Introduction
Oral cancer is a challenging disease in Indian subcontinent because of increased use of tobacco and associated products. Although surgery is the main treatment modality, radiotherapy (RT) and chemotherapy (CT) are employed in inaccessible cases. Both RT & CT will result in painful and debilitating adverse effects in oral cavity e.g., mucositis, ulceration, dysgeusia, xerostomia and opportunistic infections. One of the most common opportunistic infection is caused by fungus Candida.
Aim
Our aim was to investigate the incidence of oral colonization of Candida species with differentiation between carrier and infective state of the organism. We also investigate the effect of treatment modality (RT and CT) on the incidence of Candida, in oral cancer patients, undergoing RT and/or CT, in order to prevent and treat the Candida infection in a better way.
Materials and Methods
It was a cross-sectional case-control study; done in Gujarat, India. Fifty patients of oral cancer undergoing RT, CT alone or combined were investigated and compared with the healthy controls. The samples were collected from mid-dorsum of tongue by using imprint culture technique. The samples were inoculated on Sabouraud’s dextrose agar medium and the organisms were identified by wet mount, germ tube test, chlamydospore formation and sugar fermentation tests.
Results
There was significant increase in oral Candida colonization from 20% in healthy controls to 70% in oral cancer patients undergoing RT and/or CT (p = 0.001, < 0.05). A significant increase in infective state of Candida (71.4%) was noted (p = 0.001, < 0.05) with predominance of non-albicans species of Candida, chiefly C. tropicalis (42.8%).
Conclusion
RT and CT leads to increased oral colonization and infection by Candida with a shift towards growth of non-albicans species. As the pattern of candidal species infection is changing, such studies are important for better diagnosis and treatment planning to gain good control over the disease.
Adverse effects of radiotherapy and Chemotherapy, Candida albicans, Oral candidiasis, Opportunistic pathogen
Introduction
Cancer is one of the major causes of morbidity and mortality in the modern era [1]. Worldwide, an estimated cancer incidence of about 10 million was reported for the year 2009 [1] and 1 out of every 3 persons is estimated to suffer from cancer by age of 75 years [2]. “Oral cancer” encompasses all malignancies originating in the oral cavity. It is often grouped together with cancers of pharynx as “Oropharyngeal” cancer [3]. Oral cancer ranks sixth among the overall incidence for the 10 most common sites worldwide and third in the developing countries [2]. In Indian subcontinent, it is one of the leading causes of morbidity and mortality, because of increased use of tobacco smoking and chewing. In India, oral cancer, constituting 9.8% of an estimated 644,600 incident cancer cases in 1992, rank first among all cancer cases in males and is the third most common among females in many region, with age standardized incidence rates from 7-17/100,000 persons/year; the incidence rate being higher than the western rate of 3-4/100,000/year [4]. The mortality rate is lowest for lip cancer (0.04 per 100,000) and highest for the tongue (0.7 per 100,000) [4]. The advent of newer imaging techniques and treatment modalities greatly improve the prognosis of the disease. While surgery remains the mainstay of the treatment, radiotherapy (RT) and chemotherapy (CT) is also used as an adjuvant treatment modality.
Radiotherapy is used as a primary mode of treatment mainly in carcinomas of base of tongue because tumours are radio responsive and surgery is not advisable due to anatomical barriers. Radiotherapy causes oral mucositis, ulceration, dysgeusia and dysphagia. If salivary glands are involved during RT, both structural and functional changes occur in salivary glands. It affects saliva, both qualitatively and quantitatively, making it thick and ropy with decrease in quantity that leads to xerostomia. Irradiation induced oral ulcerations and xerostomia have been reported to facilitate Candida growth [4].
Chemotherapy is used as an adjuvant to surgery and RT. It is most benefited in treatment of laryngeal and nasopharyngeal carcinomas. Cytotoxic drugs mainly affect cells in mitosis, destroying rapidly dividing, immature carcinoma cells as well as normal cells of body e.g., cells of oral and gastrointestinal mucosa, bone marrow and skin. The most common oral reaction of chemotherapy is diffuse and multiple mucosal erosions and ulcerations. These ulcerations are frequently infected by secondary bacteria and fungi, commonly by Staphylococci, streptococci and Candida, mainly because of neutropenia [4].
Candida species are usually normal oral commensal and their transition to an opportunistic pathogen may be associated with the virulence of the organism and the host factors. Candidal species e.g., C. albicans, C. tropicals, C. krusei, C. parakrusei, C. glabrata, C. guillermondii, C. parapsilosis, C. kefyr/pseudotropicalis, C. dubliniensis, C. viswnathii and C. stellatoidea, can be isolated. C. albicans is the most common species detected in the oral cavity of both healthy and medically compromised individuals [5].
Oral candidal carriage was reported by various authors in healthy as well as in immunocompromised individuals. The prevalence of yeast in the oropharynx of healthy volunteers was reported to be 35%, by Cohen et al., [6]. The oral Candida colonization (up to 93%) and infection (up to 30%) were seen in oral cancer patients undergoing RT [7]. The oral carriage rate of Candida species increases to 75% in oral cancer patients with CT in comparison to 40% in healthy control [8].
Aim
The aim of this study was to analyse oral Candida colonization and identification of the species of Candida with differentiation between carrier and infective state of the Candida in Indian oral cancer patients undergoing RT and CT and compare it on different parameters with healthy controls.
Materials and Methods
It was a cross-sectional, case control study conducted in a period of two years between 2013 to 2015, in which the study group consisted of 50 Indian patients suffering from oral cancer and undergoing RT and/or CT at Gujarat Cancer Research Institute, Ahmadabad. Permission from ethical committee of the institution was taken and patients consent was obtained prior to investigation. Patients with histological diagnosis of carcinoma of oral cavity e.g., carcinoma of lip, buccal mucosa, retro-molar triangle, lateral surface of tongue, base of tongue, maxillary alveolus and mandibular alveolus, undergoing RT and/or CT, were included in the study. The patients with carcinoma of vocal cord and oesophagus and who were undergoing antifungal medications were excluded from the study. The control group comprised of 50 healthy individuals of similar age group, not suffering from any major disease and were not undergoing any medication for any chronic illness. The demography, clinical and treatment characteristics of the study group were described in [Table/Fig-1]. After taking detailed history, intra-oral examination was done to note the presence and nature of oral Candidiasis. Only lesions that were clearly visible were noted.
Demographic, clinical and treatment modality characteristics of the study group.
| Variable | Category | n (%) |
|---|
| Total no. | 50 |
|---|
| Age | Range | 32-65 |
| Mean | 48.56 |
| Gender | Male | 40 (80) |
| Female | 10 (20) |
| Tumor site | Base of tongue | 18 (36) |
| Lateral surface of tongue | 12 (24) |
| Buccal mucosa | 10 (20) |
| Lower lip | 2 (4) |
| Alveolus maxilla | 4 (8) |
| Alveolus mandible | 4 (8) |
| Clinical presentation | Ulceration | 20 (40) |
| Xerostomia | 15 (30) |
| Dysphagia | 10 (20) |
| Asymptomatic | 5 (10) |
| Treatment modality | Radiotherapy | 14 (28) |
| Chemotherapy | 20 (40) |
| Combination of RT & CT | 16 (32) |
In order to investigate possible presence of Candida and to differentiate between the carrier state and infective stage of the organism, imprint culture technique as described by Arendorf and Walker [9] was applied in all patients. In brief, a sterile square plastic foam pad dipped in sterile saline was held on the middle third of dorsal surface of the patient’s protruded tongue for 10 seconds. The pad was then pressed firmly on to a Sabouraud’s dextrose agar plate into which gentamycin 20μg/ml and chloremphenicol 50μg/ml had been incorporated to suppress bacterial growth. Cyclohexamide 0.5 mg/ml is also added to prevent growth of saprophytic fungi. The pad was left in situ for 60 minutes and was then removed. The plate was incubated aerobically at 37°C for 2 days. The candidal density was then determined by enumerating the colonies. The patient is considered as carrier if dentate patient have <30 colonies/cm2, if denture wearer have <49 colonies/cm2. The patient is considered as infective if dentate patient have > 30 colonies /cm2, if denture wearer has >49 colonies / cm2. Confluent growth obtained from a mucosal surface was highly suggestive of Candida infection [9].
The colony characteristics were recorded and compared with known colony characters of various candidal species. If no colonies were seen on Sabouraud’s agar after 48hrs incubation, culture plate was kept for seven days in incubator before being considered as negative.
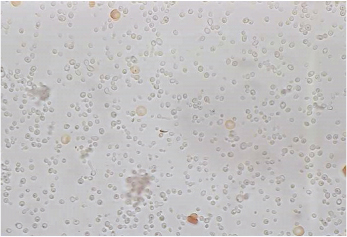
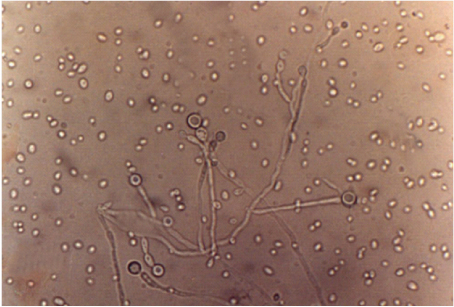
The morphology of the organism was studied by preparing Wet mount. The yeast appeared as gram positive, round to oval bodies. The species of Candida was identified by sugar fermentation tests. Further identification of C. albicans species was done by germ tube test [Table/Fig-2] and chlamydospores formation [Table/Fig-3].
Photomicrograph showing tube like, out growth from yeast cell - germ tube, C. albicans (45 X).
Photomicrograph showing thick walled chlamydospores at the end of pseudo-hyphae on cornmeal agar plate. C. albicans (45 X).
Results
Candida colonization
Out of 50 healthy controls, 10 (20%) had shown positive Candida culture while out of 50 oral cancer patients undergoing RT and/ CT, 35 (70%) patients had shown positive Candida culture (p = 0.001, < 0.05) [Table/Fig-4]. Candida was cultured in 50% of the patients taking RT, 75% of the patients taking CT and 81.25% of the patients taking RT and CT both [Table/Fig-5].
The prevalence and growth pattern of Candida from oral cavity of controls & oral cancer patients receiving RT &/or CT.
| Groups | Total no. | Candida culture | Candida growth pattern | Candida species |
|---|
| Positive | Negative | Carrier | Infective | C. albicans | C. stellatoidea | C. tropicalis | C. krusei |
|---|
| Controls | 50 | 10 (20%) | 40 (80%) | 10 (100) | - | 7 (70%) | 3 (30%) | - | - |
| Oral cancer patients | 50 | 35 (70%) | 15 (30%) | 10 (28.58%) | 25 (71.42%) | 5 (14.28%) | 10 (28.57%) | 15 (42.85%) | 5 (14.28%) |
The relationship between prevalence and growth pattern of Candida and treatment modality of oral cancer patients.
| Treatment group for Oral cancer patients | Total no. | Candida culture | Candida growth pattern | Candida species |
|---|
| Positive | Negative | Carrier | Infective | C. albicans | C. stellatoidea | C. tropicalis | C. krusei |
|---|
| Radiotherapy | 14 | 7 (50%) | 7 (50%) | 2 (28.57%) | 5 (71.42%) | 2 (28.57%) | 2 (28.57%) | 3 (42.85%) | - |
| Chemotherapy | 20 | 15 (75%) | 5 (25%) | 3 (20%) | 12 (80%) | 3 (20%) | 3 (20%) | 6 (40%) | 3 (20%) |
| Combined RT & CT | 16 | 13 (81.25%) | 3 (18.75%) | 5 (38.46%) | 8 (61.53%) | - | 3 (23.07%) | 8 (61.53%) | 2 (15.38%) |
(Chi-square test: p=0.01, Not significant)
Candida infection
All positive healthy controls had shown carrier growth pattern of Candida while out of 35 Candida positive oral cancer patients, 10 (28.57%) were in carrier and 25 (71.42%) were in infective state (p = 0.001, < 0.05) [Table/Fig-4]. The infective state of Candida was seen in 71.42% in patients undergoing RT, 80% in patients undergoing CT and 61.53% in patients on RT and CT both [Table/Fig-5].
Candida species isolation
In healthy controls, out of 10 positive controls, 7 (70%) were identified as C. albicans and 3 (30%) were C. Stellatoidea [Table/Fig-4]. In 35 Candida positive oral cancer patients undergoing RT &/CT, the most common candidal species identified were C. tropicalis, in 15 (42.85%) patients. followed by C. stellatoidea in 10(28.57%), C. albicans in 5 (14.28%), and C. Krusei in 5 (14.28%) patients [Table/Fig-5].
The relationship between prevalence and growth pattern of Candida and treatment modality of oral cancer patients: The oral cancer patients undergoing RT, showed 50% Candida positive culture with 71.42% were in infective state and 71.42% were non albicans species. The oral cancer patients undergoing CT, showed 75% Candida positive culture with 80% were in infective state and 80% were non albicans species. The oral cancer patients undergoing both RT and CT showed 81.25% Candida positive culture with 61.53% were in infective state and 100% were non albicans species [Table/Fig-5].
Discussion
Oral candidiasis is one of the most common opportunistic infection of the oral cavity. It is caused by a yeast-like fungus, Candida, which is present in oral cavity as commensal and becomes pathogenic when the host defense is compromised. Oral candidiasis manifested as acute or chronic disease and either superficial or disseminated systemic mycosis [10]. There are many systemic conditions which leads to immune-compromised state e.g., diabetes mellitus, HIV, patients undergoing solid organ and bone marrow transplants and patients undergoing chemotherapy and radiotherapy targeted against carcinomas and sarcomas [4]. Oral candidiasis is common in patients with head and neck cancers, especially during chemotherapy and radiotherapy. It usually manifest as acute erythematous candidiasis, but the diagnosis may often be missed, as it may be mistaken for radiation mucositis [11].
In the present research, a total of 50 cases of oral cancer undergoing RT and CT, were screened and compared with a control group of 50, healthy controls of same age group, for oral Candidal isolation and species identification.
We observed significant increase in oral carriage of Candida in oral cancer patients taking RT &/ CT, it was 50% in patients taking RT, 75% in patients taking CT and 81.25% in patients taking RT v CT both, in comparison to 20% Candida prevalence in healthy controls. This is in accordance with findings of previous studies. Silverman et al., and Chen and Webster found 49% and 63% Candida carriage in patients taking RT in comparison to 22% and 29.1% in healthy controls respectively [12,13]. Samaranayake et al., and Main et al., found 70% and 75% Candida carriage in patients taking CT respectively [8,14]. The candidal carriage rate increased from 70% to 80% during the 3 months period of cytotoxic therapy [8]. Main et al., found that the saliva volume & salivary amylase activity decreased and candidal score increased after the cytotoxic therapy. The carriage of coliforms was also increased [14].
The significantly increased in Candida carriage may be due to compromised defence system of host because of underlaying disease and use of cytotoxic drugs. Moreover, RT causes mucositis and changes in salivary glands which lead to quantitative and qualitative changes in saliva [12]. Xerostomia and thick saliva makes the oral environment conducive for fungal colonization.
Apart from isolation of Candida, the growth pattern of Candida is also changed from carrier to infective state, in oral cancer patients undergoing RT and/or CT. In our observation all healthy controls (100%) showed carrier growth pattern while 71.42% oral cancer patients showed infective growth pattern. It shows significant increase in the infective state of Candida in oral cancer patients undergoing RT and/ CT (p = 0.001, < 0.05). According to Ueta et al., the virulence of Candida strain in chemotherapy and irradiated individuals is largely determined by activities of adherence, multiplication and release of a cytoplasmic antigen, enolase & Candida aspartic proteinase [15].
By far the most pathogenic as well as most common species of Candida occurring as a commensal in healthy man are C. albicans followed by C. glabrata, C. Krusei, C. tropicalis & C. parapsilosis [16]. In accordance we found C. albicans in 70% positive healthy controls. The pattern is different in the oral cancer patients undergoing RT and/or CT, non-albicans species of Candida are predominantly isolated out of which the most common candidal species identified was C. tropicalis, (42.85%). Our results were in congruence with that of Belazi et al., Redding et al., and Dahiya et al., who reported non-albicans species of Candida in 12% to 30% of irradiated patients [17–19]. Jham et al., also reported similar findings, 33% increase in non-albicans species colonization, which increased to 71.4% at the end of study [20]. Hence we could suggest that the prevalence of non albicans species of Candida were increased in oral cancer patient undergoing RT &/ CT. Candida species distribution, especially non-albicans, varies worldwide. Studies reveal that in the United State/Canada region, the most common non-albicans species is C. glabrata while in South America C. tropicalis and C. parapsilosis are most common [20]. In India, we found predominance of C. tropicalis in our study which should be further evaluated on a larger sample size.
Conclusion
In conclusion, we found significant increase in candidal colonization in oral cancer patients of Indian origin, undergoing RT and/or CT, with change in the growth pattern of candida, from carrier to infective state. There is a shift toward non albicans species of Candida, chiefly C. tropicalis which are more bizarre in presentation and resistant to conventional treatment. As the pattern of candidal species infection is changing, such studies are important for better diagnosis and treatment planning to gain good control over the disease. Since, a small sample size has been the chief limitation of this study, we suggest further studies on larger study groups should be conducted to confirming the above findings. It will contribute better towards the prevention and control of oral cancer related candidiasis.
[1]. Jemal A, Siegel R, Xu J, Ward E, Cancer statistics, 2010CA Cancer J Clin 2010 60:277-300. [Google Scholar]
[2]. Johnson NW, Tobacco use and oral cancer : a global perspectiveJ Dent Educ 2001 65:328-39. [Google Scholar]
[3]. Daftary DK, Murti PR, Bhonsle RB, Gupta PC, Mehta FS, Pindborg JJ, Oral squamous cell carcinoma, In : Prabhu SR, Wilson DS, Daftary DK, Johnson NW, editorsOral Diseases in the Tropics 1992 2nd edOxfordOxford University Press:429-48.Ch. 37, [Google Scholar]
[4]. Rajendran R, Benign and Malignant tumors of Oral Cavity. In : Rajendran R, Sivapathasundaram B, editorsShafer’s Textbook of Oral Pathology 2011 7th edIndiaElsevier:102Ch. 2, [Google Scholar]
[5]. Xu J, Mitchell TG, Geographical differences in human oral yeast floraClin Infect Dis 2003 36:221-24. [Google Scholar]
[6]. Cohen R, Roth FJ, Delgado E, Ahearn DG, Kalser MH, Fungal flora of the normal human small and large intestineN Engl J Med 1969 280:638-41. [Google Scholar]
[7]. Ramirez-Amador V, Silverman S, Mayer P, Tyler M, Quivery J, Candidal colonization and oral Candidiasis in patients undergoing oral and pharyngeal radiation therapyOral Surg Oral Med Oral Pathol 1997 84:149-53. [Google Scholar]
[8]. Samaranayake LP, Calman KC, Ferguson MM, Macfarlane TW, Main B, Welsh J, The oral carriage of yeasts & coliforms in patients on cytotoxic therapyJ Oral Pathol 1984 13:309-93. [Google Scholar]
[9]. Arendorf TM, Walker DM, The prevalence & intra-oral distribution of candida albicans in manArch Oral Bio 1980 25:1-10. [Google Scholar]
[10]. Kantheti LP, Reddy B, Ravikumar S, Anuradha Ch, Chandrasekhar P, Rajeswari MR, Isolation, identifi cation and carriage of Candidal species in PLHA’s and their correlation with immunological status in cases with and without HAARTJ Oral Maxillofac Pathol 2012 16:38-44. [Google Scholar]
[11]. Bakki SR, Kantheti LP, Kuruba KK, Poosarla C, Baddam VR, Mulakaluri RR, Candidal carriage, isolation and species variation in patients undergoing radiotherapy and chemotherapy for head and neck tumoursJournal of Dr. NTR University of Health Sciences 2014 3(1):28-34. [Google Scholar]
[12]. Silverman JS, Luangjarmekorn L, Greenspan D, Occurrence of oral candida in irradiated head & neck cancer patientsJ Oral Med 1984 39:194-96. [Google Scholar]
[13]. Chen TY, Webster JH, Oral monilial study on patients with head & neck cancer during radiotherapyCancer 1974 34:246-49. [Google Scholar]
[14]. Main BE, Ferguson MM, Kaye SB, Macfarlance TW, Mairs RJ, Samaranayake LP, The effect of cytotoxic therapy on saliva & oral floraOral Surg Oral Med Oral Pathol 1984 58:545-48. [Google Scholar]
[15]. Ueta E, Tanida T, Yoneda K, Yamamoto T, Osaki T, Increase of Candida cell virulence by anticancer drugs and irradiationOral Microbiol Immunol 2001 16:243-49. [Google Scholar]
[16]. Fisher BM, Lamey PJ, Samaranayake LP, Macfarlane TW, Carriage of candida species in the oral cavity in diabetic patients: relationship to glycaemic controlJ Oral Pathol 1987 16:282-84. [Google Scholar]
[17]. Belazi M, Velegraki A, Koussidou T, Andreadis D, Hini S, Arsenis G, Oral Candida isolates in patients undergoing radiotherapy for head and neck cancer: prevalence, azole susceptibility profile and response to antifungal treatmentOral Microbiol Immunol 2004 19:347-51. [Google Scholar]
[18]. Redding SW, Bailey CW, Lopez JL, Kirkpatrick WR, Fothergill AW, Renaldi MG, Candida dubliniensis in radiation induced oral pharyngeal CandidiasisOral Surg Oral Med Oral Pathol 2001 91:659-62. [Google Scholar]
[19]. Dahiya MC, Redding SW, Dahiya RS, Eng TY, Kirkpatrick WR, Coco BJ, Oropharyngeal Candidiasis caused by non-albicans yeast in patients receiving external beam radiotherapy for head and neck cancerInt J Radiat Oncol Biol Phys 2003 57:79-83. [Google Scholar]
[20]. Jham BC, Franca ES, Oliveria RR, Santos VR, Kowalski LP, Freire AR, Candida oral colonization and infection in Brazilian patients undergoing head and neck radiotherapy: a pilot studyOral Surg Oral Med Oral Pathol 2007 103:355-58. [Google Scholar]