Oral Submucous Fibrosis (OSMF) is a chronic fibrosing disease of the oral cavity which is characterised by fibroelastic change of the lamina propria and atrophy of epithelium causing trismus and inability to eat [1].
The term “atrophica idiopathica mucosa oris” was proposed by J. Schwartz in 1952 when he first described this disease in five Indian women from Kenya. In ancient medicine, Shusrutha described a similar condition as “VIDARI” under mouth and throat diseases. This condition was subsequently termed as “Oral Submucous Fibrosis (OSF)” by SG Joshi [2]. Goleria in 1970 proposed the term “subepithelial fibrosis”. Areca nut is considered to be the main etiological factor for oral submucous fibrosis. The most common clinical symptom is burning sensation of the oral mucosa which is aggravated by intake of spicy food. Xerostomia or hyposalivation is also common.
Increase in the rate of collagen synthesis and decrease in collagen degradation play a key role in the pathogenesis of OSMF. OSMF shows characteristic histopathological features like increased collagen fiber formation in the initial stages followed by dense collagen fiber bundles and different degrees of hyalinization, along with atrophic epithelium. Assessment of the severity of this disease is of paramount importance in treatment planning and can be done using clinical, functional and histopathologic criteria. The objective of the present study was to compare the clinical and functional staging with histopathologic staging methods used to assess the severity of OSMF. A qualitative analysis of the collagen fibres in various histopathologic stages of OSMF was performed using picrosirius red stain and polarising microscope.
Picrosirius red stain is specific for collagen and can be used to distinguish mature and immature fibers. It is considered superior to other dyes as it stains finer collagen fibrils intensely, is stable and does not fade easily [3]. It stains collagen by reacting via the sulphonic acid groups with the basic groups present in collagen. The long axis of elongated dye molecules is parallel to the long axis of collagen. The birefringency of collagen under polarising microscope is enhanced by the parallel relationship between collagen and the dye molecules, thereby enhancing the visibility of immature collagen fibrils [4].
Materials and Methods
The study sample comprised of 30 cases. The sample was divided into two groups. Group I comprised of OSMF samples (n=20) which were obtained from the archives of the Department of Oral Pathology, Faculty of Dental Sciences, Sri Ramachandra University, Chennai. Group II comprised of normal buccal mucosa tissue samples (n=10) obtained from patients who reported for minor oral surgical procedures like pericoronitis associated with impacted third molars. Prior informed consent was obtained from the patients. Ethical clearance for the study was obtained from the institutional ethical committee.
Archival samples with complete details regarding symptoms like burning sensation, habits, mouth opening parameters and clinical signs like presence of palpable fibrous bands were included in the study. Cases with insufficient data were excluded from the study. Two tissue sections of 4 micron thickness were obtained from each specimen.
One tissue section of each sample was stained with haematoxylin and eosin stain and the other with picrosirius red stain.
Clinical and functional staging of all the 20 OSMF cases were done according to the criteria given by Haider et al., [5]. Clinical staging was done based on the presence of palpable fibrous bands in various locations: Stage 1- Faucial bands only, Stage 2- Faucial and buccal bands, Stage 3- Faucial, buccal and labial bands. Functional staging was done based on extent of mouth opening and the categories include Stage A (mouth opening ≥ 20mm), Stage B (mouth opening between 11-19 mm) and Stage C (mouth opening ≤ 10mm) [5]. Mouth opening was evaluated by measuring the inter-incisal distance.
Haematoxylin and eosin stained sections were analysed under light microscope following which histopathological staging was done based on criteria given by Pindborg and Sirsat [1] [Table/Fig-1]. The Picrosirius Red stained slides were examined under polarising microscope for the different colours produced in the different stages of OSMF.
Histopathological grading of oral submucous fibrosis by pindborg and sirsat [1].
| Histopathological stage | Histopathological features |
|---|
| Very early | Finely fibrillar collagen, plump young fibroblasts, dilated blood vessels and acute inflammatory cell infiltrate chiefly polymorphonuclear leukocytes. |
| Early | Juxta-epithelial hyalinisation with collagen arranged in separate thick bundles. Moderate number of young fibroblasts; dilated and congested blood vessels with inflammatory infiltrate consisting of lymphocytes and few eosinophils. |
| Moderately Advanced | Moderately hyalinised collagen. Thickened collagen bundles separated by slight residual oedema. Fibroblastic response is less marked. Blood vessels are normal or compressed. Inflammatory infiltrate consists of lymphocytes and plasma cells. |
| Advanced | Complete hyalinisation with smooth sheets of collagen and absence of oedema. There are no separate bundles of collagen and it is devoid of fibroblasts. Blood vessels are completely obliterated and the inflammatory infiltrate is composed of lymphocytes and plasma cells. |
Statistical Analysis
Descriptive data which includes frequency and percentages were calculated for each group. The output data was ordinal in nature. The strength of association between the clinical and functional staging methods and histopathological grading methods were assessed by spearmans correlation coefficient. Correlation coefficient (r) revealed the strength of association. Correlation coefficient value r=0.7 to 1, –0.7 to –1 denoted strong association; r=0.5 to 0.7, –0.5 to –0.7 indicated moderate association and r=0.3 to 0.5, - 0.3 to -0.5 denoted weak association.
Results
The study included 30 tissue samples, which comprised of 20 OSMF cases and 10 normal tissues. There were 14 males and 6 females in the study group. The age range of the study group was 18 to 60 with a mean age of 26. The most common habit found was areca nut chewing.
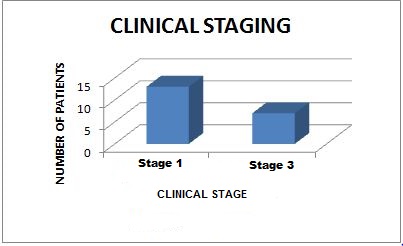
Clinical, functional and histopathological staging were done for all the 20 cases. In the clinical staging, it was found that, out of the 20 OSMF cases, 13 had faucial bands only, and seven had faucial, buccal and labial bands and hence were grouped under Stage one and stage three respectively. There were no cases which could be grouped under stage 2 [Table/Fig-2].
Distribution of study subjects (Clinical staging).
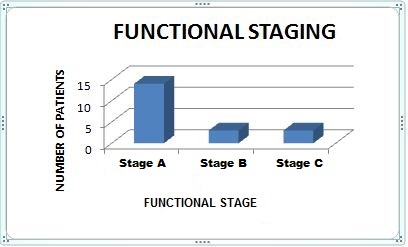
Functional staging was done based on mouth opening parameters. Mouth opening was estimated by measuring the inter-incisal distance. There were three groups depending on the degree of mouth opening namely, Stage A, B and C. There were 14 patients in stage A and three patients each in stage B and C [Table/Fig-3].
Distribution of study subjects (functional staging).
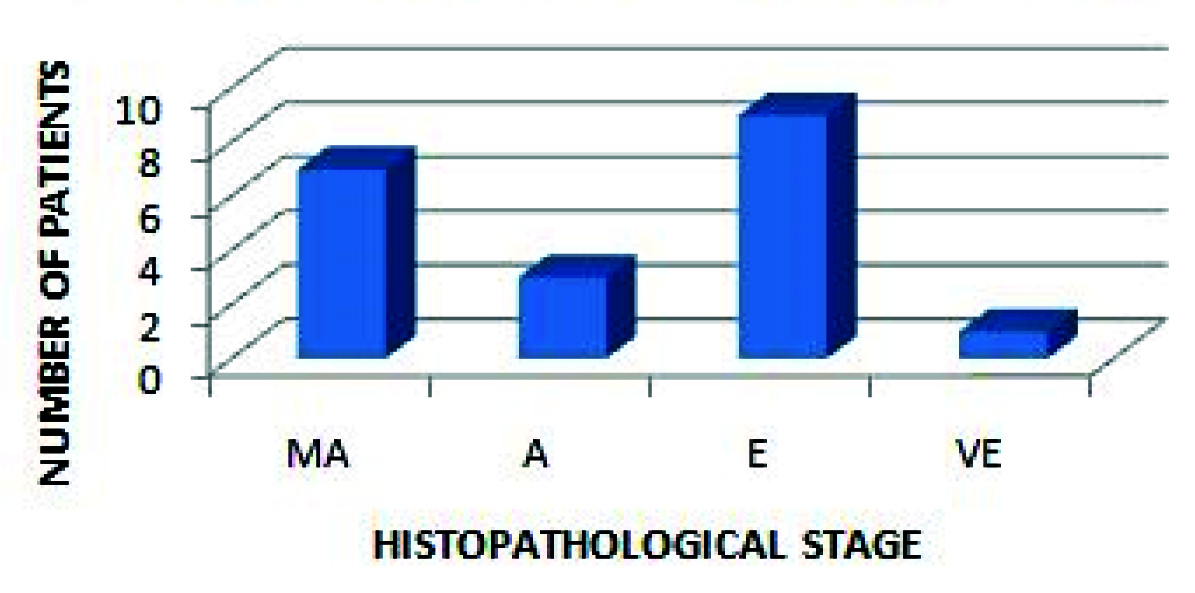
Histopathological staging was done based on the criteria given by Pindborg et al., [Table/Fig-1] [1]. There was one case in the very early stage, 9 cases in the early stage, seven in the moderately advanced stage and 3 in the advanced stage [Table/Fig-4,5a,6a,7a,8a].
Distribution of study subjects (Histopathological staging).
MA - Moderately Advanced, A - Advanced, E - Early, VE - Very Early
Very Early histopathological stage of OSMF (20x).
a - Haematoxylin and Eosin stained sections
b - Picrosirius red stained sections of OSMF under Polarising microscope exhibiting predominant yellowish green birefringence

Early histopathological stage of OSMF (20x).
a - Haematoxylin and Eosin stained sections
b - Picrosirius red stained sections of OSMF under Polarising microscope exhibiting predominantly yellowish birefringence

Moderately advanced histopathological stage of OSMF (20x).
a - Haematoxylin and Eosin stained sections.
b - Picrosirius red stained sections of OSMF under Polarising microscope exhibiting predominant orange-red birefringence

Advanced histopathological stage of OSMF (20x).
a - Haematoxylin and Eosin stained sections.
b - Picrosirius red stained sections of OSMF under Polarising microscope exhibiting predominant red birefringence

Clinical and functional staging was compared with histopathological staging. Functional staging revealed statistically significant correlation with histopathological staging of OSMF (P < 0.05). There was no correlation (p> 0.05) between clinical and histopathological staging methods [Table/Fig-9].
Comparision of clinical and functional stage with the histopathological grade of study subjects
| Type of staging | No. of cases | Histological Grading n(%) | Correlationco-efficient (r) |
|---|
| Clinical staging | Very Early | Early | Moderatelyadvanced | Advanced |
|---|
| I | 13 | 1 (7.9) | 5 (38.5) | 5 (38.5) | 2 (15.4) | 0.264* |
| II | 0 | 0 | 0 | 0 | 0 |
| III | 7 | 0 | 4 (57.1) | 2 (28.5) | 1 (14.3) |
| Functional Staging |
| A | 14 | 1 (7.1) | 9 (64.3) | 3 (21.4) | 1 (7.1) | 0.621** |
| B | 3 | 0 | 0 | 2 (66.6) | 1 (33.3) |
| C | 3 | 0 | 0 | 2 (66.6) | 1 (33.3) |
r=0.7 to 1, - 0.7 to -1 Strong association***; r=0.5 to 0.7, - 0.5 to -0.7 Moderate association**; r=0.3to 0.5, - 0.3 to -0.5 Weak association *
Examination of the picrosirius red stained OSMF sections under light microscope revealed characteristic arrangement pattern of the collagen fibers and fibrils which were distinct for each stage of OSMF. Collagen was stained red whereas epithelium and muscle took up yellow colour. Fibrillar collagen was clearly evident in the very early stages of OSMF with the picrosirius red stain. Early stage showed arrangement of collagen fibers in separate bundles. Moderately advanced cases showed thicker collagen bundles with moderate hyalinization Advanced cases of OSMF displayed smooth sheets exhibiting complete hyalinization. The arrangement of collagen fibers in different stages of the disease appears similar in both picrosirius red and haematoxylin & eosin stained sections. However, the pattern was clearly appreciated in Picrosirius Red stained sections compared to the conventional haematoxylin and eosin stained sections as the finer collagen fibers are more intensely stained by picrosirius red.
Polarising colours of collagen fibers in 20 cases of OSMF patients were compared with those of 10 cases of the control group. Enhanced birefringence of the collagen fibers due to picrosirius red stain yielded characteristic prominent polarising colours in different stages of OSMF. Normal tissues exhibited a predominant green colour. The very early and early cases of OSMF exhibited a predominant greenish yellow colour under polarising microscope [Table/Fig-5b,6b]. A shift towards orange red to red colour was observed in the moderately advanced and advanced cases of OSMF [Table/Fig-7b,8b].
Discussion
OSMF is a potentially malignant disorder of oral mucosa. The condition is common in India with a prevalence of 6.42% [6,7]. OSMF results from increased production of collagen by fibroblasts. In addition to this, there is decreased breakdown, leading to accumulation of excessive amounts of collagen. This results in juxta-epithelial inflammatory reaction and fibrosis in the oral mucosa [8]. Various biological mechanisms have been considered in the pathogenesis of OSMF with increased lysyl oxidase activity being the most important [9]. Lysyl oxidase is a copper dependant enzyme implicated in cross-linking of collagen fibers [10]. The key pathogenetic process in OSMF is altered collagen metabolism. The initial stages of the condition is characterized by excessive deposition of collagen fibers and the advanced stages show dense collagen fiber bundles exhibiting varying degrees of hyalinization [11].
Comparison of clinical (presence of palpable fibrous bands, Haider et al.,), functional (extent of mouth opening, Haider et al.,) and histopathological methods (Pindborg et al.,) used to stage OSMF revealed that functional staging with histopathologic staging was more reliable than clinical staging in reflecting the severity of the disease [1,5]. The results of our study was in accordance with studies by Ceena et al., and Modak N et al., who also observed a significant correlation between functional and histopathologic staging [3,12]. Kiran Kumar et al., also observed that there was no direct correlation between clinical stages and histopathologic grading which he attributed to the possibility of difference in the severity and extent of fibrosis in different regions of the oral mucosa and involved muscles [11].
The traditional stains like van gieson and trichrome stains rely on differential binding by tissue components which in turn is determined by various factors like relative size of the dye, the physical structure of the tissue and aminoacid composition of tissue elements. Hence, these stains may not be ideal for collagen detection due to lack of selectivity. A major disadvantage of these stains is their lack of ability to reveal very thin collagen fibers and thereby result in substantial underestimation of collagen content. The tendency of these stains to fade and their inability to detect very thin collagen fibrils urged Puchtler and colleagues to seek a better method for collagen detection [13]. The Picrosirius red stain is a strong anionic dye, specific and sensitive for collagen and gives a characteristic red colour to the collagen. It stains collagen by reacting via its sulphonic groups, with the basic groups present in the collagen molecule [4]. Hence, the characteristic arrangement patterns of the collagen in different stages of OSMF were clearly appreciated with this stain as compared to the conventional staining method.
Further, this stain when used in combination with Polarising microscopy, selectively demonstrates collagen fibers. The use of this microscopy increases the method’s sensitivity and resolution. Polarising microscope is a specialised microscope which uses polarised light (light waves in the same vibration direction). Different Polarising colours were produced depending on the thickness and density of collagen. This can be attributed to the fact that the elongated dye molecules of the stain are attached to the collagen fiber in such a way that their long axes are parallel. This parallel relationship results in an enhanced birefringency [14]. The fact that thin fibers produce green to yellowish- green colours and thick fibers produce orange-red to red colours of longer wavelengths under polarising microscope is well known from previous studies [15]. It is also stated that green to greenish yellow colours suggest that the collagen is thin and orange red colour denotes tight packing of fibers [12,15,16]. In our study, the moderately advanced stages and advanced stages showed an orange red to red colour, while the early stages showed predominant greenish yellow colour as observed by Ceena DE et al., Modak N et al., and Velidandla S et al., [3,12,16]. This could be attributed to the presence of poorly packed thinner collagen fibrils in the early stages and increased number and tight packing of thick collagen fibers in the advanced stages of this condition.
Conclusion
Comparison of functional staging with histopathologic grading is more reliable in determining the severity of the disease than the clinical staging. Production of characteristic polarising colours by various stages of picrosirius red stained sections of OSMF substantiates the use of picrosirius red stain and polarising microscope as a tool in assessing the severity of this condition thereby aiding in better treatment planning.
Since oral submucous fibrosis is a potentially malignant condition, early recognition with accurate staging of the disease and appropriate treatment planning is of utmost importance to prevent the malignant transformation and to improve the quality of life of the patient.
r=0.7 to 1, - 0.7 to -1 Strong association***; r=0.5 to 0.7, - 0.5 to -0.7 Moderate association**; r=0.3to 0.5, - 0.3 to -0.5 Weak association *