An Epidemiological Study of Malnutrition Among Under Five Children of Rural and Urban Haryana
Sachin Singh Yadav1, Shweta Tomar Yadav2, Prabhaker Mishra3, Anshu Mittal4, Randhir Kumar5, Jagjeet Singh6
1 Assistant Professor, Department of Community Medicine, M. M. Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
2 Associate Professor, Department of Obstetrics and Gynaecology, M. M. Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
3 Assistant Professor, Department of Biostatistics & Health Informatics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raebareli Road, Lucknow, UP, India.
4 Professor, Department of Community Medicine, M. M. Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
5 Assistant Professor, Department of Community Medicine, M. M. Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
6 Professor and Head, Department of Community Medicine, M. M. Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sachin Singh Yadav, E-12 MMU Residential Complex, Mullana, Ambala, Haryana, India.
E-mail: dr.sachin2015@rediffmail.com
Introduction
A child is future of nation. Malnutrition is a big public health problem in India as it can be attributed for more than half (54 percent) of all under five mortality in India.
Aim
To assess prevalence of malnutrition among urban and rural population of Haryana using newly developed WHO growth standards.
Settings and Design
A community based cross-sectional survey was conducted in children of 3-60 months age living in the urban and rural field practice areas of Department of Community Medicine MMIMSR, Mullana, Ambala during January 2012 to December 2012.
Materials and Methods
Seven hundred and fifty children, aged 3-60 months, were studied for nutritional status, socio-demographic measures were obtained from structured questionnaire and followed by anthropometric assessment using standards methods. Z score for Anthropometric data was calculated by WHO Anthro 2010 software (beta version).
Statistical Analysis
Descriptive statistics as well as simple proportion were calculated with SPSS 20.
Results
We found that 41.3% children were underweight and 14% were severe underweight. Female children were more nutritionally deprived than males. Among sociodemographic factors maternal educational and working status as well as SES class and rural background of family had greater impact on nutritional status of child.
Conclusion
We found that almost half of our under five children are underweight, girl child being affected more. For attainment of best possible nutrition and growth in children, targeted short-term strategies addressing underlying risk factors and more long-term poverty alleviation strategies may be needed.
Anthropometric assessment, Nutritional status, Underweight, WHO growth standards
Introduction
The health of children and youth is of fundamental importance. Without ensuring optimal child growth and development efforts to accelerate economic development significantly will be unsuccessful. Good nutrition is a basic requirement for good health [1].
Malnutrition is a silent emergency [2]. Malnutrition is both undernutrition and over nutrition ranging from severe nutrient deficiencies to extreme obesity [3]. Globally; more than one third of child deaths are attributable to under nutrition. Nutrition plays a key role in physical, mental and emotional development of children and much emphasis has been given to provide good nutrition to growing populations especially in the formative years of life [4].
Eighty percent of the world’s undernourished children live in 20 countries, with India being home to nearly 60 million children who are underweight [5]. At present in India 48% children < 5 years age are chronically malnourished and 43% are underweight (NFHS-3). More than half (54 percent) of all deaths before age five years in India are related to malnutrition. Because of its extensive prevalence in India, mild to moderate malnutrition contributes to more deaths (43 percent) than severe malnutrition (11 percent) [6]. Growth assessment best defines the health and nutritional status of children because disturbances in health and nutrition regardless of their aetiology invariably affect child growth and hence provide an indirect measurement of the quality of life of an entire population [7]
Anthropometric assessment is widely used and often regarded as the best single measure for health and nutritional status in children [8] Interpretation of the growth of a population is largely dependent on the growth reference standard used [9]. The World Health Organization (WHO) published the Child Growth Standard for infants and children up to the age of 5 year based on a multi-country study on growth of healthy breast-fed children under optimal conditions in April 2006 [10].
This study was an attempt to assess prevalence of malnutrition among urban and rural population of Haryana using newly developed WHO growth Standards.
Materials and Methods
A community based cross sectional study was conducted in children of 3 months to 60 months of age living in the urban and rural field practice areas of Department of Community Medicine MMIMSR, Mullana, Ambala, during January 2012 to December 2012. NFHS 3 reports a prevalence of malnutrition to be 39.6% among children under 5 years of age in Haryana. The sample size was calculated assuming a prevalence of 38% among under five children.
The equation used for calculating sample size is as follows:

Where, Z = level of confidence - 95% (1.96), P= Prevalence of the disease, e = margin of error.
Taking relative error as 10% of the prevalence, the sample size came out to be 652. Assuming non-response rate to be 10%, minimum target sample size is 717. Finally we have taken up 750 children for this study. Simple random sampling technique was used for sample collection. As per census 2001, the ratio of rural to urban population in district Ambala was 3:1. Thus 530 children have been taken from rural area and 220 from urban area. In the selected households all the children of age 3-60 months have been included in the study.
The data was collected on a self designed and semi-structured questionnaire. We conducted house to house survey and data was collected by interviewing the mothers or the primary care giver of the child after taking an informed and written consent. This was followed by anthropometric assessment using standards methods as described in training manual of WHO Growth Standards.
Statistical Analysis
The data collected during the survey have been entered in ms excel. Anthropometric data entered in WHO Anthro 2010 software (beta version) and Z scores for anthropometric measurements were computed for boys and girls separately by age groups. All the data were analysed in Statistical package for social sciences (SPSS) version 20 (IBM, Chicago, USA). Descriptive statistics as well as simple proportion were calculated for the data.
Results
Study population included 410 (54.7%) male and 340 (45.3%) female children. Majority of children (23.6%) belonged to 36-47 month age group. Mean age of males was 28.58± SD 16.88 month, while of females 28.95± SD 16.89months. [Table/Fig-1] shows socio demographic details of children.
Socio demographic details of children.
| Age in Months | Male | Female | Total |
|---|
| (3-5) | 33(8.1%) | 37(10.9%) | 70(9.3%) |
| (6-11) | 62(15.1%) | 29(8.5%) | 91(12.1%) |
| (12-23) | 54(13.2%) | 71(20.9%) | 125(16.7%) |
| (24-35) | 99(24.1%) | 45(13.2%) | 144(19.2%) |
| (36-47) | 77(18.8%) | 100(29.4%) | 177(23.6%) |
| (48-60) | 85(20.1%) | 58(17.1%) | 143(19.1%) |
| Age (Years) | Father | Mother | Total |
| 18-24 | 19 (2.5%) | 136 (18.1%) | 155(10.3%) |
| 25-35 | 642(85.7%) | 614 (81.9%) | 1256(83.8%) |
| >35 | 88(11.8%) | 0 | 88 (5.9%) |
| Education | Father | Mother | Total |
| Professional Degree | 59(7.9%) | 16(2.1%) | 75(5%) |
| Graduate and PG | 225(30%) | 81(10.8%) | 306(20.4%) |
| I.Sc./Post High School Diploma | 115(15.4%) | 103(13.7%) | 118(7.9%) |
| High School Certificate | 105(14 %) | 120(16%) | 225(15%) |
| Middle School Completion | 151(20.2%) | 183(24.4%) | 334(22.3%) |
| Primary School | 65(8.7%) | 127(16.9%) | 192(12.8%) |
| Illiterate | 29(3.9%) | 120(16%) | 149(9.9%) |
| Socioeconomic status | Male | Female | Total |
| I | 18(4.4%) | 14(4.1%) | 32(4.3%) |
| II | 46(11.2%) | 40(11.8%) | 86(11.4%) |
| III | 78(19%) | 63(18.5%) | 141(18.8) |
| IV | 168(41%) | 146(42.9%) | 314(41.9%) |
| V | 100(24.4%) | 77(22.6%) | 177(23.6%) |
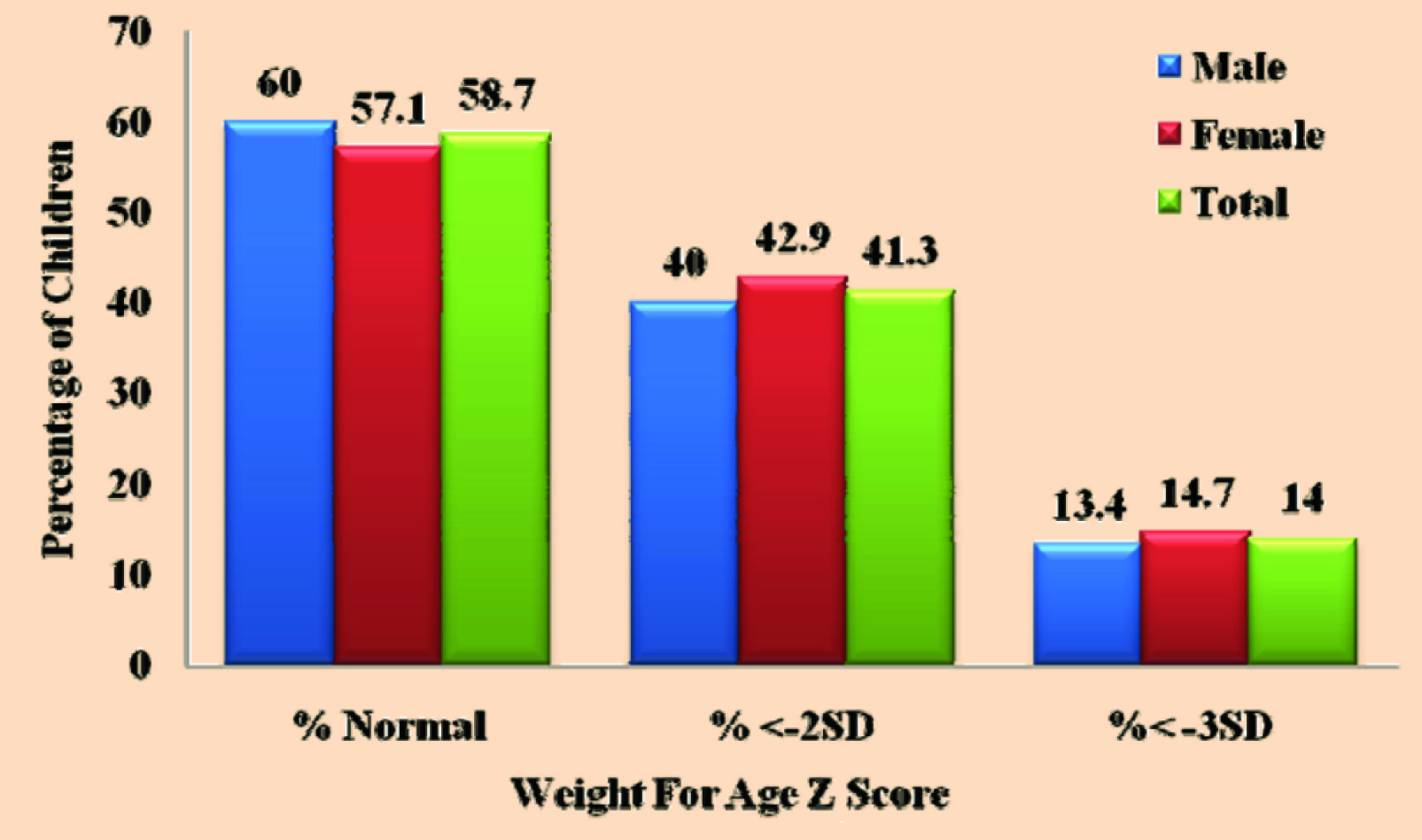
All children having weight for age Z score (WAZ) above – 2 SD were classified as normal, those with WAZ score < -2SD as underweight, and with WAZ score <-3 SD as severe underweight. Number of cases <-2 SD includes cases with <-3SD. In our study we found that out of 750 children 310 (41.3%) were underweight (WAZ < -2 SD) and 105(14%) were severe underweight (WAZ < -3 SD). Highest prevalence of underweight & severe underweight was found in 12-23 month age group. [Table/Fig-2] illustrates the prevalence of underweight in different age groups. Prevalence of underweight was higher in females compared to male children (42.9% Vs 40%, p value = 0.417) respectively. The prevalence of severe underweight among males and females were 13.4% and 14.7% respectively [Table/Fig-3]. We found that 44% of rural and 35% urban children were underweight and severe underweight was seen in 15.7% rural and 10% urban participants.
Age wise distribution of children according to weight for age.
| Age groups | N(%) normal | N(%)< - 2 SD | N(%) < - 3 SD |
|---|
| (0-5) | 49(70%) | 21(30%) | 7(10%) |
| (6-11) | 51(56%) | 40(44%) | 14(15.4%) |
| (12-23) | 68(54.4%) | 57(45.6%) | 20(16%) |
| (24-35) | 84(58.3%) | 60(41.7%) | 20(13.9%) |
| (36-47) | 97(54.8%) | 80(45.2%) | 26(14.7%) |
| (48-60) | 91(63.6%) | 52(36.4%) | 18(12.6%) |
| Total (%) | 440(58.7%) | 310 (41.3%) | 105(14%) |
Sex wise distribution of children as per weight for age.
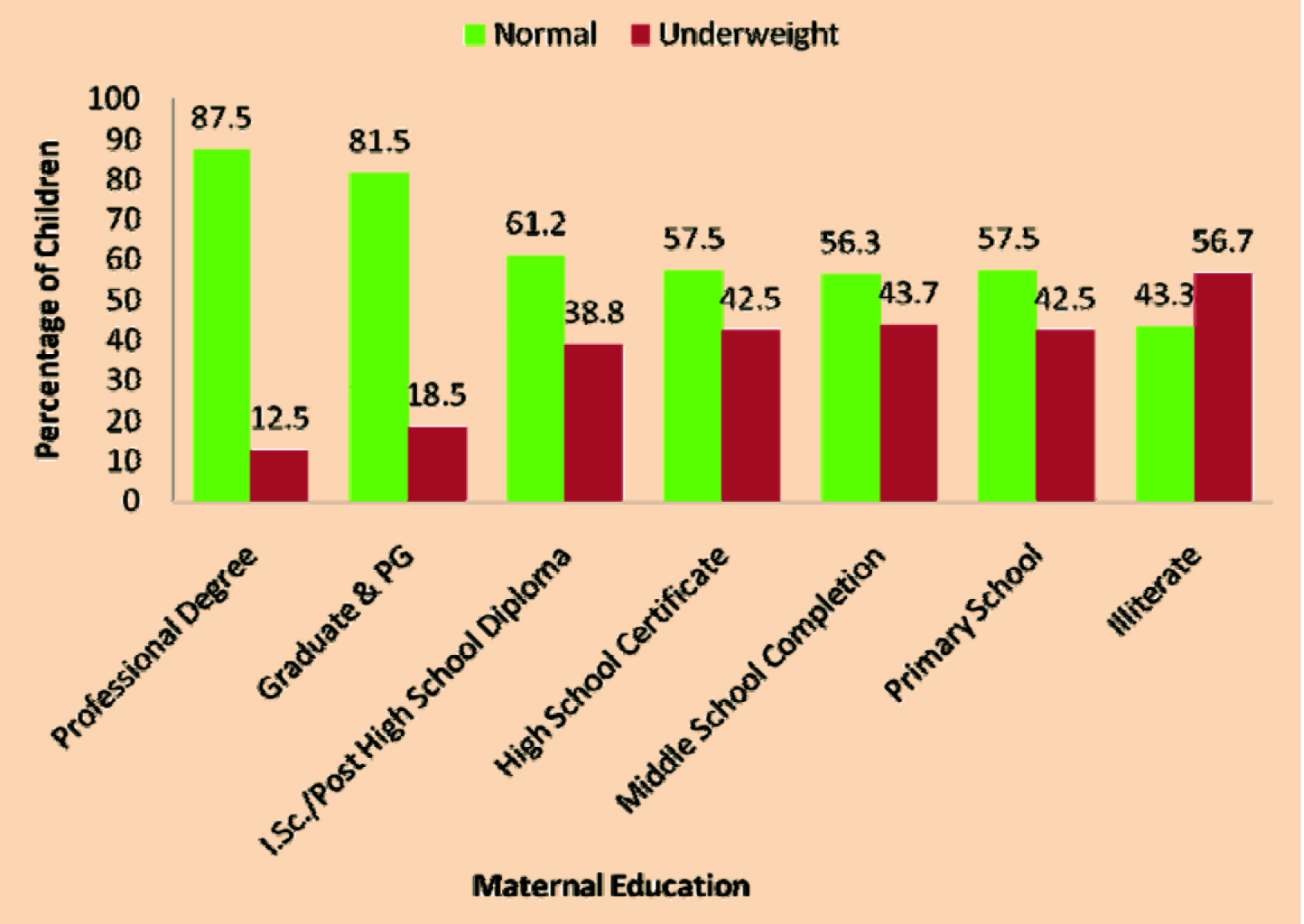
[Table/Fig-4] explains effect of maternal educational status on child’s nutritional status. We observed a declining trend of malnutrition with increase in educational qualification of the mothers. Less than half of the children (43.3%) of the illiterate mothers were having normal weight for age Z score. This observed difference was statistically highly significant (p=0.0001) while father’s educational status had less marked effect on child’s nutritional status. When mother is unemployed underweight prevalence was similar to total study population but if she is employed underweight and severe underweight prevalence was elevated (p=0. 002). On the contrary father’s occupation had modest effect on underweight prevalence (p= 0.135). We found that statistically highly significant (p=0.0001) number of children were underweight in lower socioeconomic status (52.5 and 55.4% respectively in class IV and V).
Association of maternal education with nutritional status of children.
Discussion
Our study revealed that overall 41.3 % children under 60 months age were underweight and14 % were severe underweight. As per the NFHS 3 report, 43% of children below 5 years of age are underweight and 16% are severe underweight [6], while Ramchandran P et al., analysed the NFHS 3 data on new WHO standards and found 42.5% underweight prevalence [10]. [Table/Fig-5] depicts underweight prevalence reported by various researchers [11–18]. In our study underweight prevalence was higher in females compared to male children 42.9% and 40% respectively. Prevalence of severe underweight was 13.4% and 14.7% in males and females respectively, similar results were obtained by William R F et al., [19] on the contrary Ahmed et al., in his study demonstrated that female children had 20% to 21% less odds of being underweight than the male counterparts [20].
Studies on prevalence of malnutrition among under-five children in India
| Sr.No | Name of study | Study population andplace | UnderweightPrevalence | Prevalence ofsevereUnderweight |
|---|
| 1 | Current study | 750 under 5 children of from rural and urban Ambala | 41.3% | 14% |
| 2 | GS Boregowda et al., (2015) [11] | 602 toddlers from slums of Raipur | 45.2 | 11.8 |
| 3 | Stanly AM (2015) [12] | 385 under 5 children of rural area | 42.9% | 5% |
| 4 | Philip, et al., (2015) [13] | 438 tribal preschool children in 10 clusters of Wayanad district of Kerala | 39% | 8.2% |
| 5 | Srinivas Chakravarthy Bhimisetti et al., (2015) [14] | 236 under 5 children of tribal areas of Visakhapatnam | 60.2% | 12.7% |
| 6 | Agrawal D et al.,(2015) [15] | 458 under 5 children residing in Agra city | 42.8% | |
| 7 | Mane, et al., (2015) [16] | 210 preschool children aged 1-3 years of Bhadravatitaluk of Shivamogga district | 29.5% | 8.6% |
| 8 | Davey S et al., (2014) [17] | 450 children between the age group 0-5 years of Delhi slums | 57.8%. | |
| 9 | Dasgupta A et al., (2014) [18] | 113 under-five children of Nasibpur Union Health Centre | 17.7% | |
Among rural children overall prevalence of underweight was found to be 44%, while of severe underweight was 15.7%, similar results were obtained by 53 [21] urban children were privileged that only 35% children were underweight and 10% were found to be severe underweight, our findings are similar to earlier reported from slum children of Delhi by Bhadoria AS [22], while Narkhede V et al., [23] report higher (52.23%) prevalence among Nagpur children. while NFHS 3 reported that undernutrition is substantially higher in rural areas than in urban areas [6].
In present study, underweight was influenced by mother’s education status (p=0.0001) with increased prevalence of all forms of under nutrition among children of illiterate mothers. As observed in NFHS 3 report undernutrition has a strong negative relationship with the mother’s education. The percentage of children who are severely underweight is almost five times as high for children whose mothers have no education as for children whose mothers have 12 or more years of education [6]. According Menezes RCE et al., maternal schooling has been pointed out as a factor associated with child growth [24]. In our study effect of father’s education on child’s malnutrition status effect is not that much marked as that of maternal educational effect (p=0.007). According to Rijal P et al., education of mothers and fathers has significant effect on the nutritional status of their children [25]. Here, 41.6% mothers and 32.2% fathers were illiterate out of which 53.9% and 40.6% children had malnutrition. Similar to earlier study we observed that if mother is unemployed underweight prevalence was similar to total study population but when she is employed underweight and severe underweight prevalence was elevated (p=0. 002) [26]. On the contrary father’s occupation had modest effect on underweight prevalence (p= 0.135).
We found that statistically highly significant (p=0.0001) number of children were underweight in lower socioeconomic status (52.5 and 55.4% respectively in class IV andV). Our results are comparable to previous studies [27–29].
Limitations
This study being a cross-sectional study cannot establish case and effect relationship between various socio-environmental factors and malnutrition. A follow-up study design is much better to assess the nutritional status of the children. Recall bias, and effect of both environmental and genetic factors is expected to have been obscured.
Conclusion
Although there is declining tendency of under-nutrition in the last years, yet malnutrition in preschool children ought to be considered as a community crisis. We found that almost half of our under five children are underweight, girl child being affected more. Malnutrition was more prevalent among children from rural families and from lower socioeconomic status. Maternal education and occupational status had significant effect on child’s nutritional status. To diminish the load of malnutrition in the children, a collective attempt by the government, non-governmental organizations and the community is crucial. Effective, efficient and equitable program should be designed to reduce child malnutrition. Indian government is having Integrated Child Development Services (ICDS), which At the national levels having high coverage, but utilization of ICDS services is low., For attainment of best possible nutrition and growth in children, targeted short-term strategies addressing underlying risk factors and more long-term poverty alleviation strategies may be needed.
[1]. Hasan I, Zulkifle M, Ansari AM, An assessment of nutritional status of the children of government urdu higher primary schools of Azad Nagar and its surrounding areas of BangaloreArch Appl Sci Res 2011 3(3):167-76. [Google Scholar]
[2]. Pulfrey S, Malnutrition a silent emergencyCMAJ 2006 174(13):1837 [Google Scholar]
[3]. Kandala NB, Madungu TP, Emina JBO, Nazita KPD, Cappuccio FP, Malnutrition among children under the age of five in the Democratic Republic of Congo (DRC): does geographic location matter?BMC Public Health 2011 11:261 [Google Scholar]
[4]. Kumar A, Kamath VG, Kamath A, Rao CR, Pattanshetty S, Sagir A, Nutritional status assessment of under-five beneficiaries of Integrated Child Development Services program in rural KarnatakaAMJ 2010 3(8):495-98. [Google Scholar]
[5]. Bryce J, Coitinho D, Darnton H, Pinsturp I, Anderson P, Maternal and child undernutrition, effective action at national levelLancet 2008 371:510-26. [Google Scholar]
[6]. Fred A, Parasuraman S, Parokiasamy P, Kothari M. Nutrition in India. National Family Health Survey(NFHS-3) India, 2005-06. Mumbai: International Institute For Population Sciences; Calverton Maryland, USA: ICF Macro [Google Scholar]
[7]. De Onis M, Monteiro C, Akre J, Clugston G, The worldwide magnitude of protein- energy malnutrition: an overview from the WHO Global Database on child growthBull World Health Organ 1993 71:703-12. [Google Scholar]
[8]. De Onis M, Measuring nutritional status in relation to mortalityBulletin of the WHO 2000 78(10):1271-74. [Google Scholar]
[9]. Nuruddin R, Lim MK, Hadden WC, Azam I, Comparison of estimates of under-nutrition for pre-school rural Pakistani children based on the WHO standard and the National Center for Health Statistics (NCHS) referencePublic Health Nutrition 2008 12(5):716-22. [Google Scholar]
[10]. Ramchandran P, Gopalan HS, Assessment of nutritional status in Indian preschool children using WHO 2006 Growth StandardsIndian J Med Res 2011 134:47-53. [Google Scholar]
[11]. Boregowda GS, Soni GP, Jain K, Agrawal S, Assessment of Under Nutrition Using Composite Index of Anthropometric Failure (CIAF) amongst Toddlers Residing in Urban Slums of Raipur City, Chhattisgarh, IndiaJournal of Clinical and Diagnostic Research 2015 9(7):LC04-06. [Google Scholar]
[12]. Stanly AM, Samya V, Prevalence of Undernutrition Among Under 5 Children in A Rural AreaIndian Journal of Applied Research 2015 10(5):207-09. [Google Scholar]
[13]. Philip RR, Vijayakumar K, Indu PS, Shrinivasa BM, Sreelal TP, Balaji J, Prevalence of undernutrition among tribal preschool children in Wayanad district of KeralaInt J Adv Med Health Res 2015 2:33-38. [Google Scholar]
[14]. Bhimisetti SC, Pamarthi K, Srinivas PJ, Nutritional Status of Under 5 Children Belonging to tribal Population Living in Visakhapatnam District, Andhra PradeshJournal of Evidence based Medicine and Healthcare 2015 2(33):4975-80. [Google Scholar]
[15]. Agarwal D, Misra SK, Chaudhary SS, Prakash G, Are we underestimating the real burden of malnutrition? An experience from community-based studyIndian J Community Med 2015 40:268-72. [Google Scholar]
[16]. Mane V, Naik TB, Mallappa O, Ambure O, Protein Energy Malnutrition among Preschool Children: A Cross Sectional StudyInt J Sci Stud 2015 3(2):109-13. [Google Scholar]
[17]. Davey S, Davey A, Adhish SV, Bagga R, Factors influencing status of undernutrition among children (0-5 years) in a rural area of Delhi; a cross sectional studyInt J Community Med Public Health 2014 1(1):12-17. [Google Scholar]
[18]. Dasgupta A, Parthasarthi R, Prabhakar RV, Biswas R, Geetanjali A, Assessment of Under nutrition with Composite index of anthropometric failure among under 5 children in rural area of West BengalIndian Journal of Community Health 2014 26(2) [Google Scholar]
[19]. William RF, Bijou J, Ali M, Velan V, Nutritional Assessment of Children in the 3 –5 Years of Age Group in Karaikal District, PudhucherryNat J Res Com Med 2012 1(2):61-65. [Google Scholar]
[20]. Ahmed AMS, Ahmed T, Roy SK, Alam N, Hossain MDI, Determinants of Under Nutrition in Children under 2 years of age from Rural BangladeshIndian Pediatr e-pub 2012 10 [Google Scholar]
[21]. Singh MB, Lakshminarayana J, Fotedar R, Anand PK, Childhood illnesses and malnutrition in under five children in drought affected desert area of western Rajasthan, IndiaJ Commun Dis 2006 38(1):88-96. [Google Scholar]
[22]. Bhadoria AS, Sareen N, Kapil U, Prevalence of underweight, stunting and wasting among children in urban slums of DelhiInt J Nutri Phramacol Neurol Dis 2013 3:323-24. [Google Scholar]
[23]. Narkhede V, Likhar S, Pitale S, Durge P, Nutritional status and dietary pattern of underfive children in urban slum areaNJCM 2011 2(1):143-8. [Google Scholar]
[24]. Menezes REC, Lira PC, Leal V, Oliveria JS, Determinants of stunting in children under five in Pernambuco, Northeastern BrazilRev Saúde Pública 2011 45(6):1079-87. [Google Scholar]
[25]. Rijal P, Sharma A, Shrestha S, Upadhyay S, Nutritional assessment of children at Nepal Medical College Teaching HospitalHealth Renaissance 2011 9(3):184-88. [Google Scholar]
[26]. Olatidoye OP, Effect of maternal employment on nutritional status of pre-school children from low income households area of oyo stateEJEAFCh 2011 10(7):2574-80. [Google Scholar]
[27]. Siddiqi M, Haque M, Goni M, Malnutrition of Under-Five Children: Evidence from BangladeshAsian J of Medical Sciences 2011 2:113-9. [Google Scholar]
[28]. Sengupta P, Philip N, Benjamin AI, Epidemiological correlates of under-nutrition in under-5 years children in an urban slum of LudhianaHealth and Population: Perspectives and Issues 2010 33(1):1-9. [Google Scholar]
[29]. Ruwali D, Nutritional Status of Children Under Five Years of Age and Factors Associated in Padampur VDC, ChitwanHealth Prospect 2011 10:14-8. [Google Scholar]