The evaluation of the patient who has liver disease in order to arrive at a definitive diagnosis and management plan requires careful clinical assessment and the use of various investigations. The analysis of the information obtained also allows an assessment of severity of the disease and the prognosis for the patient [6]. 5’-Nucleotidase (5’-ribonucleotide phosphohydrolase; EC 3.1.3.5; 5’-NT), an intrinsic membrane glycoprotein present as an ectoenzyme in a wide variety of mammalian cells, catalyzes hydrolysis of 5-nucleotides to their corresponding nucleosides [7,8]. 5’-NT was described in heart and skeletal muscle about 60 years ago [9]. Dixon and Purdon first observed that serum 5’-NT was clinically useful for differential diagnosis of hepatobiliary and osseous diseases; the enzyme activity being increased only in hepatobiliary diseases [10]. Raised levels of 5’-nucleotidase activity were found in patients with obstructive jaundice, parenchymal liver disease, hepatic metastases and bone disease. Moreover, 5’-nucleotidase is a precise marker of early hepatic primary or secondary tumors [11]. 5’-Nucleotidase was superior to alkaline phosphatase (ALP) as far as its sensitivity & specificity is concerned [12]. Increased 5’-NT in the serum of patients with normal ALP identified with high probability the presence of liver disease, confirming that any increase in 5’-NT activity that is more than marginal is highly specific for hepatobiliary disease, at least in patients with increased ALP [8].
In recent years 5’-NT is merely among routine examination of liver related disease. Present case-control study was conducted to find the comparative level of 5’-NT among patients with Viral Hepatitis, Alcoholic Liver disease and liver cirrhosis.
Materials and Methods
Study Design: Perspective, case- control study.
Study site: Gandhi Medical College, Hyderabad, India.
Selection of study subjects: In this study 60 male subjects (15 healthy controls and 45 cases) included, aged between 30 -50 years were included. The cases were divided into three groups based on clinical and histopathological examination. Each case group consisted of 15 male age- matched subjects suffering from either viral hepatitis, alcoholic liver disease (more than 10 years.) or liver cirrhosis. All cases were the patients admitted to Gastroenterology unit in Gandhi Hospital, Secunderabad and Owaisi Hospital Hyderabad, India. Inclusion criteria for selection of healthy controls were apparently healthy without any history of alcohol intake, liver disease, any other chronic disease, recent illness and medication.
Ethical consideration: Ethical approval was obtained and the institutional guidelines were followed.
Blood sample collection and laboratory analysis.
Blood sample (5ml) was collected in a plain vial in aseptic condition from each subject. Serum was separated after allowing the blood samples to clot at room temperature for 45 minutes and centrifugation was done at 3000 rpm for 10 minutes. The activity of 5’-NT was assayed on haemolysis free sera.
Estimation of 5’-nucleotidase level by colorimetric method of Campbell (1962) [13,14] A 5’-NT hydrolyses nucleotides with phosphate group on carbon atom of ribose i.e. adenosine 5 phosphate which hydrolyzed to adenosine and inorganic phosphate. These nucleotide are hydrolyzed also by nonspecific phosphatase such as alkaline phosphatases. However, 5’-NT is inactivated by nickel, so that if the hydrolysis is carried out with and without added Nickel, the difference give the 5’-NT activity. Magnese ions are included as the activator.
For the determination of 5 NT two test tubes were set up as follows:
A) Total activity: 0.2 mL of serum was taken, then 0.1 mL of 0.02M manganous sulfate and 1.5 mL of 40 mM, pH 7.5 barbitone buffer were added.
B) Non-specific ALP activity: 0.2 mL of serum was taken, then 0.1 mL of 0.02 M manganous sulfate, 1.3 mL of 40 mM, pH 7.5 barbitone buffer and 0.2 mL of 0.1M nickel chloride were added.
Test tubes warmed to 37 °C, then 0.2 mL 10mM adenosine 5’-phosphate were added to each test tube and kept for incubation at 37°C for 30 minutes. Then 2 mL of 10% trichloroacetic acid (TCA) were added, mixed well, allowed to stand and centrifuged to take 2ml of supernatant.
For the blank and standard 1 mL of water and 1 mL of the phosphate standard (stock solution containing 6 mmol/L) were taken further, to each 1 mL of TCA added. To all four tubes 3 mL Reagent C {2M, pH 4.0 acetate buffer, 0.5 mL of 5% ammonium molybdate and 0.5 mL metol (2 g metol and 10g sodium sulfite in water made up to 100 mL)} mixed, allowed to stand for 10 minutes and then read at 680 nm.
Calculation
5’-NT activity in U/L= (A-B/STD)*0.0516/0.1*1000*1/30
Statistical Analysis
Statistical analysis was done using SPSS for Windows version 17.0. Results were expressed as (Mean ±SD). Comparison of variables between two groups performed with student t-test for continuous variables. The p-values < 0.05 were considered statistically significant.
Results
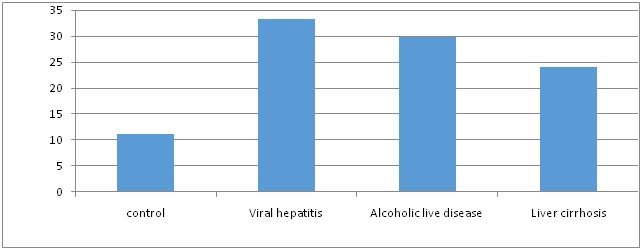
Serum 5’-NT levels were significantly raised in viral hepatitis, alcoholic liver disease and cirrhosis patients. The levels were 35.2±8.43, 29.87 ±3.94, and 24.07± 4.33 respectively when compared to healthy controls (11.2±3.42) U/L.
The [Table/Fig-1] demonstrated significant differences (p<0.001) between the studied cases groups and each case group compared to the control group. The [Table/Fig-2] shows that the level of 5’. NT was the highest among the viral hepatitis group, followed by alcoholic group, and then between cases in liver cirrhosis group.
“5’-NT” in Controls, viral hepatitis, alcoholic liver disease and liver cirrhosis subjects.
| Mean±SD | p1 | p2 | p3 |
|---|
| Control(n=15) | 11.2±3.42 | | | |
| Viral hepatitis(n=15) | 35.2±8.43 | <0.001 | | |
| Alcoholic liver disease(n=15) | 29.87 ±3.94 | <0.001 | <0.001 | |
| Liver cirrhosis(n=15) | 24.07± 4.33 | <0.001 | <0.001 | <0.001 |
p-value 1 comparing patients with viral hepatitis, alcoholic liver disease and liver cirrhosis to healthy controls.
p-value 2 comparing patients with alcoholic liver disease to liver cirrhosis and viral hepatitis.
p-value 3 comparing patients with liver cirrhosis to alcoholic liver disease.
*p<0.05 significant
Serum 5 nucleotidase levels in viral hepatitis, alcoholic liver disease and liver cirrhosis and healthy controls.
Discussion
The liver is the largest organ in the body and serves many vital functions such as remove damaged red blood cells from the blood in co-ordination with spleen, produces bile, clotting factors, stores vitamins, minerals, protein, fats and glucose from diet [15]. Disease of liver and biliary tract always calls for determination of liver enzymes as opposed to other parameters [16]. Since the liver performs a variety of functions so no single test is sufficient to provide complete estimate of its function [17]. Elevation of 5’-NT is reported in various disease [18]. The serum elevation of 5’-NT resembles that of ALP. However, 5’-NT elevations persist longer than ALP. Osteoblastic bone disease does not cause elevated levels of 5- nucleotidase. Thus, when serum ALP is increased the usual interpretation is that either cholestatic liver disease or osteoblastic bone disease is present. The determination of 5’-NT is useful to differentiate cholestatic liver disease from osteoblastic bone disease [19]. This makes 5’-NT more useful as compared to ALP for evaluation of obstructive biliary diseases. This advantage coupled with the fact that 5’-NT has shown a significant rise in anicteric biliary disease patients and ALP has not shown any such significant rise, shows the usefulness and superiority of this enzyme over ALP as a diagnostic tool in evaluation of such biliary disease patients [20]. It is measured as an indicator of liver damage resulting primarily from interference with the secretion of bile. The diagnostic value of 5’-NT has been shown to be superior to other liver enzymes, especially in liver metastasis. Raised levels of 5’-NT activities are found in 92% of patients with obstructive jaundice, 70% of patients with parenchymal liver disease and 81% of patients with hepatic metastasis [21]. The study result reflects that serum 5’-NT is raised in all case groups’ viral hepatitis, alcoholic liver disease and Liver cirrhosis in comparison of healthy controls [Table/Fig-2]. Subhani et al., found that serum 5’-NT levels were higher among alcoholic consumers than cirrhotic groups [14]. In another study Pratibha et al., observed higher levels of serum 5’-NT inacute infective hepatitis patients [22]. In our study we have found comparatively the serum 5’-NT levels were highest in viral hepatitis than Alcoholic liver disease and Liver cirrhosis, moreover a significant differences was observed between alcoholic liver disease and liver cirrhosis groups. While Raghvendra et al., reported highest level among infective hepatitis patients than alcoholic hepatitis and liver cirrhosis, but there was no significant difference was observed between alcoholic hepatitis and liver cirrhosis patients [23]. One recent study reported higher level of serum 5’-NT in chronic hepatitis C than Alcoholic patients [24].
Limitation
The small sample size, needed a more subjects and for longer period was limitation of the study.
Conclusion
Comparatively among the groups, highest value was observed among viral hepatitis than Alcoholic liver diseases than liver cirrhosis as compare to healthy control. Serum 5’-NT showed elevations in mean value of three fold in viral hepatitis, 2.5 folds elevation in alcoholic liver disease and two fold in cirrhosis. It is worth to estimate the serum 5’-NT, could be clinically useful for differential diagnosis of hepatobiliary diseases and its degree of involvement.
Conflict of interests: The authors declare that they have no conflict of interests.
p-value 1 comparing patients with viral hepatitis, alcoholic liver disease and liver cirrhosis to healthy controls.
p-value 2 comparing patients with alcoholic liver disease to liver cirrhosis and viral hepatitis.
p-value 3 comparing patients with liver cirrhosis to alcoholic liver disease.
*p<0.05 significant