An Unusual ST Elevation in a Case of Left Atrial Myxoma
Nikunj Vyas1, Ravi Ghatanatti2, Amrutraj Nerlikar3, Mohan Gan4, Mahadev Dixit5
1 Senior Resident, Department of CTVS, KLE’S Dr Prabhakar Kore Hospital and Medical Research Center, Belagavi, Karnataka, India.
2 Consultant, Department of CTVS, KLE’S Dr Prabhakar Kore Hospital and Medical Research Center, Belagavi, Karnataka, India.
3 Consultant, Department of CTVS, KLE’S Dr Prabhakar Kore Hospital and Medical Research Center, Belagavi, Karnataka, India.
4 Consultant, Department of CTVS, KLE’S Dr Prabhakar Kore Hospital and Medical Research Center, Belagavi, Karnataka, India.
5 Consultant, Department of CTVS, KLE’S Dr Prabhakar Kore Hospital and Medical Research Center, Belagavi, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nikunj Vyas, Senior Resident, Department of CTVS, KLE’S Dr Prabhakar Kore Hospital and Medical Research Center, Belagavi, Karnataka, India.
E-mail: nikk110986@gmail.com
Myxomas are the most common and potentially dangerous benign tumours of the heart. They may have either smooth or papillary surfaces and may have thrombus adherent. As both the papillary excrescences and the surface thrombi are friable in nature hence may undergo embolization. We report a case of left atrial myxoma, which underwent excision of the tumour for mitral valve obstructive features. In the immediate postoperative period patient developed ST elevation in lead II, III and aVF. Coronary angiogram revealed normal coronary pattern. Patient was treated with aspirin, heparin and IABP for 48 hours and recovered well. We conclude that there is a tendency for spontaneous recanalization of the obstructed coronary vessels by tumour emboli, hence patient can be managed conservatively.
Benign tumour, Coronaries, Emboli, ECG
Case Report
A 35-year-old female patient presented to cardiothoracic surgery department with complains of dyspnea on exertion (NYHA class III) since three months. There were no embolic events in the past. On examination patient had tachypnea and tachycardia. Auscultation revealed mid-diastolic murmur in mitral area. ECG was suggestive of left atrial enlargement and atrial fibrillation. Further work up was done to differentiate rheumatic mitral disease from left atrial (LA) myxoma as a cause for mitral stenosis. Transesophageal echocardiography (TEE) showed large pedunculated myxoma attached to inter atrial septum, measuring 3.8*3.3cm. It protruded into left ventricle through the mitral valve (MV) causing obstruction to MV inflow [Table/Fig-1].
LA myxoma attached to interatrial septum with mitral valve inflow obstruction.
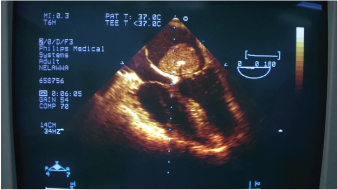
Peak pressure gradient of 32mmHg, tricuspid regurgitation with mitral regurgitation grade I, severe pulmonary artery hypertension and good biventricular function. CAG revealed normal coronary pattern. Provisional diagnosis of LA myxoma was made and informed written consent was taken for the surgery.
The patient underwent elective LA myxoma excision with intact tumour under cardiopulmonary bypass support through right atrial approach. The septal defect was closed with autologous pericardium. Postoperative TEE showed good biventricular function after weaning off from cardiopulmonary bypass. She developed ST elevations in lead II, III and aVF. Postoperative coronary angiogram was done suspecting tumour emboli to coronaries but was normal. The patient remained haemodynamically unstable & she was treated with aspirin 75mg, heparin to maintain activated clotting time between 150-180 sec and intra-aortic balloon pump (IABP) support. She made good haemodynamic recovery within next 48 hours without any neurologic deficits. Patient was discharged on 10th postoperative day. Follow up after a month with echocardiography suggested normally functioning mitral valve with mild pulmonary artery hypertension and NYHA class improved from class III to I.
Discussion
Myxomas are the most common and potentially dangerous benign tumours of the heart. Approximately 75% atrial myxoma’s arise in LA and systemic embolization occurs in 30-50% cases [1–3]. Women are most commonly affected in their 3rd -5th decade. Most cases are sporadic but about 7% have family history. Surgical treatment is the main stay of treatment and they rarely recur.
Patients with atrial myxomas may present with valve obstruction, embolization to the pulmonary and systemic circulation, or constitutional symptoms. Left atrial myxomas have a higher propensity to embolize both pre and postoperatively [4]. Right atrial myxomas rarely display clinical manifestations of emboli. There is a risk of extensive haemorrhagic MI with tamponade [5] and tumour fragmentation with systemic embolization [6], if thrombolysis is performed in an undiagnosed left atrial myxoma causing MI. Our patient presented with mitral valve obstruction features with no signs of systemic embolization.
Most atrial myxoma cases make uneventful recovery after excision except a few show systemic embolization. Careful handling of the heart and intact removal of the tumour is advocated during surgery. Inspite, systemic and coronary embolization is reported in 30-50% and 0.06% cases respectively [1–3,7]. When coronary occlusion with tumour tissue occurs, percutaneous coronary artery intervention or CABG may be needed [8].
Our patient developed ST elevations in lead II, III and aVF and no cardiac enzyme elevation was seen in immediate postoperative period. The reason for such an observation could be that the tumour emboli may have caused subtotal occlusion of coronaries giving rise to ST changes. CAG was normal possibly due to lysis of the smaller fragments or spontaneous recanalization of the coronaries [9–11]. The patient made good recovery with IABP support, heparin and aspirin.
Similar case reporting was done by Yavuz and colleagues in which patient presented with features of myocardial infraction without risk factors for coronary artery disease. Echo showed left atrial myxoma and coronary angiogram was normal [12].
Braun in his review of 40 cases of MI due to left atrial myxoma found that the right coronary artery was the common culprit with inferior myocardial infarction seen in most of the cases [13]. In 33% of the documented coronary angiogram it was found to be normal.
Conclusion
Myxomas are the most common cause for ST changes in both pre & post op period. Coronary angiogram can show normal coronary pattern due to spontaneous recanalization or lysis of tumour thrombus.
[1]. Bortolotti V, Maraglino G, Rubino M, Surgical excision of intracardiac myxomas: A 20-year follow-upAnn Thorac Surg 1990 49:449-45. [Google Scholar]
[2]. Fyke FE, Seward JB, Miller FA, Primary cardiac tumours: Experience with 30 consecutive patients since introduction of two-dimensional echocardiographyJ Am Coll Cardiol 1985 5:1465 [Google Scholar]
[3]. Goodwin JF, The spectrum of cardiac tumoursAm J Cardiol 1968 21:307 [Google Scholar]
[4]. Meller J, Teichholz LE, Pickard AD, Left ventricular myxoma: Echocardiographic diagnosis and review of the literatureAm J Med 1977 63:816 [Google Scholar]
[5]. Tomita Y, Endo T, Takano T, Hayakawa H, Tamura K, Sugisaki Y, Extensive haemorrhagic myocardial infarction associated with left atrial myxomaCardiology 1992 81(6):384-88. [Google Scholar]
[6]. Abascal VM, Kasznica J, Aldea G, Davidoff R, Left atrial myxoma and acute myocardial infarction: a dangerous duo in the thrombolytic agent eraChest 1996 109(4):1106-08. [Google Scholar]
[7]. Lehrman KL, Prozan GB, Ullyot D, Atrial myxoma presenting as acute myocardial infarctionAmerican Heart Journal 1985 110(6):1293-95. [Google Scholar]
[8]. Demir M, Akpinar O, Acarturk E, Atrial myxoma: an unusual cause of myocardial infarctionTexas Heart Institute Journal 2005 32(3):445-47. [Google Scholar]
[9]. Rath S, Har-Zahav Y, Battler A, Coronary arterial embolus from left atrial myxomaAmerican Journal of Cardiology 1984 54(10):1392-93. [Google Scholar]
[10]. Hashimoto H, Takahashi H, Fujiwara Y, Joh T, Tomino T, Acute myocardial infarction due to coronary embolization from left atrial myxomaJapanese Circulation Journal 1993 57(10):1016-20. [Google Scholar]
[11]. Namazee MH, Rohani-Sarvestani HR, Serati AR, The early presentation of atrial myxoma with acute myocardial infarctionArchives of Iranian Medicine 2008 11(1):98-102. [Google Scholar]
[12]. Yavuz T, Peker O, Ocal A, Ibrisim E, Left atrial myxoma associated with acute myocardial infarctionInt J Cardiovasc Imaging 2005 21(2-3):235-38. [Google Scholar]
[13]. Braun S, Schrötter H, Reynen K, Schwencke C, Strasser RH, Myocardial infarction as complication of left atrial myxomaInt J Cardiol 2005 101:115-21. [Google Scholar]