A Rare Association of Bilateral and Unilateral Masseter Hypertrophy with Hypertrophy of Pterygoids
Vijaya Kamble1, Kajal Mitra2
1 Associate Professor, Department of Radiodiagnosis, NKPSIMS and Research Centre, Nagpur, India.
2 Professor, Department of Radiodiagnosis, NKPSIMS and Research Centre, Nagpur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vijaya Kamble, Associate Professor, Department of Radiodiagnosis . NKPSIMS and Research Centre, Nagpur-440019, India.
E-mail: vijayashelkar@gmail.com
Computed tomography, Masseter muscle, Magnetic resonance imaging
Case 1
A 20-year-old female patient visited department of maxillofacial surgery with the chief complaints of swelling on either side of the face since 4 years [Table/Fig-1]. The swelling increased gradually in this time period and was first noticed by her relatives. It was non-tender and not associated with pain on jaw movements. She did not give any history of oral habits like tobacco chewing or betal leaf chewing. However, there was history of psychosocial depression. On extra oral examination, mild facial asymmetry was noticed on either side of jaw, measuring size of 5.5 x 6.5 cm in right side and 4.5 x 5.5 cm on left side. Prominence of swelling was noted on clenching of teeth. On intraoral examination, no abnormality was detected. The opening and closing of the jaws were normal. There was no history of facial trauma, dental abnormalities or temporomandibular joint clicking. Based on above clinical features provisional diagnosis of bilateral masseter hypertrophy was given.
Frontal view showing bilateral mandibular angle prominence.

Magnetic Resonance Imaging was performed using 1.5 Tesla GE scanner. MRI revealed enlargement of both masseter muscles, bilateral medial and lateral pterygoids [Table/Fig-2,3]. Bilateral temporal muscles also appeared to be enlarged. All these enlarged muscles were of the same signal intensity as that of the adjacent paraspinal muscles. The muscles were measured in transverse dimension at their maximum transverse bulge. Right masseter measured approximately 21.9mm and left masseter measured approximately 21.3mm. No obvious focal lesion was demonstrated in either of these muscles. Computed Tomography scan was performed using Toshiba 16 slice CT scanner to know bony details. CT study revealed subtle bony spurs on both sides, of right side being more prominent than left side [Table/Fig-4].
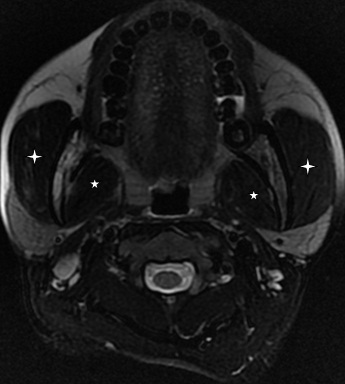
MRI axial T2WI, showing enlargement of masseters (4-point star) and medial pterygoid muscles (5-point star) on both sides.
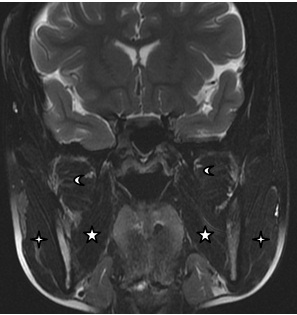
MRI Coronal T2WI, reveals hypertrophied masseters (4- point star), medial pterygoids(5- point star) and superior and inferior heads of lateral pterygoids (moon) on both sides.
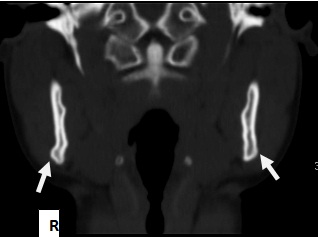
CT scan bone window coronal view, shows small bony spurs on both sides, right is more prominent than left (arrows).
Case 2
A 17-year-old female patient visited OPD of our college and hospital with chief complains of swelling on right side of lower third of face since two years [Table/Fig-5]. She noted that the swelling gradually increased. It was painless swelling and not associated with jaw movements. She did not give any history of tobacco, betal leaf or bubble gum chewing. She gave history of academic stress. On extraoral examination, mild facial asymmetry was noticed on right side of lower third of face due to swelling on mandibular angle region. The swelling was 3.5 x 4.0 cm in size with diffuse borders. On palpation, swelling was non tender, soft in consistency, compressible and fixed to the underlying tissues. Based on above clinical findings, a provisional diagnosis of unilateral masseter hypertrophy on the right side was given.
Frontal view showing unilateral right sided mandibular angle prominence.

A MRI study was done which showed increase muscle thickness of right sided masseter, medial pterygoid as well as lateral pterygoid muscles [Table/Fig-6,7]. Right masseter measured approximately 18.1 mm in its maximum transverse dimension. Bilateral temporalis muscles was not hypertrophied. A CT scan were also taken which showed prominence of mandibular angle on right side with mild expansion of the underlying bone [Table/Fig-8]. A final diagnosis of unilateral masseter hypertrophy with associated pterygoid muscle hypertrophy on right side was given.
MRI axial T2WI, showing enlargement of masseter (4-point star)and medial pterygoid(5-point star) in right side.

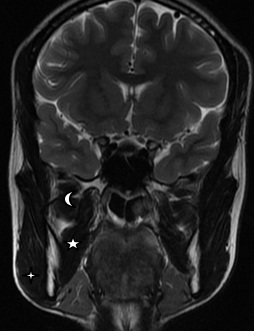
MRI Coronal T2WI, reveals hypertrophied masseter (4- point star), medial pterygoid (5- point star) and superior and inferior head of lateral pterygoid (moon) on right side.
CT scan bone window axial view, shows prominence of right mandibular angle with mild expansion of underlying bone(arrow).

A written informed consent was obtained from both the patients, for disclosure of photographs, MRI and CT scan for scientific purpose.
Both these patients were informed of the benign nature of their conditions respectively. The option of botulinum toxin injection was offered to both the patients. But they did not take the treatment. Both the cases reported were not associated with any causative factors for hypertrophy of masseter. So they were included under idiopathic masseter muscle hypertrophy.
Hypertrophy of the masseters was first described by Legg in 1880 [1]. Idiopathic masseter muscle hypertrophy is relatively rare disorder which manifests in adolescence and early adulthood. People of Asian descent are more frequently involved [2]. Around 140 cases of masseter hypertrophy are reported in the literature since the first described. A study by Riefkohl et al., showed that of the total 90 patients 4% were less than 10-year-old, 3% were over 40 and remaining patients had a mean age of 30 years [3]. Fifty seven percent of the patients were male and 43% were female. Our both patients were females and presented in early adulthood.
The aetiology of idiopathic masseter muscle hypertrophy has been attributed to a number of factors such as emotional stress, chronic bruxism, masseteric hyperfunction and microtrauma. The most common of these, bruxism is associated with psychosocial stress, anxiety, malocclusion and sleep disorders [4]. Our first patient complained of psychosocial depression and second patient complained of psychosocial stress due to academic pressure. So the aetiology in both of our cases can be attributed to emotional stress.
Change in the facial appearance is the most frequent complaint of patients. Clinical diagnosis of masseter hypertrophy could be difficult in unilateral cases and we have to consider differential diagnosis of local infective, inflammatory lesion, vascular tumour, benign and malignant muscle tumours.
Clinical diagnosis of masseter hypertrophy is not possible and various modalities like CT, MRI and ultrasonogram are used to confirm muscle hypertrophy [5]. Very few cases of concurrent occurrence of hypertrophy of medial pterygoids and temporalis muscles has been reported [6,7]. In both our cases, MRI study revealed hypertrophy of medial pterygoids as well lateral pterygoids and masseter muscle. Temporalis muscle hypertrophy was noted in case of bilateral masseter hypertrophy.
In both our cases, MRI has clearly demonstrated the soft tissue features and CT has demonstrated the bony features. Along with masseter hypertrophy MRI and CT also demonstrated medial pterygoid, lateral pterygoid and temporalis hypertrophy, which complemented our diagnosis, thus obviating the need for further invasive investigations.
Bone spurs at the mandibular angles and mandibular angle prominence can be observed in CT study [Table/Fig-4,8] of these cases. Guggenheim and Cohen [8] reported that bone spurs are caused by periosteal irritation and new bone deposition responding to increased forces exerted by the muscle bundles.
Masseter hypertrophy treatment include reassurance, tranquilizers and injection of very small doses of botulinum toxin type A. Surgical treatment include dental restoration, occlusal adjustments, reduction and restoration of prominent mandibular angle. In our cases, counselling was done and option of botulinum toxin injection was offered. Both patients were not ready for surgical treatment.
[1]. Legg JW, Enlargement of the temporal and masseter muscles on both sidesTrans Pathol Soc London 1880 3:361-66. [Google Scholar]
[2]. Whitakar LA, Prominent mandiular angle -preoperative management, operative technique and results in 42 patients (Discussion)Plastic Reconstruction Surgery 1989 83:279 [Google Scholar]
[3]. Riefkohl R, Georgiade GS, Georgiade NG, Masseter muscle hypertrophyAnn Plast Surg 1984 12:528-32. [Google Scholar]
[4]. Balatsouras D, Kaberos A, Psaltakos E, Economou N, Bruxism: two case reportsActa Otorhinolaryngol Ital 2004 24:165-70. [Google Scholar]
[5]. Sannomiya EK, Goncalves M, Cavalcanti MP, Masseter Muscle Hypertrophy-Case ReportBraz Dent J 2006 17(4):347-50. [Google Scholar]
[6]. Guruprasad R, Rishi S, Nair PP, Thomas S, Masseter and medial pterygoid muscle hypertrophyBMJ Case Reports 2011 10.1136/bcr.07.2011.4557 [Google Scholar]
[7]. Andreadis D, Stylianou F, Tsatsouli IL, Markopoulos A, Bilateral muscle and internal pterygoid muscle hypertrophy: A diagnostic challengeMedical principles and Practise 2014 23:286-88. [Google Scholar]
[8]. Guggenheim P, Cohen L, Masseteric hypertrophyArch Otolaryngol 1959 70:674-80. [Google Scholar]