Acute Exercise-Induced Compartment Syndrome of the Leg- Don’t Miss It
Manish Dewangan1, Manish Kumar Khare2, Sumanta Mishra3, Jogesh Chandra Marhual4
1 Surgical Specialist, JLN Hospital & Research Centre, Bhilai (CG), India.
2 Assistant Professor, Department of Surgery, CM Medical College, Durg (CG), India.
3 Joint Director, Department of Surgery, JLN Hospital & Research Centre, Bhilai (CG), India.
4 Joint Director, Department of Surgery, JLN Hospital & Research Centre, Bhilai (CG), India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manish Dewangan, Street-16,14/A Hospital Sector, Bhilai (CG)-490009, India.
E-mail: drmanishd78@gmail.com
Acute exercise induced compartment syndrome of leg is a very rare and very oftenly missed entity which leads to delay in its management. We are presenting such case in which diagnosis was established two days after the onset of symptoms. Urgent decompressive fasciotomy was done. After 3 months of follow up, patient has got full functional recovery of his affected limb. This case highlights the importance of keeping high index of clinical suspicion to diagnose the problem and manage promptly. We have reviewed the English literature and found only about 40 cases since 1945.
Acute compartment syndrome of leg, Anterior tibial syndrome, Fasciotomy, March gangrene
Case Report
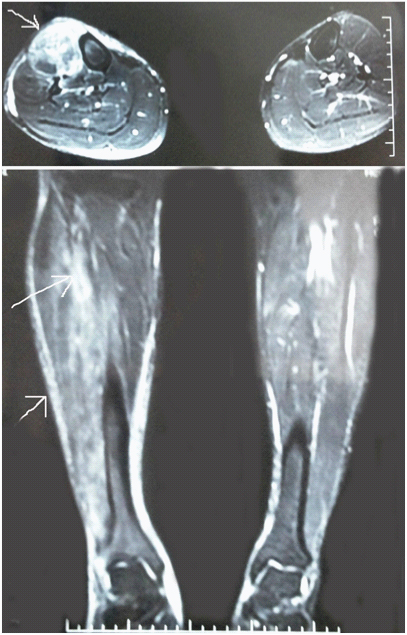
A 54-year-old man was presented to the emergency in the night with pain all over body, especially in the right lower limb and vomiting following heavy exercise. Patient was not a regular athlete. He had done vigorous heavy weight lifting exercise of the legs in the evening under the influence of alcohol. He felt generalized body ache, especially in the right leg. After sometimes, he started vomiting and then rushed to the emergency for further management. He was a known hypertensive and diabetic, on regular treatment. On general examination, he was restless and his BP was 170/100 mm Hg. He was admitted in the medical ward. Blood investigation revealed hyponatremia (serum Na-114 mmol/l and K-4.7 mmol/l) and markedly elevated serum CK (serum CK-37599 U/l). Subsequently, his sodium was corrected but CK remained elevated. On the next day, he started localizing pain in right leg anteriorly. His pain, initially thought to be due to muscle pull and/or soft tissue injury, was getting worsened. After two days of admission, his pain got aggravated with underlying muscle became tender and overlying skin became indurated. Dorsiflexion of the foot was absent and plantar flexion also was painful. Distal arterial pulsations were intact. There was no sensory loss but foot drop was present on the right side. MRI of both lower limb revealed oedema of extensor muscles on right side anterior compartment [Table/Fig-1]. Rest of the leg compartments were normal. The clinical diagnosis of acute compartment syndrome of anterior compartment of the right leg was made. Urgent decompressive fasciotomy of right anterior compartment was done. There was bulge of the extensor muscles. Colour of the muscle was dusky with poor contractility. No debridement was carried out. Wound was left open and relooked after 48 hours. The dusky muscle regained its normal colour with no further necrosis. Fasciotomy wound became infected in the meantime and was managed with local wound care and appropriate antibiotics [Table/Fig-2a&b]. He started walking. Initially he was able to walk with the help of sticks due to foot drop but his condition improved subsequently and after 3 months his gait became absolutely normal with power 5/5. He is walking normally without any problems after 2 years of follow up.
MRI of both lower limbs. Arrow showing oedema of the extensors of anterior compartment of right lower limb
Fasciotomy wound after 1 month.


Discussion
Acute exercise-induced compartment syndrome of leg is defined as an acute compartment syndrome arising in the leg in the complete absence of any trauma or surgery, in individuals without pre-existing risk factors for the development of the condition, following athletic activity [1]. Of all the four compartment of leg, anterior compartment is the most commonly affected because of its rigid boundaries [2]. The average incidence of ACS of leg is 3.1 per 100000 people (7.3 per 100000 men with mean age of 32 years and 0.7 per 100000 women with mean age of 44 years). Various causes have been described ranging from bony and soft tissue injury, crush syndrome, revascularization, exercise, snake bite, burns to many medical comorbidites including diabetes, hypothyroidism and bleeding diathesis [3]. After being first described by Vogt in 1943 [4], exercise-induced ACS of anterior compartment of leg is still an exceptional entity with only less than 40 cases reported in the literature so far [1,5].
Exercise - induced compartment syndrome of anterior leg can manifest in two ways-Acute compartment syndrome (as in our case) and chronic compartment syndrome. The basic pathophysiology behind this is that the capacity of the anterior compartment is fixed and exercise causes 20% increase in the volume of muscles. When an unaccustomed person undergo exercise, at a particular point of time he will feel pain. That pain is the limit point of his activity. If he stops at that point his pain will subside but if he continues his vigorous activities, he may get permanent injury which will not subside with rest [5]. There occurs impaired perfusion resulting in ischemia, oedema and rising interstitial fluid pressure further compromising capillary flow. The blood flow ceases in the microcirculation when the local tissue pressure is equal to the diastolic pressure. Muscle metabolism ceases when the pressure gradient is less than 30 mmHg between the compartment and the mean arterial pressure [6]. In our case, there was no history of any precipitating cause except exercise, no history of pain on exercise which got relieved by rest. The typical intraoperative findings and relief of symptoms after surgery suggest that this compartment syndrome is solely due to acute exercise.
The most unfortunate part of this entity is delay in the diagnosis because it mimics with soft tissue injury, cellulitis, nerve injury or simply a muscle pull. Most radiological tools fail to diagnose the problem. MRI is able to detect soft tissue oedema and swollen compartments but cannot differentiate between the oedema of affected muscles in compartment syndrome and that of soft tissue injury after trauma [7]. Diagnosis is established on clinical grounds in most of the cases. Compartmental manometry is a very useful tool in establishing the diagnosis in doubtful cases. The normal resting intracompartmental pressure (ICP) is 0-8 mm Hg. Absolute ICP of 30mm Hg and a difference of less than 30 mm Hg between diastolic blood pressure and ICP are both commonly accepted threshold for surgical intervention [1,8]. Urgent decompressive fasciotomy of the affected compartment is the only treatment [8]. A high degree of suspicion is required for its diagnosis and appropriate management because delay can not only lead to permanent disability and mortality but also has got embarrassing medicolegal implications [9].
Conclusion
To conclude, we should be aware of this rare entity and an early surgical intervention should be considered to prevent permanent limb morbidity. Compartmental manometry is a useful test when there is diagnostic dilemma.
[1]. Insull P, Young SW, Acute exercise-induced compartment syndrome of the leg: an Aukland seriesNZMJ 2009 122(1295)ISSN 1175 8716. URL:http://www.nzma.org.nz/journal/122-1295/3614/ [Google Scholar]
[2]. Sweeney RC, Chadwick CJ, Bagnall WE, Exercise–induced anterior tibial compartment compression syndrome in the elderlyPostgraduate Medical Journal 1981 57:537-38. [Google Scholar]
[3]. Mauser N, Gissel H, Henderson C, Hao J, Hak D, Mauffrey C, Acute Lower-leg Compartment SyndromeTrauma update 2013 36(8):619-24. [Google Scholar]
[4]. Vogt PR, Ischemic muscular necrosis following marching. Unpublished but read before the Oregon State Medical Society, 4 September 1943Quoted by Horn in Journal of Bone and Joint Surgery 1945 27:615-22. [Google Scholar]
[5]. Blandy JP, Fuller R, March Gangrene; ischemic myositis of the leg muscle from exerciseThe Journal of Bone Joint Surgery 1957 39-B(4):679-93. [Google Scholar]
[6]. Sebag MM, Laversuch C, Witt J, Alcohol abuse associated with anterior tibial compartment syndrome-should it be a recognized complication?Journal of the Royal Society of Medicine 1992 85:112-13. [Google Scholar]
[7]. Rominger M, Lukosch C, Bachmann G, Compartment syndrome: value of MR imagingRadiology 1995 197:296 [Google Scholar]
[8]. Shadgan B, Menon M, Sanders D, Berry G, Marth C, Current thinking about acute compartment syndrome of the lower extremityCan J Surg 2010 53(5):329-34. [Google Scholar]
[9]. Mabvuure NT, Malahias M, Hindocha S, Khan W, Juma A, Acute Compartment Syndrome of the Limbs: Current Concepts and ManagementThe Open Orthopedic Journal 2012 6(Suppl 3:M7):535-43. [Google Scholar]