 |
| Old | 57.56±3.44 | 6.02±3.20 |
Comparison of mean pulse pressures and mean amplitudes of the different categories of subjects. The scatter plot shows four distinct groupings corresponding to the four categories of subjects. There is some degree of overlap between the two sexes within an age group.
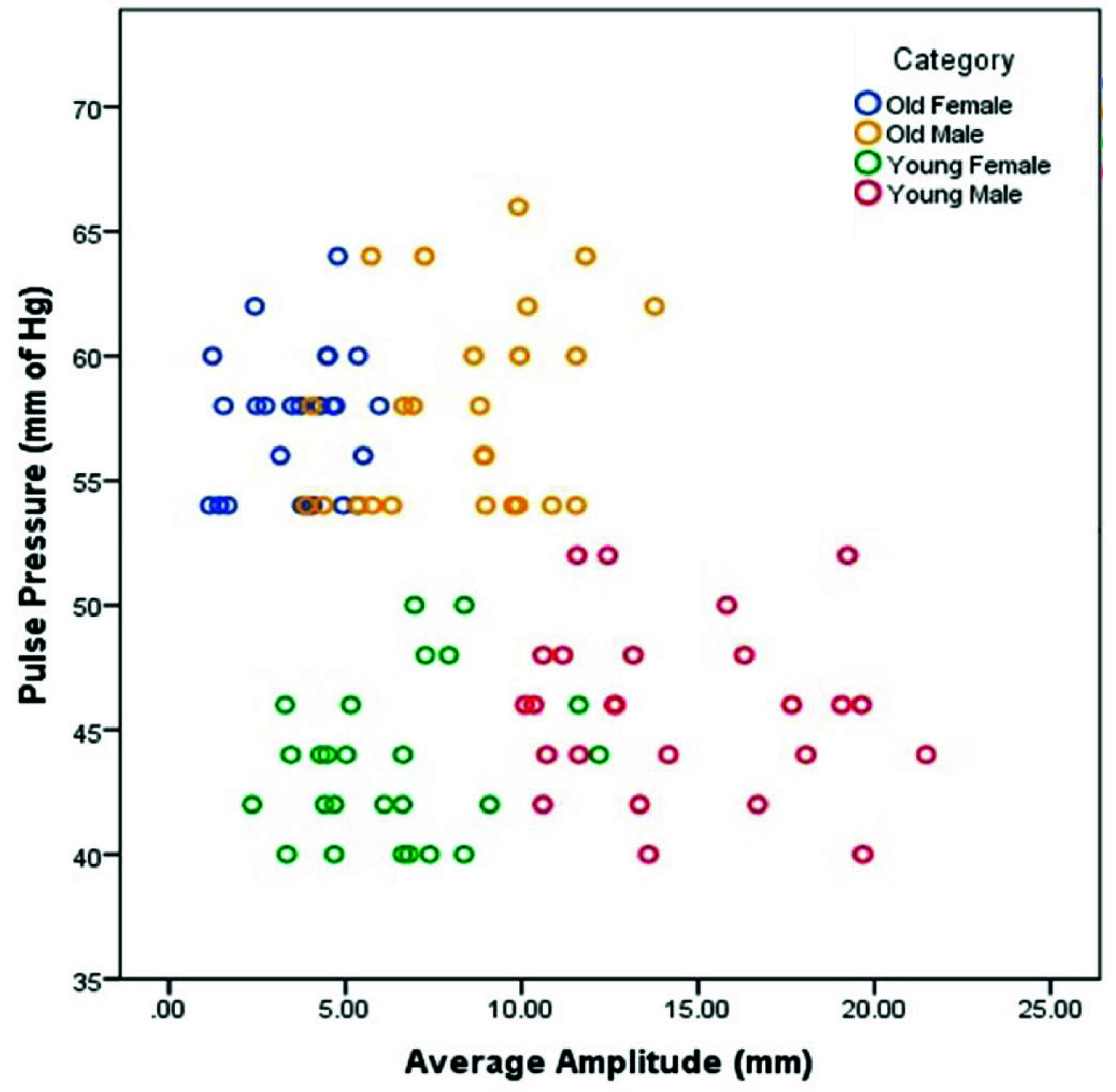 |
| Category | Mean Pulse Pressure (mm Hg) | Mean Amplitude (mm) |
| Young Male | 45.84±3.41 | 14.49±3.55 |
| Old Male | 57.84±4.00 | 8.39±2.65 |
| Young Female | 43.60±3.11 | 6.28±2.46 |
| Old Female | 57.28±2.82 | 3.65±1.46 |
Correlational significance between the pulse pressure and average amplitude of the old and young males.
| Category | Mean Pulse | Mean Amplitude | r-value | p-value |
|---|
| Pressure (mm Hg) | (mm) |
|---|
| Old Male | 45.84±3.41 | 14.49±3.55 | - 0.574 | 0.001 |
| Young Male | 57.84±4.00 | 8.39±2.65 |
Correlational significance between the pulse pressure and average amplitude of the old and young females.
| Category | Mean Pulse | Mean Amplitude | r-value | p-value |
|---|
| Pressure (mm Hg) | (mm) |
|---|
| Old Female | 43.60±3.11 | 6.28±2.46 | - 0.449 | 0.002 |
| Young Female | 57.28±2.82 | 3.65±1.46 |
Discussion
Korotkoff sounds have always been associated with the measurement of B.P. In a paper by Simon Rodbard, it was shown that the Korotkoff sounds varied in the case of reactive hyperaemia [1]. This shows that the Korotkoff sounds vary with the amount of blood flowing through the vessel. It was also shown that the sounds were produced due to the flutter of the arterial wall [1]. By using these findings, this study was taken up to see if the change in Korotkoff sounds holds good in conditions wherein the elasticity of the arterial wall differs.
The results of the study show that such a relationship can be drawn and that the amplitudes of the Korotkoff sounds do change with change in the vascular compliance. The study shows that in the older individuals, the mean amplitude is 6.02±3.20 mm, which is 4.37mm less than that of the younger individuals (p=0.001) who have an average amplitude of 10.39±5.13 mm. This occurs as a result of the phenomenon of arteriosclerosis which occurs in the ageing arterial wall [2]. Arteriosclerosis leads to a decrease in elasticity of the wall thus making it less compliant, and hence, being able to flutter less. Consequently, the amplitudes of the Korotkoff sounds should decrease which is shown by the results of the study.
As stated in studies by Dart AM et al., and Zieman SJ et al., the pulse pressure readings in the older individuals increase [4,5]. This is also due to the effect of arteriosclerosis of the vascular wall. As a result of the decreased vessel wall compliance the pulse wave velocity increases. This causes the pulse wave to rapidly rebound from the branching points in the artery and superpose earlier during systole resulting in systolic pressure augmentation. Hence, there is an increase in systolic blood pressure reading relative to the diastolic blood pressure reading resulting in an increase in pulse pressure. This is seen in the sample of subjects taken for the study wherein the values of mean systolic blood pressure, mean diastolic blood pressure and mean pulse pressure for old and young subjects are 130.52±9.35 mm Hg, 73.12±7.73 mm Hg, 57.56±3.44 mm Hg and 115.08±8.35 mm Hg, 70.32±7.50 mm Hg, 44.72±3.42 mm Hg respectively. When analysed for a correlation between the pulse pressure and average amplitude between the different age groups, in males, for the older individuals, the mean pulse pressure was higher by 12.00 mm Hg and the mean amplitude was lower by 6.10mm when compared to the younger individuals (r = -0.574, p = 0.001) and among females, for older individuals, the mean pulse pressure was higher by 13.68 mm Hg and the mean amplitude was lower by 2.63mm when compared to the younger individuals (r = -0.449, p = 0.002).
Both these observations - increase in pulse pressure and decrease in amplitude of Korotkoff sounds, seen in the older individuals are the result of decrease in vascular compliance with arterial ageing. Thus, the results obtained show that the amplitude of Korotkoff sounds does decrease as a result of decreased vascular compliance.
A noteworthy observation is the constant ratio between the amplitudes of young and old individuals (overall = 1.726, males = 1.727, females = 1.722). Since the amplitude is directly proportional to the vessel wall compliance, the factor of 1.72 may probably indicate how much more compliant the vessel wall is in a young individual compared to the older subjects. However, a study with a much larger sample size must be conducted to validate this hypothesis. It was also observed that there is a difference in the amplitude of the Korotkoff sounds between males and females of the same age group. This may be due to the differences in blood volume between the sexes [8]. The greater the blood volume, the more is the amount of blood flowing through the vessel, and hence, higher amplitude of Korotkoff sounds is observed [1]. The larger amplitude in males can also be attributed to more muscle mass which draws a greater amount of blood than compared to that of females [1].
The comparison between the amplitude of Korotkoff sounds and mid arm circumferences of the subjects could not be made effectively in this study. This is because the relative proportions of muscle and fat in the upper arm cannot be determined by the value of mid arm circumference alone. For such a study it will be necessary to take into account the derived parameters of the upper arm anthropometry like - mid upper arm area (MUAA), mid upper arm muscle area (MUAMA), mid upper arm fat area (MUAFA) and arm fat index (AFI) [9,10].
A study with a larger sample size can be taken up in order to standardize the values of the Korotkoff sounds amplitudes for healthy individuals in each category, namely - young males, young females, old males and old females.
In this study, since physiologically normal individuals were taken as subjects, a difference in amplitude of Korotkoff sounds was observed attributable to a naturally occurring change in vascular compliance. This could be extended to conditions wherein a change in vascular compliance is brought about by pathological alterations in the vascular wall as in atherosclerosis resulting from diabetes mellitus and hyperlipidaemia [11].
Further research can be done to see if this method can be used for following up the effect of drugs that affect either the amount of blood flowing through the artery as in anti-hypertensive vasodilator drugs [12] or drugs that affect the nature of the vessel wall as in anti-lipidaemic drugs [13,14].
If proven plausible, it can also be used to detect the severity of blood loss in conditions like cardiovascular shock and extensive burns [15] and it may also be used to follow up response to rehydration therapy [15,16] in such situations.
Conclusion
The amplitude of Korotkoff sounds gives us an idea of the nature of the arterial wall as shown by a decrease in amplitude in older individuals when compared to the younger individuals and of the volume of blood flowing through the artery as shown by the higher amplitudes observed in males when compared to females.
By standardizing the amplitude values for healthy individuals of different age groups in each gender by conducting larger studies, the values obtained in patients with cardiovascular diseases, metabolic dysfunctions and emergency situations can be compared with them to know the extent of decrease in circulating blood volume and vascular compliance.
Comparison can also be made between the standard reference values, the values obtained at admission to the hospital with a particular cardiovascular or metabolic complication and the values obtained after therapeutic intervention to effectively monitor the recovery of the patient.
Hence, measurement of amplitude of Korotkoff sounds can be used as a regular procedure for monitoring the cardiovascular status of patients admitted to the hospitals.
[1]. Rodbard S, The Significance of the Intermediate Korotkoff SoundsCirculation- Journal of the American Heart Association 1953 8:600-04. [Google Scholar]
[2]. O’Rourke MF, Arterial Ageing: Pathophysiological PrinciplesVasc Med 2007 12:329 [Google Scholar]
[3]. Drzewiecki G, Pilla JJ, Noninvasive Measurement of the Human Brachial Artery Pressure– Area Relation in Collapse and HypertensionAnnals of Biomedical Engineering 1998 26:965-74. [Google Scholar]
[4]. Dart AM, Kingwell BA, Pulse Pressure - A Review of Mechanisms and Clinical RelevanceJournal of the American College of Cardiology 2001 37(4):975-84.doi:10.1016/S0735- 1097(01)01108-11 [Google Scholar]
[5]. Zieman SJ, Melenovsky V, Kass DA, Mechanisms, Pathophysiology and Therapy of Arterial StiffnessArterioscler Thromb Vasc Biol 2005 25(5):932-43. [Google Scholar]
[6]. Mastropaolo JA, Stamler J, Berkson DM, Wessel HU, Jackson WE, Validity of Phonoarteriographic Blood Pressures During Rest and ExerciseJournal of Applied Physiology 1964 19:1219-33. [Google Scholar]
[7]. McDowell MA, Fryar CD, Ogden CL, Flegal KM, Anthropometric Reference Data for Children and Adults: United States, 2003 – 2006National Health Statistics Reports 2008 10 [Google Scholar]
[8]. Tarazi RC, Blood VolumeEuropean Heart Journal, Chapter 8 1985 [Google Scholar]
[9]. Grodner M, Long S, DeYoung S, Nutrition in Patient CareFoundations and clinical applications of nutrition: a nursing approach(3rd ed.)Elsevier Health Sciences:406-07. [Google Scholar]
[10]. Frisancho AR, Anthropometric standards for the assessment of growth and nutritional status17-18University of Michigan Press:20-23. [Google Scholar]
[11]. Creager MA, Lüscher TF, Diabetes and Vascular Disease: Pathophysiology, Clinical Consequences, and Medical Therapy: Part IJournal of the American Heart Association 2003 108:1527-32. [Google Scholar]
[12]. Nelson M, Drug Treatment of Elevated Blood PressureAustralian Prescriber 2010 33(4):108-12. [Google Scholar]
[13]. Bradford RH, Shear CL, Chremos AN, Expanded Clinical Evaluation of Lovastatin (EXCEL): efficacy in modifying plasma lipoproteins and adverse event profiles in patients with moderate hypercholesterolaemiaArch Intern. Med 1991 151(1):43-49. [Google Scholar]
[14]. Sever PS, Poulter NR, Dahlöf B, Reduction in cardiovascular events with atorvastatin in 2,532 patients with type 2 diabetes: Anglo- Scandinavian Cardiac Outcomes Trial—lipid-lowering arm (ASCOT-LLA)Diabetes Care 2005 28(5):1151-57. [Google Scholar]
[15]. Drozdz L, Madry R, Struzyna J, Burn shock, diagnostics, monitoring and fluid therapy, Wschodnie Centrum Leczenia Oparzei Chirurgii RekonstrukcyjnejWiad Lek 2011 64(4):288-93. [Google Scholar]
[16]. Cherkas D, Traumatic Haemorrhagic Shock: Advances in Fluid Management, Department of Emergency Medicine. Mount Sinai School of Medicine, Elmhurst Hospital CenterEmerg Med Pract 2011 13(11):1-19. [Google Scholar]