An Evaluation of Upper and Lower Pharyngeal Airway Width, Tongue Posture and Hyoid Bone Position in Subjects with Different Growth Patterns
Jaipal Singh Tarkar1, Sandeep Parashar2, Garima Gupta3, Preeti Bhardwaj4, Raj Kumar Maurya5, Atul Singh6, Parul Singh7
1 Senior Lecturer, Department of Orthodontics, K.D. Dental College and Hospital, Mathura, India.
2 Reader, Department of Orthodontics, K.D. Dental College and Hospital, Mathura, India.
3 Reader, Department of Orthodontics, K.D. Dental College and Hospital, Mathura, India.
4 Associate Professor, Department of Orthodontics, K.D. Dental College and Hospital, Mathura, India.
5 Graded Specialist, Department of Orthodontics, Corps Dental Unit, Bhopal, India.
6 Reader, Department of Orthodontics, K.D. Dental College and Hospital, Mathura, India.
7 Post Graduate Student, Department of Orthodontics, K.D. Dental College and Hospital, Mathura, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raj Kumar Maurya, Corps Dental Unit, S I Lines, Military Station, Bhopal-462001, India.
E-mail: bracedbyraj@gmail.com
Introduction
It is important to evaluate the position of the hyoid bone in relation to the tongue at the beginning of orthodontic treatment so that during the treatment, its position may be directed hence overall impact on airway could be assessed.
Aim
The aim of this study was to evaluate the upper and lower pharyngeal airway dimensions, posture of tongue and hyoid bone position in young adults with different growth patterns.
Materials and Methods
Sample size of the study included 90 post-adolescent subjects, within the age range of 18-32 years. Based on the different growth pattern of the face, subjects were divided into Group I (n=30; average growth pattern), Group II (n=30; horizontal growth pattern) and Group III (n=30; vertical growth pattern). Lateral cephalogram were traced and analysed manually by the same investigator for evaluation of upper and lower pharyngeal airway, tongue posture and hyoid bone position. The intergroup comparison of upper and lower pharyngeal airway dimensions, posture of tongue and hyoid bone was performed with one-way ANOVA test.
Results
The results showed that upper oropharyngeal widths were significantly different in different facial skeletal patterns (p=0.00). Subjects with vertical skeletal pattern have significantly narrower upper airways than those with horizontal skeletal pattern (p= 0.025). There was significantly higher difference in position of dorsum of the tongue in vertical growth pattern group (p=0.00). The hyoid bone was positioned farther from the mandibular symphysis in brachyfacial subjects, reflected by the larger H-RGN (Hyoid- retrognathion) values compared with the dolichofacial and normal subjects (p=0.044).
Conclusion
The upper oropharyngeal width was found to be narrower in subjects with vertical growth pattern. The dorsum of the tongue is seen to be placed higher in subjects with vertical growth pattern. The hyoid bone was more inferiorly and posteriorly positioned in subjects with horizontal growth pattern. Variations are seen in upper and lower oropharyngeal widths, posture of the tongue and hyoid bone position in all the growth patterns.
Dolicocephalic, Oropharyngeal width, Retrognathion
Introduction
The pharynx is 12 to 14 cm, a tube-shaped anatomic organ formed by membranous and muscular tissues. It is divided into nasopharynx, oropharynx, and laryngopharynx. It is situated posterior to the oro-nasal cavities and the larynx. It starts from the cranial base and ends at the level of the sixth cervical vertebra and the lower border of the cricoid cartilage. Its length is approximately 12 to 14 cm, and it is divided into three parts [1].
The nasopharynx, forming the upper part of the respiratory system, is situated behind the nasal cavity and above the soft palate. Anteriorly, it is connected with the nasal cavity. Posteriorly, it continues downward as the oropharynx. Its main function is to facilitate respiration and deglution during normal physiologic process [1].
The hyoid bone is positioned above the level of the lower mandibular border in early human life which later with age, gradually descends to at the fourth cervical vertebra approximately. Its a unique bone as it remain suspended with attachment of ligaments and muscles Since it is not articulated with other bones, the position of the hyoid bone changes with body position, other physiologic states, head posture. Hyoid bone moves during various oral functions as such deglution and respiration in close association with tongue due to its attachment with genioglossus and geniohyoid muscle which intermigles with each other [2].
Due to infra hyoidale muscle and its attachment with scapular girdle, hyoid bone helps in maintainance of unobstructed airway during normal posture of head and neck [3].
The hyoid bone position and its corelation with the vertical growth pattern of the face is still in question [4]. Opdebeeck and associates [5] studied the position of the hyoid bone in patients with short face and long face syndrome and found out that movement of the hyoid bone changes with movement of the mandible, tongue, pharynx and cervical spine. He further concluded that the positions of the hyoid bone and the tongue can be considered as indicators of pharyngeal airway passage [4].
Thus it is important to evaluate the position of the hyoid bone in relation to the tongue at the beginning of orthodontic treatment so that during the treatment, its position may be directed hence overall impact on airway could be assessed. Therefore this retrospective study is designed and planned to measure the upper and lower pharyngeal airway dimensions, posture of tongue and hyoid bone position in young subject with different growth patterns.
Materials and Methods
Present study was performed retrospectively in Department of Orthodontics, K D Dental College & Hospital over the period of three months. The collected data contained cephalograms of 90 post-adolescent (males & females) subjects, within the age range of 18-32 years. The cephalographs were retrospectively selected based on the following inclusion criteria. All patients had Skeletal class I malocclusion with ANB between 1° and 3°, full complement of teeth up to 2nd molar, presence of Angle’s Class I molar relationship and Class I incisor relationship with normal overjet and overbite and pleasant soft tissue profile. There was no or minimum crowding of 2-3 mm among all selected patients. There was no history of orthodontic or orthognathic surgical treatment in past. Patients did not have any large restorations/carious lesions. Patients were exculded in presence of open bite (Anterior or lateral), history of (TMJ) problem, clenching or bruxism, congenital defect or deformed teeth and any history of trauma to the craniofacial region. All radiographs were digitized and traced on 0.003 inch acetate paper by same person.
The samples were divided into three groups. Group I consisted of 30 subjects with average growth pattern and Angle’s Class I normal occlusion. Group II consisted of 30 subjects with horizontal growth pattern and Angle’s Class I normal occlusion. Group III consisted of 30 subjects with vertical growth pattern and Angle’s Class I normal occlusion. Jarabak’s ratio (Posterior facial height/Anterior facial height x100), Sn-GoGn and FMA (FH-MP) parameters were used to divide the subjects into different growth pattern [6].
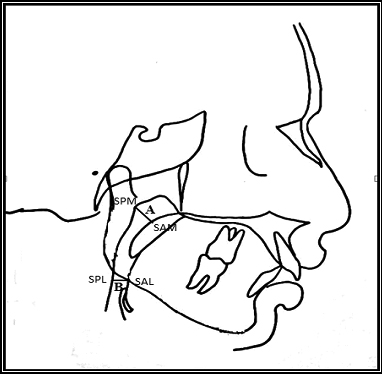
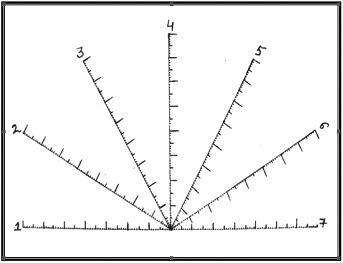
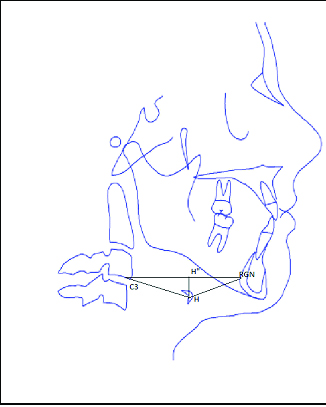
The cepahlometric landmarks and measurements for upper and lower pharyngeal airways were assessed according to McNamara analysis [Table/Fig-1,2] [7]. Tongue posture measurements used a template based on Rakosi analysis [Table/Fig-3] [8] and Hyoid bone position based on hyoid triangle analysis given by Bibby and Preston [Table/Fig- 4] [9].
Cephalometric landmarks and measurement.
| Variables | Definition |
|---|
| ULOPW(mm) | Upper and lower oropharyngeal airway |
| A(UOPW) | Upper oropharyngeal width |
| B(LOPW) | Lower oropharyngeal width |
| SPM | Point on posterior pharyngeal wall |
| SAM | Point on soft palate |
| SPL | Point on posterior pharyngeal wall |
| SAL | Point on tongue along the mandibular lower border |
| Hyoid bone position(mm) | Hyoid triangle by joining all the three point |
| C3 | The point at the most inferior anterior position on the third cervical vertebrae |
| RGN (retrognathion) | The most inferior post. Point on the mandibular symphysis. |
| H (hyoidale) | The most superior, anterior point on the body of the hyoid bone. |
| H 1 | Line perpendicular drawn from Hyoidale to C3-RGN |
| Tongue posture(mm) | Measurements using the template |
| Point 1 | Distance between the soft palate and the root of the tongue |
| Point 2-6 | Relationship of the dorsum of the tongue to the roof of the mouth |
| Point 7 | Position of the tip of the tongue relative to lower incisors |
Measurement of pharyngeal airway based on McNamara analysis.
Template used to measure tongue posture.
Hyoid triangle used to measure Hyoid bone position according to Bibby and Preston.
Results
Data were stastically analysed with SPSS (Version 17, SPSS, Chicago USA) to determine any significance of difference among the means of pharyngeal, hyoid bone and tongue postion.
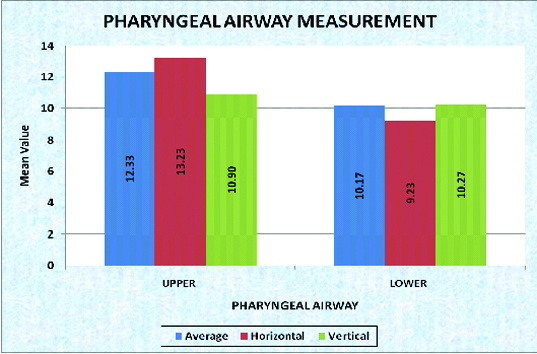
Pharyngeal Measurements: The mean value of the Upper Oropharyngeal Width (UOPW) for Group I was 12.33 mm (SD± 2.19 mm), Group II was 13.23 mm (SD± 2.16 mm) and Group III was 10.90 mm (SD± 1.92 mm) which was highly significantly different (p=0.00) however Lower Oropharyngeal width were found to be not significant (p= 0.158) [Table/Fig-5,6 and 7].
Mean SD± of upper and lower pharyngeal widths with in each group.
| Type | Growth Pattern | N | Mean | S.D. | Min. | Max. |
|---|
| UPPER PHARYNGEAL AIRWAY | Average | 30 | 12.33 | 2.19 | 10.00 | 19.00 |
| Horizontal | 30 | 13.23 | 2.16 | 10.00 | 17.00 |
| Vertical | 30 | 10.90 | 1.92 | 7.00 | 14.00 |
| LOWER PHARYNGEAL AIRWAY | Average | 30 | 10.17 | 2.83 | 5.00 | 16.00 |
| Horizontal | 30 | 9.23 | 1.61 | 7.00 | 12.00 |
| Vertical | 30 | 10.27 | 2.21 | 5.00 | 14.00 |
One-way ANOVA of upper and lower pharyngeal widths.
| One-way ANOVA |
|---|
| Type | Growth Pattern | N | Mean | S.D. | f-value | p-value | NS/S |
|---|
| UPPER PHARYNGEAL AIRWAY | Average | 30 | 12.33 | 2.19 | 9.49 | 0.000 | VHS |
| Horizontal | 30 | 13.23 | 2.16 |
| Vertical | 30 | 10.90 | 1.92 |
| LOWER PHARYNGEAL AIRWAY | Average | 30 | 10.17 | 2.83 | 1.89 | 0.158 | NS |
| Horizontal | 30 | 9.23 | 1.61 |
| Vertical | 30 | 10.27 | 2.21 |
p<0.001 is very highly significant (vhs), p<0.01 is highly significant (hs), p<0.05 is significant (s), p>0.05 is not significant.
Pharyngeal Airway Measurement.
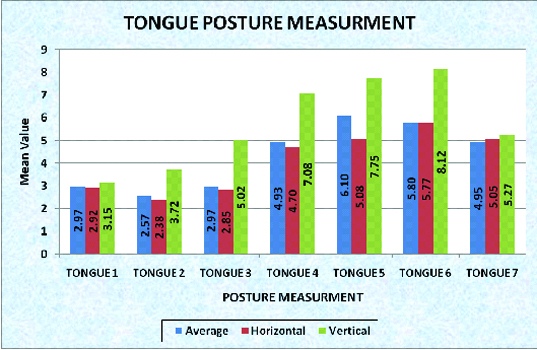
Tongue Measurements: The mean value of measurement at the posture of the dorsum of the tongue at Point 2 for Group I was 2.57 mm (SD± 0.93 mm), Group II was 2.38 mm (SD± 0.92 mm) and Group III was 3.72 mm (SD 1.01). The difference between the groups were found to be very highly significant (p=0.000). Similarly the mean value of measurement at the posture of the Dorsum of the tongue at Point 3 for Group I was 2.97 mm (SD± 1.10 mm), Group II was 2.85 mm (SD± 1.12 mm) and Group III was 5.02 mm (SD± 1.63) which showed that the difference between the groups were found to be very highly significant (p=0.000). The mean value of measurement at the posture of the Dorsum of the tongue at Point 4 showed highly significant difference amongs the mean (p=0.000) as the value for Group I was 4.93 mm (SD± 1.64 mm), Group II was 4.70 mm (SD± 1.97 mm) and Group III was 7.08 mm (SD 1.93). The mean value of the posture of the dorsum of the tongue at Point 5 for Group I was 6.10 mm (SD± 2.33 mm), Group II was 5.08mm (SD± 2.43 mm) and Group III was 7.75 mm (SD± 2.23) which was found to be highly significant different (p=0.000). The mean value at the posture of the Dorsum of the tongue at Point 6 for Group I was 5.80 mm (SD± 2.02 mm), Group II was 5.77 mm (SD± 3.02 mm) and Group III was 8.12 mm (SD± 1.84). The difference between the groups were found to be very highly significant (p=0.000). However the differences were not found to be significant at the Posture of the Dorsum of the Tongue at Point 1 (p=.755) and at the position of the tip of the tongue relative to the lower incisor at Point 7 (p=0.805) [Table/Fig-8, 9 and 10].
Mean SD± of tongue posture measurement with in each group Descriptive.
| Type | Growth Pattern | N | Mean | S.D. | Min. | Max. |
|---|
| TONGUE 1 | Average | 30 | 2.97 | 1.09 | 1.00 | 5.00 |
| Horizontal | 30 | 2.92 | 1.59 | 1.00 | 7.00 |
| Vertical | 30 | 3.15 | 1.04 | 1.00 | 5.00 |
| TONGUE 2 | Average | 30 | 2.57 | 0.93 | 1.00 | 5.00 |
| Horizontal | 30 | 2.38 | 0.92 | 1.00 | 4.00 |
| Vertical | 30 | 3.72 | 1.01 | 2.00 | 6.00 |
| TONGUE 3 | Average | 30 | 2.97 | 1.10 | 1.00 | 5.00 |
| Horizontal | 30 | 2.85 | 1.12 | 1.00 | 5.00 |
| Vertical | 30 | 5.02 | 1.63 | 3.00 | 9.00 |
| TONGUE 4 | Average | 30 | 4.93 | 1.64 | 2.50 | 8.00 |
| Horizontal | 30 | 4.70 | 1.97 | 1.50 | 9.00 |
| Vertical | 30 | 7.08 | 1.93 | 3.00 | 10.50 |
| TONGUE 5 | Average | 30 | 6.10 | 2.33 | 2.50 | 13.00 |
| Horizontal | 30 | 5.08 | 2.43 | 2.00 | 12.00 |
| Vertical | 30 | 7.75 | 2.23 | 4.00 | 12.00 |
| TONGUE 6 | Average | 30 | 5.80 | 2.02 | 3.00 | 12.00 |
| Horizontal | 30 | 5.77 | 3.02 | 3.00 | 16.00 |
| Vertical | 30 | 8.12 | 1.84 | 2.00 | 12.00 |
| TONGUE 7 | Average | 30 | 4.95 | 2.36 | 2.00 | 11.00 |
| Horizontal | 30 | 5.05 | 1.54 | 2.00 | 8.00 |
| Vertical | 30 | 5.27 | 1.70 | 2.00 | 8.00 |
One-way ANOVA of tongue posture measurement.
| Type | Growth Pattern | N | Mean | S.D. | f-value | p-value | NS/S |
|---|
| TONGUE 1 | Average | 30 | 2.97 | 1.09 | 0.28 | 0.755 | NS |
| Horizontal | 30 | 2.92 | 1.59 |
| Vertical | 30 | 3.15 | 1.04 |
| TONGUE 2 | Average | 30 | 2.57 | 0.93 | 17.36 | 0.000 | VHS |
| Horizontal | 30 | 2.38 | 0.92 |
| Vertical | 30 | 3.72 | 1.01 |
| TONGUE 3 | Average | 30 | 2.97 | 1.10 | 26.14 | 0.000 | VHS |
| Horizontal | 30 | 2.85 | 1.12 |
| Vertical | 30 | 5.02 | 1.63 |
| TONGUE 4 | Average | 30 | 4.93 | 1.64 | 15.08 | 0.000 | VHS |
| Horizontal | 30 | 4.70 | 1.97 |
| Vertical | 30 | 7.08 | 1.93 |
| TONGUE 5 | Average | 30 | 6.10 | 2.33 | 10.01 | 0.000 | VHS |
| Horizontal | 30 | 5.08 | 2.43 |
| Vertical | 30 | 7.75 | 2.23 |
| TONGUE 6 | Average | 30 | 5.80 | 2.02 | 9.84 | 0.000 | VHS |
| Horizontal | 30 | 5.77 | 3.02 |
| Vertical | 30 | 8.12 | 1.84 |
| TONGUE 7 | Average | 30 | 4.95 | 2.36 | 0.22 | 0.805 | NS |
| Horizontal | 30 | 5.05 | 1.54 |
| Vertical | 30 | 5.27 | 1.70 |
p<0.001 is very highly significant (vhs), p<0.01 is highly significant (hs), p<0.05 is significant(s), p>0.05 is not significant.
Tongue posture measurement.
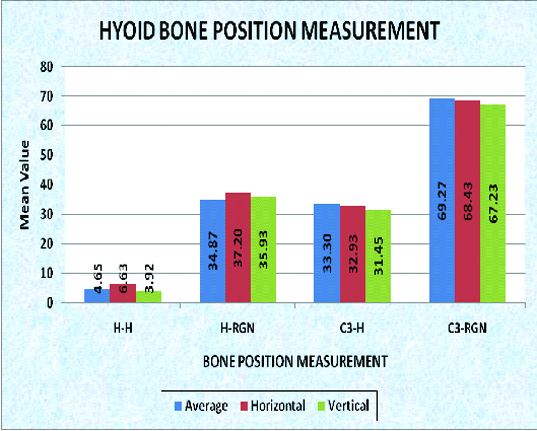
Hyoid bone measurement: The mean value for H-HI Group I was 4.65 mm (SD± 3.18 mm), Group II was 6.63 mm (SD± 4.32 mm) and Group III was 3.92 mm (SD± 2.59 mm). The differences between the groups were found to be highly significant (p=0.009). The mean value for H-RGN Group I was 34.87 mm (SD± 3.88 mm), Group II was 37.20 mm (SD± 3.79 mm), and Group III was 35.93 mm (SD± 2.90 mm). The differences found to be significant (p=0.044). Howevr, the mean value of the C3-H Group I and C3-RGN Group I, were not found to be significant respectivley (p=0.141 & 0.375) [Table/Fig-11,12 and 13].
Mean SD± of hyoid bone position measurement with in each group.
| Descriptive |
|---|
| Type | Norm | N | Mean | S.D. | Min. | Max. |
|---|
| H-H | Average | 30 | 4.65 | 3.18 | 1.00 | 11.00 |
| Horizontal | 30 | 6.63 | 4.32 | 1.00 | 19.00 |
| Vertical | 30 | 3.92 | 2.59 | 1.00 | 12.00 |
| H-RGN | Average | 30 | 34.87 | 3.88 | 24.00 | 42.00 |
| Horizontal | 30 | 37.20 | 3.79 | 31.00 | 44.00 |
| Vertical | 30 | 35.93 | 2.90 | 33.00 | 40.00 |
| C3-H | Average | 30 | 33.30 | 4.05 | 26.00 | 41.00 |
| Horizontal | 30 | 32.93 | 3.15 | 28.00 | 38.00 |
| Vertical | 30 | 31.45 | 4.11 | 25.00 | 43.50 |
| C3-RGN | Average | 30 | 69.27 | 6.07 | 57.00 | 81.00 |
| Horizontal | 30 | 68.43 | 6.38 | 57.00 | 83.00 |
| 30 | 67.23 | 4.13 | 59.00 | 75.00 |
One-way ANOVA of Hyoid bone position measurement.
| Type | Norm | N | Mean | S.D. | F-value | p-value | NS/S |
|---|
| H-H | Average | 30 | 4.65 | 3.18 | 5.00 | 0.009 | HS |
| Horizontal | 30 | 6.63 | 4.32 |
| Vertical | 30 | 3.92 | 2.59 |
| H-RGN | Average | 30 | 34.87 | 3.88 | 3.24 | 0.044 | S |
| Horizontal | 30 | 37.20 | 3.79 |
| Vertical | 30 | 35.93 | 2.90 |
| C3-H | Average | 30 | 33.30 | 4.05 | 2.00 | 0.141 | NS |
| Horizontal | 30 | 32.93 | 3.15 |
| Vertical | 30 | 31.45 | 4.11 |
| C3-RGN | Average | 30 | 69.27 | 6.07 | 0.99 | 0.375 | NS |
| Horizontal | 30 | 68.43 | 6.38 |
| 30 | 67.23 | 4.13 |
p<0.001 is very highly significant (vhs), p<0.01 is highly significant (hs), p<0.05 is significant (s), p>0.05 is not significant.
Discussion
Since the turn of the century, nasal airway function has been implicated as a contributory factor in dentofacial development; however there is another school of thought that denies any significant relationship between facial morphology and mode of breathing [10].
Gwynne-Evans and Ballard subjectively evaluated the relationship between facial morphology and breathing condition over period of 15 years and reported that orofacial morphology remains constant during growth regardless of breathing patterns [10,11]. Authors further concluded that there is no association between dentofacial deformity and malocclusion with mouth breathing. McNamara observed significant relationship between the pharyngeal structure and both dentofacial and craniofacial structure [12]. He reported that retropositioned maxilla and mandible and hyper divergant growth pattern with maxillary excess can cause narrowing of anteroposterior dimension of the airway [13]. Similarly the orophayngeal airway has its impact on the growth of craniofacial structures. During function of breathing and swallowing, the mandible and tongue are displaced downward and backward and head is tipped back in order to open mouth. All these postural changes suggest the possible morphological and physiological variation which can be induced by relationship of teeth and direction of jaw growth.
Present study also showed the significant differences between upper oropharyngeal widths in different facial skeletal pattern. Subjects with vertical skeletal pattern have significantly narrower upper airways than those with horizontal skeletal pattern. Similar finding had been reported by Marcos Roberto de Freitas et al., which had been corroborated by present study [14].
The anterior wall of the oropharynx consists of very movable structures such as the tongue and the hyoid bone, and the posterior border is formed by the cervical vertebrae, which are also capable of changing their positions. As the mandible is moved posteriorly in relation to the other craniofacial structures, the tongue and hyoid do not follow this movement in a similar manner. If it happens, it might encroach upon the vital airway. To avoid this problem, the hyoid-associated structures are guided to an inferior position suggesting the stability and patency of the pharyngeal airway as primary factors in hyoid positioning [15].
The documentations of effect of change in antero-posterior position of the mandible on hyoid bone position and the pharyngeal airway space are seen among the literature. Battagel et al., reported a more posterior position of the hyoid bone in class II subject with constricted upper pharyngeal width [16]. Adamidis and Spyropoulos also showed that hyoid bone in class III subject lies in more forward position [17].
According to present study H-RGN (line from hyoidale to retrognathion) values were significantly higher in short face subjects when compared with vertical and average face subjects. The hyoid bone was positioned farther from the mandibular symphysis in brachyfacial subjects, reflected by the larger H-RGN values compared with the dolichofacial and normal subjects. This finding is in agreement with Eung-Kwon et al., according to which brachyfacial person has a hyoid bone position closer to the mandibular plane and more posteriorly located— i.e. toward the cervical vertebrae [18]. On contrary, position of hyoid bone in dolichofacial and normal subjects have is more inferiorly and anteriorly positioned. Paes et al., also observed hyoid bone position farther from mandibular symphysis in hypodivergent growth pattern group [19].
In the present study Increase in H-H1(hyoidale-hyoidale perpendicular) value i.e. the vertical position of hyoid bone were also seen in horizontal group when compared to average and vertical groups.
The functions of the tongue and lower jaw muscles alter craniofacial growth and development. Same have been reported by Ferraz et al., in their study that strain of the muscle, ligaments and fascia affects the position of hyoid bone in Angle’s class I, II and III malocclusion [20].
Wright et al., studied that the tongue posture in normal subjects was such that the apex of the tongue was slightly below the incisal edges of the mandibular incisors and the dorsum was visible above the teeth in all parts of the mouth [21]. Rakosi et al., also reported that in class II malocclusion patients, dorsum of tongue generally rest in high position. It has also been documented that In low level, the lateral borders of the tongue were found to rest against the lingual surfaces of the lower posteriors, while in the high level, the lateral borders were found to lie above the occlusal surfaces of the lower posteriors [22].
According to present study, the position of the dorsum of the tongue was found to be significantly higher in hyperdivergant cases at all level (Point 2 to 6). This finding is in agreement with a study by Elham Saleh et al., according to which in individuals with vertical skeletal pattern, the antero-posterior dimensions of the airway gets narrowed and to breathe through mouth, one must maintain an oral airway, and to accomplish this, the mandible and the tongue are displaced downward and backward and the head is tipped back [13].
Limitation
Since present study has been performed retrospectively on lateral cephalogram which is 2D image of 3D structures, future studies can be planned on recent CBCT and MRI modalities to make study more relevant in long term. Further study can be performed on larger scale in longitudinal pattern to provide more clinical data. In this study, the hyoid bone position was assessed using the hyoid triangle analysis. However, some individual variations may have to be accepted in the hyoid bone measurements. Findings of the study can be used as clinical guidance to assess airways abnormalities in long term and predict prognosis and treatment modalities.
Conclusion
The upper oropharyngeal width is seen to be narrower in subjects with vertical growth pattern.
The position of dorsum of the tongue is seen to be placed higher in subjects with vertical growth pattern at all level.
The hyoid bone was more inferiorly and posteriorly positioned in subjects with horizontal growth pattern.
Variations are seen in upper and lower oropharyngeal widths, posture of the tongue and hyoid bone position in all the growth patterns.
p<0.001 is very highly significant (vhs), p<0.01 is highly significant (hs), p<0.05 is significant (s), p>0.05 is not significant.
p<0.001 is very highly significant (vhs), p<0.01 is highly significant (hs), p<0.05 is significant(s), p>0.05 is not significant.
p<0.001 is very highly significant (vhs), p<0.01 is highly significant (hs), p<0.05 is significant (s), p>0.05 is not significant.
[1]. Ceylan I, Oktay H, A Study on the pharyngeal size in different skeletal patternsAm J Orthod Dentofacial Orthop 1995 108:69-75. [Google Scholar]
[2]. Pae EK, Blasius JJ, Nanda R, Heterogeneity in vertical positioning of the hyoid bone in relation to genioglossal activity in menAngle Orthod 2004 74:343-48. [Google Scholar]
[3]. Urzal V, Braga AC, Ferreira AP, Hyoid bone position and vertical skeletal pattern- open bite/deep biteOral Health Dent Manag 2014 13:341-47. [Google Scholar]
[4]. Jena AK, Duggal R, Hyoid bone position in subjects with different vertical jaw dysplasiasAngle Orthod 2011 81:81-85. [Google Scholar]
[5]. Opdebeeck H, Bell WH, Eisenfeld J, Mishelevich D, Comparative study between the SFS and LFS rotation as a possible morphogenic mechanismAm J Orthod 1978 74:509-21. [Google Scholar]
[6]. Kuramae M, Magnani MB, Boeck EM, Lucato AS, Jarabak’s cephalometric analysis of brazilian black patientsBraz Dent J 2007 18:258-62. [Google Scholar]
[7]. McNamara JA, A method of cephalometric evaluationAm J Orthod 1984 86:449-69. [Google Scholar]
[8]. Rakosi T, An atlas & manual of cephalometric radiography 1982 Wolfe medical publications ltd:96-99. [Google Scholar]
[9]. Bibby RE, Preston CB, The hyoid triangleAm J Orthod 1981 80:92-97. [Google Scholar]
[10]. Gwynne-Evans E, Discussion on the mouth –breatherProc R Soc Med 1958 51:279-82. [Google Scholar]
[11]. Yamaoka M, Furusawa K, Uematsu T, Okafuji N, Kayamoto D, Kurihara S, Relationship of the hyoid bone and posterior surface of the tongue in prognathism and micrognathiaJ Oral Rehabil 2003 30:914-20. [Google Scholar]
[12]. McNamara JA, Influence of respiratory pattern on craniofacial growthAngle Orthod 1981 51:269-300. [Google Scholar]
[13]. Abu Allhaija ES, Al-Khateeb SN, Uvulo-Glosso-Pharyngeal dimensions in different antero-posterior skeletal patternsAngle Orthod 2005 75:1012-18. [Google Scholar]
[14]. Freitas MR, Alcazar NM, Janson G, Freitas KM, Henriques JF, Upper and lower pharyngeal airways in subject with ClassI and Class II malocclusions and different growth patternsAm J Orthod Dentofacial Orthop 2006 130:742-45. [Google Scholar]
[15]. Tourne LP, Growth of the pharynx and its physiologic implicationsAngle Orthod 1990 60:184-93. [Google Scholar]
[16]. Battagel JM, Johal A, L’Estrange PR, Croft CB, Kotecha B, Changes in airway and hyoid position in response to mandibular protrusion in subjects with obstructive sleep apnoeaEur J Orthod 1999 21:363-76. [Google Scholar]
[17]. Adamidis IP, Spyropoulos MN, Hyoid bone position and orientation in Class I and Class III malocclusionsAm J Orthod Dentofacial Orthop 1992 101:308-12. [Google Scholar]
[18]. Jena AK, Duggal R, Hyoid bone position in subjects with different vertical jaw dysplasiasAngle Orthod 2011 81:81-85. [Google Scholar]
[19]. Pae EK, Quas C, Quas J, Garrett N, Can facial type be used to predict changes in hyoid bone position with age? A perspective based on longitudinal dataAm J Orthod Dentofacial Orthop 2008 134:792-97. [Google Scholar]
[20]. Ferraz MJ, Nouer DF, Fausto Bérzin, Sousa MA, Romano F, Cephalometric appraisal of the hyoid triangle in brazilian people of piracicaba’s regionBraz J Oral Sci 2006 5:1001-06. [Google Scholar]
[21]. Hotokezaka H, Matsuo T, Nakagawa M, Mizuno A, Kobayashi K, Severe dental open bite malocclusion with tongue reduction after orthodontic treatmentAngle Orthod 2001 71:228-36. [Google Scholar]
[22]. McKee TL, A cephalometric radiographic study of tongue position in individuals with cleft palate deformityThe angle orthodontist 1956 4:99-109. [Google Scholar]