Persistent Mullerian Duct Syndrome with Embryonal Cell Carcinoma along with Ectopic Cross Fused Kidney
Arun Kumar Barad1, NR Manju Bharath2, V Narayana3, V Om Pramod Kumar Raja4, Pranav Reddy Jambula5
1 Assistant Professor, Department of General Surgery, Vydehi Institute of Medical Sciences and Research Center, Bangalore, Karnataka, India.
2 Assistant Professor, Department of General Surgery, Vydehi Institute of Medical Sciences and Research Center, Bangalore, Karnataka, India.
3 Professor and Unit Chief, Department of General Surgery, Vydehi Institute of Medical Sciences and Research Center, Bangalore, Karnataka, India.
4 Junior Resident, Department of General Surgery, Vydehi Institute of Medical Sciences and Research Center, Bangalore, Karnataka, India.
5 Junior Resident, Department of General Surgery, Vydehi Institute of Medical Sciences and Research Center, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Arun Kumar Barad, Assistant Professor, Department of General Surgery, VIMSRC, #82 EPIP Area, Whitefield, Bangalore-560 066, Karnataka, India. E-mail : arunkumarb23@gmail.com
Persistent Mullerian Duct Syndrome (PMDS) is a form of internal male pseudohermaphroditism, where there is normal development of male secondary sexual characters, along with the presence of bilateral fallopian tubes and uterus. Majority of these cases go undetected and some cases are accidentally diagnosed while investigating for other problems. Cross fused renal ectopia is a condition where one kidney lies in the opposite side, fused to the other kidney. We present an extremely rare case of a phenotypical male presenting with mass per abdomen and bilateral cryptorchidism, turned out to have uterus with bilateral fallopian tubes, ectopic cross fused right kidney and Embryonal cell carcinoma of left undescended testis.
Anti-Mullerian Hormone (AMH), Cryptorchidism, Male pseudohermaphroditism
Case Report
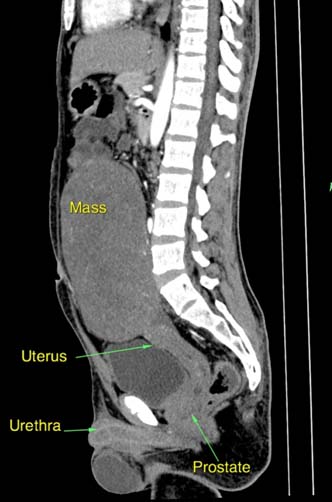
A 20-year-old unmarried male patient presented with a mass per abdomen noticed since 3 years, along with vague pain abdomen. The mass was gradually increasing in size, with a rapid increase noted over the past 6 months. There was no history of bowel and bladder disturbances. He also gave a history of absence of left testis since birth, but did not have a medical consultation for the same. Examination revealed a non-tender mass occupying the umbilical and suprapubic regions, 18x12cm in size. Both the testes were not palpable, but in the right scrotum a small fluid filled sac was palpable which the patient thought was testis. A working diagnosis of tumour of undescended testis was made and the investigative work up was initiated. Ultrasonography findings were ambiguous and only revealed a midline mass with ectopic cross fused right kidney. Computed tomography revealed a large pelvi-abdominal mass with a uterus, bilateral fallopian tubes, and cross fused renal ectopia on the right [Table/Fig-1,2]. These findings were confirmed with MRI. Computed tomography of chest was done as a part of metastatic work up and was found to be normal. Micturating cystourethrogram did not reveal any patent communication between the uterus and the urinary tract. Hormonal and tumor marker study revealed a raised Luteinizing Hormone (LH=9.25mIU/ml, Normal=0.7-7.4mIU/ml), beta-Human Chorionic Gonadotropin (58.92 IU/L, Normal= <5 IU/L) and CA125 (85.3 U/ml, Normal= <35U/ml), rest were within normal limits. Semen analysis showed azoospermia. All the other routine investigations were within normal limits.
Sagittal CT image showing the testicular mass with uterus.
Cross sectional view showing the cross fused right kidney.

On exploratory laparotomy, a large mass (16x10x5cm) was found along with the uterus and bilateral fallopian tubes. An atrophic intra-abdominal right testis was also noted [Table/Fig-3,4]. The left testicular mass was excised along with hysterectomy, bilateral salphingectomy and right orchiopexy was done. The upper and lower poles of the right testis were biopsied as well. The postoperative period was uneventful. Histo-pathological examination revealed embryonal carcinoma of the left testis, not involving epididymis and spermatic cord. Uterus showed hyperplasia of endometrium. There was no evidence of ovo-testis in testicular biopsy. Right testis had atrophic changes with no evidence of malignancy [Table/Fig-5]. Patient is now on adjuvant chemotherapy (bleomycin, etoposide and cisplatin).
Image showing the testicular tumour being removed.
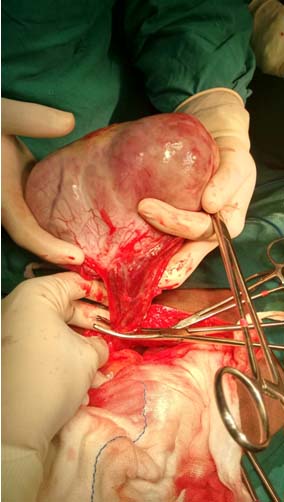
Image showing the uterus in situ and after excision.

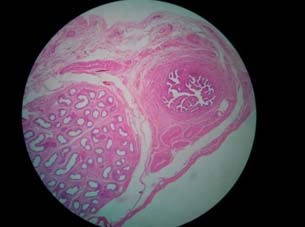
Histopathological slide showing fallopian tube and the vas defferentia together.
Discussion
Persistent Mullerian Duct Syndrome (PMDS) is a form of internal male pseudohermaphroditism with normal male phenotype. In addition to normal development of male secondary sexual characters, they also have bilateral fallopian tubes and uterus. It is known to occur due to failure of secretion of Anti-Mullerian Hormone (AMH), also called as Mullerian inhibiting factor, by Sertoli cells [1].
PMDS was first described by Nilson in 1939 [2]. There are ~262 cases reported in the literature so far [3]. The incidence of PMDS appears to be far more exceeding than what is apparent, due to the possibility of having been overlooked before the laparoscopic era. Even today in the laparoscopic era there is a high possibility of overlooking this condition which may be attributed to lack of clinical suspicion of PMDS in cases of pediatric cryptorchidism, which in turn may be due to less awareness about the condition among clinicians.
The exact cause of PMDS is not known. Deficiency of the anti-Mullerian hormone or failure of the Mullerian ducts to respond to its secretion may cause this condition. The gene responsible for AMH is localized on the short arm of chromosome 19 [4]. Both Mullerian and Wolffian ducts (mesonephric ducts) are present at 7 weeks of gestation in a fetus [1]. Thereafter, in a XY fetus testis differentiates to produce testosterone, which drives Wolffian duct differentiation into epididymis, vas deferentia and seminal vesicles. Meanwhile, sertoli cells produce anti mullerian hormone leading to the regression of the mullerian ducts [5]. Patients with PMDS are often asymptomatic and discovered incidentally either during imaging or intraoperatively. Usually, an investigation for cryptorchidism or abdominal mass reveals the presence of PMDS, as in our case.
The overall incidence of malignancy in an ectopic testis is known to be 15%, more for the abdominal testis than the inguinal one. The risk remains same for the patients of PMDS with ectopic testis. Our review of literature has revealed ~30 cases of malignancies in patients with PMDS. Majority of the tumours were arising from the ectopic testis, with a few cases of malignancies in mullerian duct remnants. Testicular tumours encountered were seminomas, embryonal cell carcinoma, yolk sac tumour and teratomas. Seminomas were the commonest [6]. However, in our case it was an embryonal cell carcinoma of the left intra-abdominal testis presenting as mass per abdomen, which led to the accidental finding of PMDS and cross fused renal ectopia on the right. Embryonal cell carcinoma of testis is a type of non-seminomatous germ cell tumour. It is a relatively rare testicular tumour occurring at a young age, the average being 31 years.
Cross fused renal ectopia is known to result from the abnormal development of the ureteric bud and metanephric blastema during the fourth to eighth weeks of gestation. It is the second most frequent fusion abnormality of the urinary tract. Left to right crossover with fusion of upper pole of the crossed ectopic kidney to the lower pole of the normally located kidney is the most frequent occurrence [7]. Similar was the situation in our case. These malformations are known to be associated with symptoms related pyelonephritis, hydronephrosis and urolithiasis. However, in our case there was no history of renal infections or stones. Association of this renal malformation with PMDS, as in our case, makes it imperative to think about the presence of a possible unknown common factor which may be influencing these abnormalities during the fetal growth. Further genetic and molecular studies are required in this regard. To the best of our knowledge, this is the first reported case of PMDS with cross fused renal ectopia.
As far as the management is concerned, it is advised to remove the mullerian duct structures because of the risk of malignancies they carry [8]. The close relation between the vas deferentia and the uterus has always posed as a challenge in many cases. In our case it was closely dissected to maintain the integrity of the testis. A right sided orchiopexy was done. Even though the patient had atrophic testis and azoospermia on semen analysis, it was imperative to save it for the testosterone production and virilisation.
Conclusion
We would like to suggest that a high index of suspicion for PMDS should be kept in all the cases of cryptorchidism and suitably investigated with ultrasonography or the diagnostic laparoscopy. Also, awareness of PMDS among the primary care physicians is imperative for the prompt detection and management of the condition.
[1]. Speroff L, Glass HR, Kase NG, The uterusIn: Clinical Gynecologic Endocrinology and Infertility 1994 5th ednBaltimore, MDWilliams & Wilkins:130-31. [Google Scholar]
[2]. Nilson O, Hernia uteri inguinalisbeim ManneActa Chir Scand 1939 83:231 [Google Scholar]
[3]. Shalaby MM, Kurkar A, Zarzour MA, Faddan AA, Khalil M, Abdelhafez MF, The management of the persistent Müllerian duct syndromeArab J Urol 2014 12:239-44. [Google Scholar]
[4]. Josso N, Belville C, di Clemente N, Picard JY, AMH and AMH receptor defects in persistantMullerian duct syndromeHum Reprod Update 2005 11(4):351-56. [Google Scholar]
[5]. Dekker HM, De Jong IJ, Sanders J, Rienhart FEW, Persistent Mullerian duct syndomeRadiographics 2003 23:309-13. [Google Scholar]
[6]. Berkmen F, Persistent Mullerian Duct Syndrome with or without transverse testicular ectopia and testis tumoursBr J Urol 1997 79:122-26. [Google Scholar]
[7]. Bauer BS, Anomalies of form and fusion, crossed renal ectopia with and without fusion. In: Alan J, editorWein: Campbell-Walsh Urology Book 2007 9th edPhiladelphiaWB Saunders:3269-304. [Google Scholar]
[8]. Farikullah J, Ehtisham S, Nappo S, Patel L, Hennayake S, Persistent Mullerian duct syndrome: lessons learned from managing a series of eight patients over a 10-year period and review of literature regarding malignant risk from the Mullerian remnantsBJU Int 2012 110:E1084-89. [Google Scholar]