Sickle cell disease (SCD) is a monogenetic disorder caused by point mutation (GAG→GTG) in the beta globin gene (11p15.5) leading to replacement of polar glutamic acid with a hydrophobic valine at sixth position in beta globin chain of haemoglobin molecule [1]. In SCD patients the mutated beta globin chains combine with alpha globin chains to form sickle haemoglobin (HbS). Under hypoxic conditions, HbS gets aggregated/polymerized through hydrophobic interactions to form rope like fibrous structure [2]. Because of these fibrous aggregates/polymers, the shape of erythrocytes is deformed to sickle shape. Initially this process is reversible with oxygenation, but with repeated sickling, cell membrane of erythrocytes gets damaged and their elasticity is reduced [3]. Such erythrocytes fail to return to their normal shape, even under normal oxygen tension. SCD is prevalent in central India, especially state of Chhattisgarh and is a significant cause of morbidity. SCD allele is present in about ten percent population of state, i.e., about 25 lac people. Out of these persons, about two lac fifty thousand persons are estimated to be homozygous for disease allele and are suffering from SCD [4].
Although it is a monogenetic Mendelian trait, its phenotype is pleiotropic i.e., it differs among the affected individuals in terms of symptoms and severity of clinical course [5]. Mechanisms of SCD phenotype include three fundamental pathological processes: vaso-occlusion, sickling of erythrocytes and susceptibility to infections. Ultimately it leads to multi-organ failure and death of patient at an early age. Vaso-occlusive crisis is major cause of morbidity, but its frequency and severity differ from patient to patient [6]. Transmission of this disorder into future generation can be prevented by early detection, counseling and education, thereby preventing birth of children affected with SCD [7].
Electronic medical record (EMR) systems are well known to improve the standard of patient care in different sectors [8]. Considering the variability of patients’ presentation, an indigenously developed EMR system has been implemented. EMR system was developed by Bioinformatics Centre, Department of Biochemistry, Pt. Jawaharlal Nehru Memorial Medical College, Raipur and Department of Bioinformatics and Biostatistics, Sickle Cell Institute Chhattisgarh, Raipur, India. Both of these are institutions of Government of Chhattisgarh. EMR implementation has been done in two phases, considering the requirement at the institute. As Department of Biochemistry, Pt. J.N.M. Medical College is running a state wide sickle cell screening program with financial support of Government of Chhattisgarh since year 2007, the data generated are huge [4]. Thus, first phase of EMR development and implementation was aimed to store and manage the data generated through state wide sickle cell screening program and is referred as ‘State Wide Screening Data Interface’ (SWSDI). Further, in the next phase, EMR system was extended to store and manage data of persons, who have been screened as SCD patients during the screening, and visit OPD of the institute to avail the treatment, counseling and other facilities available. This phase of medical informatics solution has been referred as ‘Sickle Cell Patients Temporal Data Management System’ (SCPTDMS). The ultimate objective behind present study was to develop and implement a cost-effective EMR system indigenously, using informatics techniques to improve the health care services provided to SCD patients in Chhattisgarh. Thus, EMR systems were developed to store and manage the huge data being generated through state wide screening for SCD and clinical data for SCD patients attending the outpatient department (OPD) of Sickle Cell Institute Chhattisgarh, Raipur.
Materials and Methods
Collection of Data through Screening Program
In state wide sickle cell screening program in Chhattisgarh, after getting informed consent, school going children are being screened through haemoglobin solubility test to identify presence of sickle haemoglobin. For children found positive for haemoglobin solubility test, blood samples are sent to a central laboratory at the institute for haemoglobin electrophoresis test to identify genotype status i.e., sickle cell carrier (AS) and sickle cell disease patient (SS). Till June 2015, 1299003 individuals have been screened for SCD in nine districts of the state viz., Durg, Kawardha, Mahasamund, Raipur, Bemetara, Baloda Bazar, Balod, Mungeli and Gariyaband. In addition special camps for screening SCD patients were organized in five districts viz., Dhamtari, Korba, Dantewada, Jashpur, Bilaspur and 6354 individuals were screened for SCD. Thus screening program generates huge amount of data that must be stored and managed in an efficient manner for ready reference [4].
Development and Implementation of SWSDI
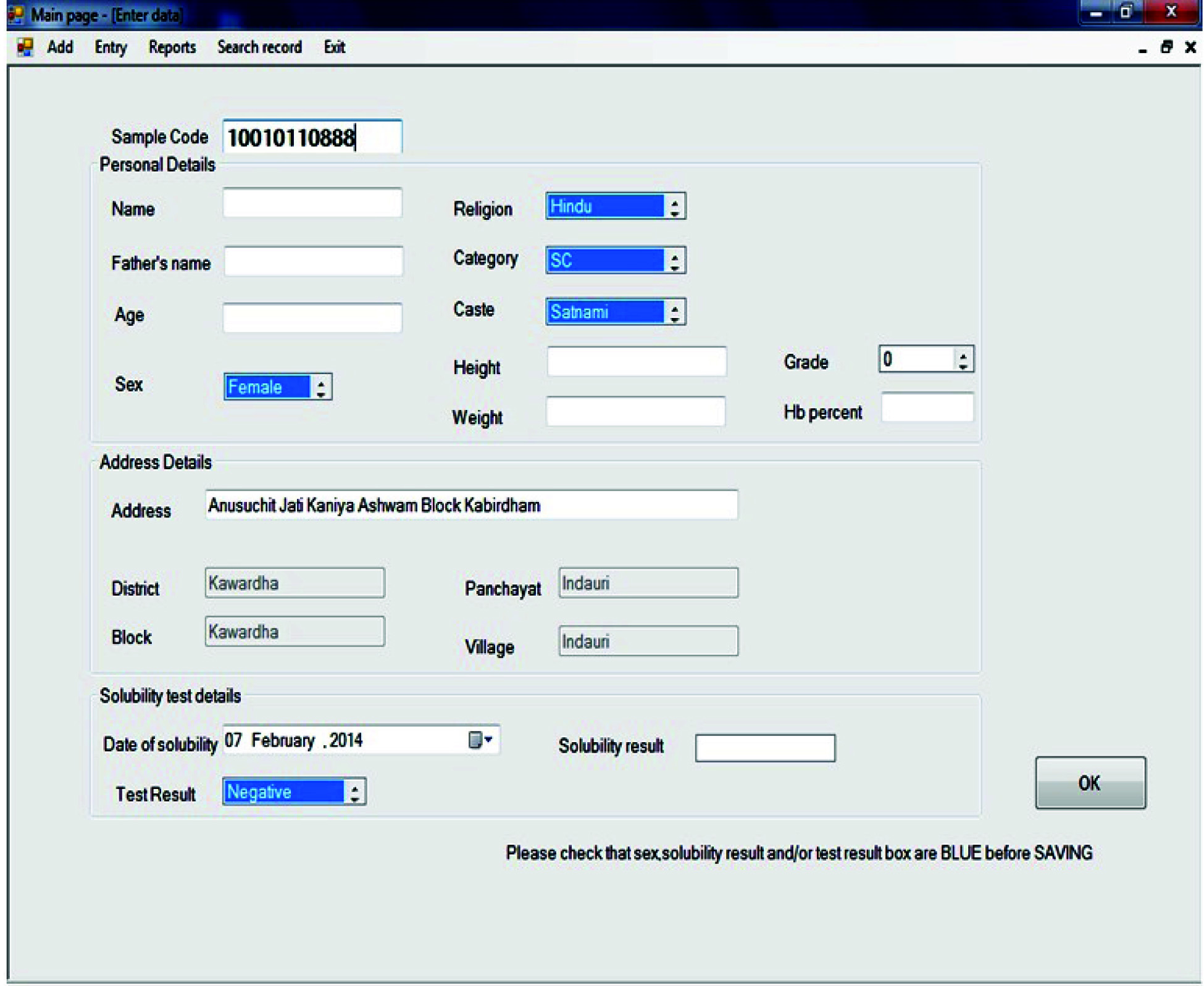
To store and manage the data generated through state wide screening program a medical informatics solution referred as SWSDI, was developed. Programming was done using VB.Net platform. For creating back end database, SQL Server 2012 platform was used. One login form was included in front page of graphical user interface for providing security to the data from unauthorized access. One parent form was designed that can be accessed after successful login, and provides access to entire solution through various forms. Among these forms, first is demographic location selection form, which helps to enter the exact demographic location of the screened persons detailing his/her district, block, panchayat and village. A serial number referred as ‘Sample Code’ is automatically generated for the person screened, once his/her demographic data has been entered [Table/Fig-1]. After entering the demographic data, personal and screening data is entered. Personal data to be entered includes person’s name, father’s name, age, gender, caste & category and religion. Further, address of the school in which screening was performed and his/her standard in the school at the time of screening are also entered. Screening data includes date, result of haemoglobin solubility test, haemoglobin electrophoresis test and haemoglobin level of the screened person. In addition, the interface provides facility for searching screening data records based on demographical information and/or name of persons. Moreover, if it has been entered incorrectly, editing of data can be done. All the data is stored in a centralized database and is easily accessible by multiple users at a time on institute’s intranet though login interface.
Screenshot of SWSDI showing fields for entering personal and screening related information of screened individuals.
Collection of Clinical Data at OPD
OPD of institute was started in January 2014. Valuable data is generated through findings in history, clinical examination, pathological and clinical chemistry laboratory tests etc. Single cross sectional data is strengthened by recording time series or temporal data generated at subsequent visits of patients for getting treatment. All the data generated is entered in the system on the same day and stored for any future reference.
Development and Implementation of SCPTDMS
In the second phase, SCPTDMS was developed and implemented in the OPD of institute. This system has been developed to keep records of patients visiting the OPD of institute. For this system also, programming was done using VB.Net platform and back end database was created using SQL Server 2012 platform. The system generates a unique serial number for each new patient that may be used for any future reference. Major forms used to enter data include complaints, Menstrual and obstetric history, Family History, History of past illness, History of blood transfusion, General examination, Drug therapy, Vaccination status, Vital signs & inspection, Investigations and follow up data [Table/Fig-2]. The forms have been designed and customized in consultation with clinicians and scientists dealing with SCD patients at the institute.
Screenshot of SCPTDMS showing fields for entering relevant data for SCD patients
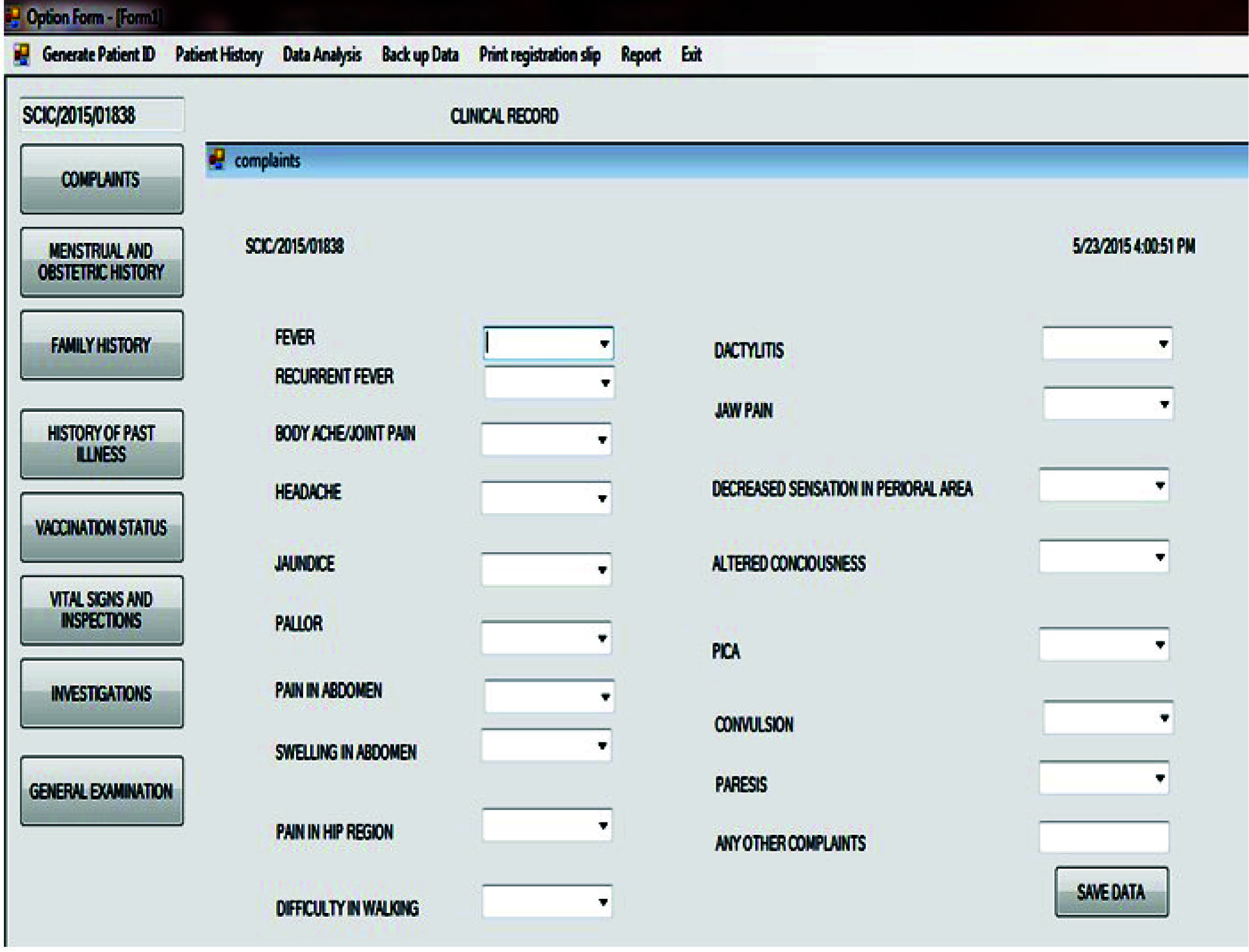
Form ‘Complaints’ is used to enter data regarding complaints of fever, recurrent fever, body ache/joint pain, headache, jaundice, pallor, pain in abdomen, swelling in abdomen, pain in hip region, difficulty in walking, dactylitis, jaw pain, decreased sensation in perioral area, altered consciousness, pica, convulsion, paresis and any other complaints [9]. Form for menstrual and obstetric history has fields for entering data related to parity, age at menarche, menstrual cycle, hysterectomy, duration of menstrual period, amount of blood flow, dysmenorrhoea/amenorrhoea, abortions and growth [10]. Family History includes fields for sickle cell status for father, mother, sister/s, brother/s, and other relatives on maternal and paternal side. Form for history of blood transfusion includes number of hospitalizations, number of blood transfusions, age at the time of first blood transfusion, age at the time of last blood transfusion, iron overload and age at which first manifestation occurred.
Form for drug therapy includes fields for folic acid, vitamin B12, hydroxyurea, penicillin, any surgical history and any history of drug allergy. Form for vaccination status includes fields for BCG, DPT, OPV, MMR, Hib meningitis vaccine, pneumococcal vaccine, vaccine for hepatitis, flu, typhoid and status of TB skin test. Form for vital signs and inspection includes fields for pulse, respiration, blood pressure, temperature, icterus, cyanosis, oedema, lymphadenopathy, haemolytic face, discharging sinus, non healing ulcer, priapism, localized/generalized swelling of limbs, bony tenderness, swelling of joints, restricted moments of hip and shoulder joint, shortening of limb, short stature and any other findings [11].
Form for investigations includes fields for solubility test, cellulose acetate electrophoresis, HPLC including HbS, HbA, HbF & HbA2, DNA analysis and other pathological and clinical laboratory tests [12]. Complete blood counts include haemoglobin level, hematocrit, reticulocyte count, total leukocyte count, differential leukocyte count, platelet count and red blood cell count. Liver function tests include serum bilirubin including total and conjugated, total serum protein, albumin/globulin ratio, enzymes including SGPT, SGOT, ALP and others [13]. Renal function test include blood urea, serum creatinine, and electrolytes [14]. Other fields include iron status, arterial blood gases, urine analysis, electrocardiography, echocardiography, X-ray, ultrasonography, computed tomography scan, magnetic resonance imaging scan etc. Follow up data includes haemoglobin, HPLC, blood cell counts, RBC indices etc that are relevant in maintenance of therapy for SCD patients.
Results
Efficient Storage and Easy Access to Screening Data
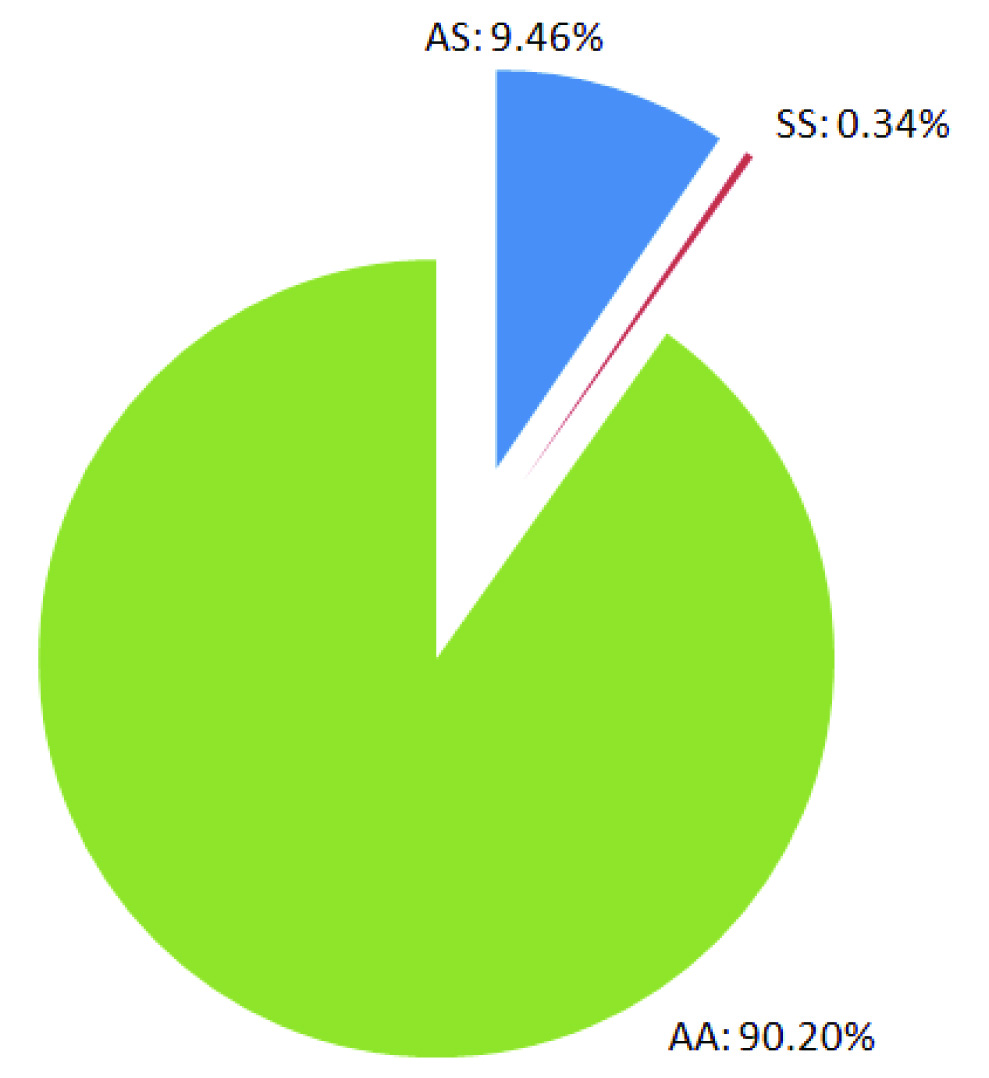
SWSDI is being used to store and manage state wide screening data in computerized data format, which was previously kept in hard copy on paper. Manual record keeping was time and space consuming. It required large number of staff, had issues related to data redundancy, security, vulnerability to hazards like fire. Transition of the method of storing the screening data has provided an easy and safe storage method. The benefits include easy access, security, management, editing and analysis of data through a single platform. Till June 2015, screening data of 1305357 persons from fourteen districts (nine districts: regular screening, five districts: special camps) has been stored in this system, out of which 123529 and 4457 have been found to be carriers and patients respectively for SCD [Table/Fig-3] [15]. Current distribution of AA, SS and AS genotypes found through ongoing SCD screening program till June 2015 is also shown [Table/Fig-4].
Results of SCD screening program till June 2015.
| Districts | SCD Status | Total |
|---|
| Negatives | Positives |
|---|
| AA | AS | SS |
|---|
| Durg | 244158 | 22163 | 706 | 267027 |
| Kawardha | 88974 | 10456 | 371 | 99801 |
| Mahasamund | 135866 | 17967 | 707 | 154540 |
| Raipur | 241431 | 24861 | 1012 | 267304 |
| Bemetara | 59837 | 5189 | 153 | 65179 |
| Baloda Bazaar | 173383 | 17901 | 336 | 191620 |
| Balod | 94670 | 11041 | 435 | 106146 |
| Mungeli | 65613 | 4919 | 199 | 70731 |
| Gariyaband | 68541 | 7864 | 250 | 76655 |
| Dhamtari | 2103 | 262 | 20 | 2385 |
| Korba | 1205 | 751 | 250 | 2206 |
| Dantewada | 286 | 50 | 8 | 344 |
| Jashpur | 323 | 0 | 0 | 323 |
| Bilaspur | 981 | 105 | 10 | 1096 |
| Total | 1177371 | 123529 | 4457 | 1305357 |
Current distribution of AA, SS and AS genotypes found through ongoing SCD screening program till June 2015.
Efficient Patient Handling in OPD of Institute
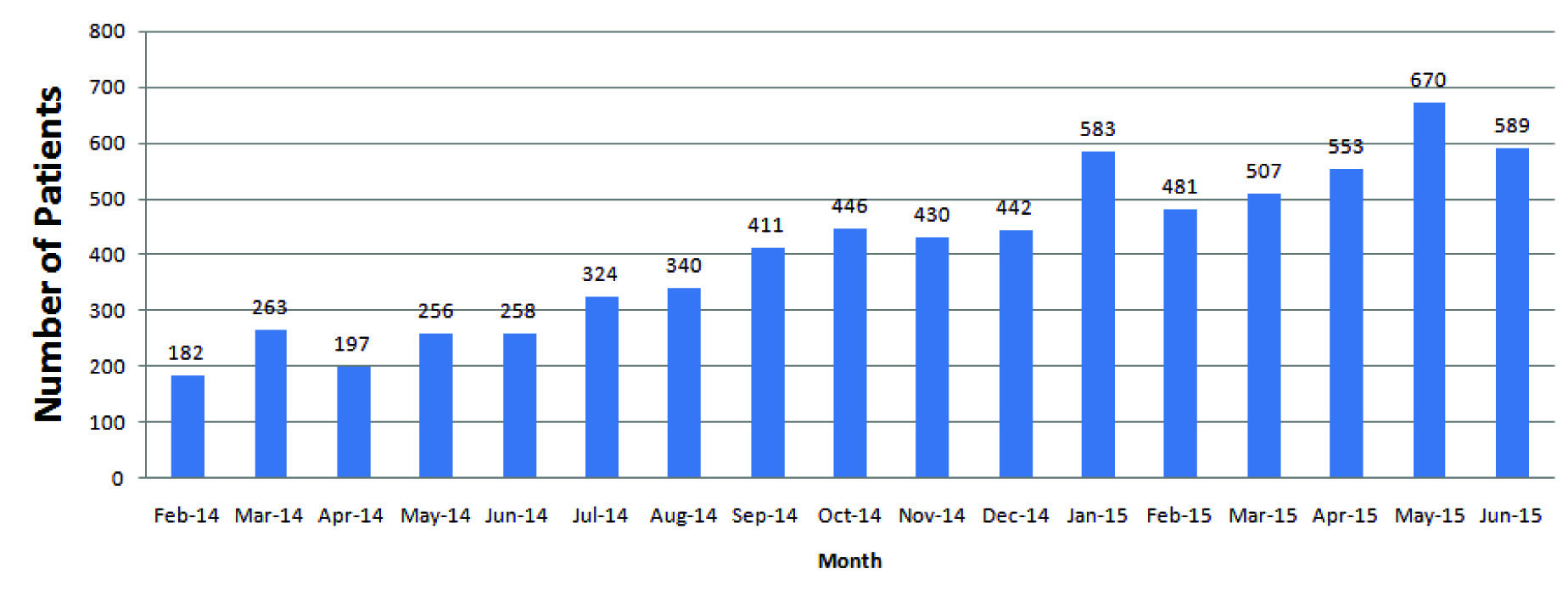
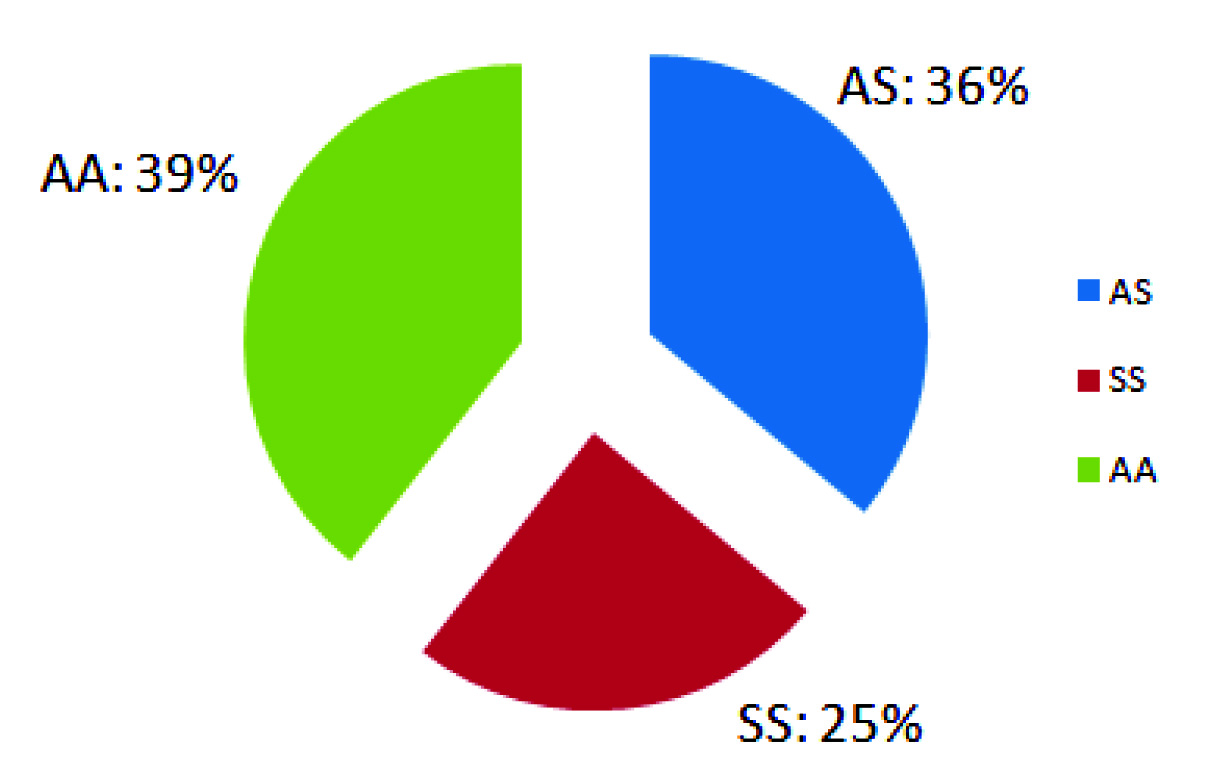
SCPTDMS has been already implemented in the OPD of institute. All the activities ranging from patients’ registration, their tracking, storing and managing their demographic, clinical and diagnostic data are being done through this interface. This interface is also a secured system to protect the patients’ data from unauthorized access. This system has made the handling of patients in OPD faster, easier and more efficient. Monthly patients’ attendance record is being maintained through SCPTDMS, which is helpful in monitoring the function of OPD [Table/Fig-5]. Till June 2015, SCPTDMS has data of 3760 persons, of which 923 are sickle cell disease patients (SS) and 1355 are sickle cell carriers (AS) [Table/Fig-6].
Monthly patients’ attendance record generated through SCPTDMS till June 2015.
Current distribution of AA, SS and AS genotypes registered in SCPTDMS till June 2015
Discussion
Monitoring of State-wide Screening Program
SWSDI has made it possible to keep an eye on the prevalence of sickle cell disease in an efficient manner. It can be used to mine the data for demographic analysis of screening data as number of persons screened for SCD in a particular geographical area and the number of persons found to be sickle cell carriers and patients. This interface is also being used to monitor the progress of state wide screening for SCD in Chhattisgarh, by assessing the number of screened persons in each district in a particular period of time. The feedback is sent to the supervisors and workers engaged in screening work for better implementation of screening program in which nine districts of the state have been covered till date.
Personalizing Therapeutic Regimen through Monitoring Temporal data
Patients’ clinical data including signs and symptoms of disease, medications given and their effects and laboratory diagnostic data that are recorded as time series or temporal data, can be analysed at any time. This analysis is used to judge the patient’s response to treatment and suggest any changes or modifications in the therapeutic regimen being given [16]. The only disease modifying drug available for SCD is hydroxyurea, which increases the level of protective fetal haemoglobin (HbF) level; is a potentially toxic drug leading to myelosuppression and renal failure [17]. Thus all the concerned clinical parameters including levels of haemoglobin variants, blood cell counts, renal function parameters are estimated at different time intervals and stored in the system as temporal data. This feature has made it easy to perform temporal analysis of data to judge the response of the patient to the therapeutic regimen and personalizing it as per requirement.
Providing Valuable Data for Research in SCD
As SCD is more prevalent in countries, lacking in resources, developed countries have not paid the required attention to pursue research in this field. Country like India has an opportunity to proactively pursue research in this field for benefit of the lacs of SCD patients in India and worldwide [18]. The screening and temporal data stored in the developed systems can be made readily available for use in research activities related to SCD with due consent of patients or their guardians. The data may be useful in pursuing research in clinical, molecular and health system related aspects of SCD in India.
Exploiting the Benefit of Information Technology for Medical Field
As discussed in methodology section, both of these systems have been developed on VB. Net and MS SQL Server 2012 platforms. This exercise has shown the advantages of a keeping electronic medical record over keeping the records in manual form or in any spreadsheet. Back end database takes care of the integrity of a record stored, which is not possible in MS Excel or manual form. An audit trail i.e., record of all changes made with time and the person who made the changes in any record; are maintained by the back end database system. Data security has been considered very rigorously and the systems provide restricted access as per the permissions to different levels of users. Data can be visualized by any user but it can be modified by database administrator only. Implementation of these systems has reduced the tedious work required for manual record keeping and provided a better measure to store and access data in comparison to previous methods. Further, the data is being stored in digital form that is safer for long durations in comparison to keeping records manually on paper.
Future Perspective
Huge amount of data is available through state wide screening program for SCD for 9 districts through regular screening and 5 districts through special camps. This data may be utilized in mapping the prevalence of SCD patients and carriers in all the 27 districts of Chhattisgarh. The mapping may provide projected number of SCD patients and carriers in all districts of Chhattisgarh, which may be used to design future strategies and programs to control SCD in the state considering regional requirements at district level. Moreover, the systems developed may be upgraded for smart phone based real time data entry and analysis.
Limitations
The system requires preinstalled SQL Server and Microsoft. Net Framework for proper functioning. Further, follow up facility is not available for patients. This facility is in the process of addition in the next version of this system, so that patients will be able to get an automated reminder for their due visit to the institute’s hospital through call or SMS. Moreover, as the screening is an ongoing process in distant areas of the state, the data is entered in the system on weekly intervals. Work is going on to develop an online smart phone based interface to facilitate real time entry of screening data into the system.
Conclusion
Although several questions are raised regarding implementation of EMR systems, like costs involved, training of personnel engaged in entry of data and dependence on technology etc; implementation of EMR systems has been a major step forward in improving the standard of care being provided for SCD patients. Several of such systems are available in market, but the systems were developed indigenously to save the financial resources and cater the specific requirements of clinicians and scientists working with SCD patients, which could not be catered through other systems. The staff, clinicians and scientists have been trained to use these systems and the systems are being used efficiently for welfare of SCD patients of the state.