For any precise radiographic diagnosis of a pathological lesion the knowledge of normal anatomic landmarks is very important, as failure to delineate the normal from the abnormal could prove to be catastrophic [1].
One such normal anatomic variant that is to be kept in mind is the Zygomatic Air Cell Defect (ZACD), which was a term coined by Tyndall and Matteson in the year 1987 and defined it as accessory cells in the zygomatic process and articular eminence of the temporal bone, which appears similar to mastoid air cells and which do not extend further anteriorly than the zygomatico-temporal suture [2].
ZACD occurs in the zygomatic arch which presents as an asymptomatic, radiolucent, non-destructive, non-expansile defect, detected incidentally on a panoramic radiograph [3].
The recognition of these air cells is important from surgical point of view as when they are demonstrated preoperatively on a panoramic radiograph, these may become contraindications to performing surgical procedures such as eminoplasty or eminectomy for the treatment of mandibular dislocation as they may become potential pathways for intracranial infections [4].
The present retrospective study was undertaken by evaluating 6825 panoramic radiographs of patients from Indian origin, to estimate the prevalence, radiographic appearance, characteristics and to propose a classification for ZACD among Indian population using digital panoramic radiography. Although similar kind of studies have been carried out in the past but none have been carried out in India with such a large sample size and also neither of the previous researches have classified the defect on the basis of appearance, location and occurrence.
Materials and Methods
The present study was carried out in Department of Oral Medicine and Radiology and a total of 6825 routine digital panoramic radiographs were included, of patients aged between 4-90 years during the period of December 2011 to June 2014. The cases in which there was pervious history of maxillofacial fractures or had anomalies or radiographs in which the zygomatic arch was not adequately visible for technical or anatomic reasons were excluded from the study.
Digital radiographs were obtained using Sirona Orthophos XG 5 and evaluated using SIDEXIS XG v2.52 (software provided by the manufacturer). The evaluation of the radiographs was done by four oral radiologist simultaneously and the ZACD was recorded only when the decision was indisputable. The same procedure for evaluation was performed after an interval of one month to verify the previous results obtained to avoid bias and the radiographs which had the same result as in the previous evaluation were considered.
Afterwards, ZACD was categorised according to: 1) Location: Unilateral or Bilateral; 2) Appearance: Unilocular or Multilocular; 3) Demographic data: Age and Sex. All the recording was done using Microsoft Office Excel.
Results
Out of total 6825 subjects the age range was 4 to 90 years with an overall mean age of 36.24±12.26 years. Out of total number of subjects 3617 were males and 3208 were females with an overall mean age of 34.62±13.19 years and 31.04±10.98 years respectively.
Out of 6825 digital panoramic radiographs evaluated, ZACD was noted among 133 subjects, youngest subject being four years of age and eldest being 85 years of age, with an overall percentage of 1.94%.
Amongst the 133 ZACDs [Table/Fig-1], 84 were noted in males and 49 were noted in females. Amongst the ZACDs 112 occurred unilaterally and 21 occurred bilaterally. Out of 112 ZACD which occurred unilaterally 58 were seen on the left side and 54 on the right side. A total of 30 ZACD presented to be unilocular and 103 presented to be multilocular in appearance [Table/Fig-2].
Age wise distribution of subjects.
| Groups | Age Range (Years) | Subjects in each group | ZACD | Occurrence% | Males | Females |
|---|
| Group I | 4 – 14 | 1027 | 2 | 1.5 | 1 | 1 |
| Group II | 15 – 30 | 1960 | 58 | 43.60 | 32 | 21 |
| Group III | 31 – 45 | 1187 | 37 | 27.81 | 15 | 10 |
| Group IV | 46 – 60 | 1134 | 19 | 14.28 | 10 | 7 |
| Group V | 61 – 75 | 1049 | 11 | 8.27 | 13 | 6 |
| Group VI | > 76 | 468 | 6 | 4.51 | 13 | 4 |
| Total | 6825 | 133 | 100 | 84 | 49 |
Comparison of ZACD with Age, Location and Appearance.
| Age Groups | Appearance | Location |
|---|
| Unilocular | Multilocular | Unilateral | Bilateral |
|---|
| Left | Right | Total | Bilateral |
|---|
| Group I | 2 | 0 | 0 | 2 | 2 | 0 |
| Group II | 9 | 49 | 24 | 22 | 46 | 12 |
| Group III | 11 | 26 | 17 | 15 | 32 | 5 |
| Group IV | 4 | 15 | 9 | 7 | 16 | 3 |
| Group V | 2 | 9 | 6 | 4 | 10 | 1 |
| Group VI | 2 | 4 | 2 | 4 | 6 | 0 |
| Total | 30 | 103 | 58 | 54 | 112 | 21 |
Amongst the 112 ZACD found to be unilateral, 74 were found in males and 38 were found in females and out of 21 ZACD that had a bilateral presentation 13 were noted in males and eight were noted in females. Further, out of 74 males with unilateral presentation of ZACD 41 were noted on the left side and 33 were noted on the right side and among the 38 females, 21 were observed on the left side and 17 on the right side.
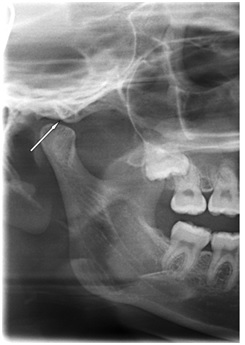
Amongst the 30 ZACDs that appeared to be unilocular [Table/Fig-3], 19 were observed in males and 11 were observed in females. Out of 103 ZACDs with multilocular [Table/Fig-4] presentation 56 were noted in males and 47 in females.
Orthopantomogram showing unilocular appearance of ZACD.
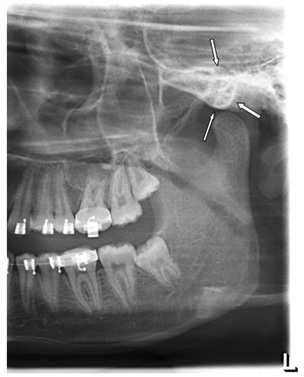
Orthopantomogram showing multilocular appearance of ZACD.
On further evaluation of the radiographs we observed that out of total 21 bilateral presentations of ZACD 10 cases had a unilocular appearance bilaterally, nine cases had a unilocular presentation on one side and a multilocular presentation on the other and two cases had a multilocular appearance bilaterally.
Discussion
Pneumatization refers to the development of air-filled cavities in the bones. The structures that develop by gradual Pneumatization of solid tissue and are the best characterized structures for aeration in humans are the mastoid air cells and Paranasal Sinuses (PNSs) [5]. The primary region of Pneumatization in the temporal bone consists of the middle ear, squamomastoid, perilabyrinthine, petrous apex. Accessory region includes the squamous, the zygomatico occipital and the styloid. ZACD is produced by the extension of periantral air cells in to the zygomatic arch [6].
The occurrence of ZACDs has been considered similar to that of pneumatisation of mastoid process. Air cells can be a potential pathway for the spread of infections, pathological processes and cranial sepsis, thus it is mandatory to have a thorough knowledge of the air cells [7]. There can be complications such as dural tear and cerebro-spinal fluid leakage during surgical procedures involving mandibular condyle and articular eminence which results from penetration through the defect. Procedures such as eminoplasty and eminectomy are also contraindicated [8].
A few central pathologies have been recognized to involve the zygomatic processes which contribute its differential diagnosis, namely aneurismal bone cyst, central or osseous haemangioma, central giant cell tumour, eosinophilic granuloma, fibrous dysplasia and metastatic tumours. Unlike ZACD these lesions present with symptoms like pain, swelling over the zygoma, facial asymmetry along with radiographic evidence of cortical expansion [1]. A classification was proposed by Tyndall and Matterson, which classified ZACD into three types: unilocular, multilocular and trabecular type. Unilocular refers to a well defined oval radiolucency, multilocular refers to numerous small cavities similar to mastoid air cells and trabacular variant has been defined as a multilocular defect, but with internal bony striations [2].
In the present study the overall prevalence was 1.94% which is in accordance with the research work of Patil et al., and Hofman et al., [1,8]. Previously conducted study by Zamaninaser et al., on 2600 orthopantomograms of Esfehanian population shows an overall prevalence 3.6% [9]. In two different research works undertaken on South Indian population by Srikanth et al., and Balla et al., showed an overall prevalence of 2.5% and 2.8% respectively [10,11]. In a study carried out in North Indian population by Gupta et al., gave an overall prevalence of 5.7% [3]. The difference in sample size and the region over which the research work was undertaken can be major factor for explain the difference in overall prevalence.
In the present study it was observed that prevalence of ZACD was almost double in males as compared to females i.e. M:F = 1.7:1. These findings are in complete agreement with the studies carried out by Park et al., and Patil et al., in which M:F was 2.4:1 and 1.82:1 respectively [1,6]. According to studies carried out by Carter et al., and Srikant et al.,, gender do not play a key role in the prevalence of ZACD and there is no gender predilection [4,10]. Some researchers like Orhan et al.,, Miloglu et al.,, Zamaninaser et al., and Balla et al., have concluded that there is a female predilection for the prevalence of ZACD and gave a M:F of 1:1.7, 1:1.5, 1:1.6 and 1:2.5 respectively [7,9,11,12]. The number of female participants was more as compared to males in the mentioned research works, which could be the reason for the reversed gender ratio. This is the only topic of debate for all the researchers over which no conclusion can be made [Table/Fig-5].
Clinical studies comparing the features of ZACD included in the study.
| Study | No. of Participants | Population | Prevalence | Sex Ratio (M:F) | Laterality | Locularity |
|---|
| Patil et al., [1] | 7755 | Indian | 1.82 | 1.82:1 | 2/3rd Unilateral1/3rd Bilateral | 2/3rd Multilocular1/3rd Unilocular |
| Srikanth et al., [10] | 600 | South Indian | 2.5 | 1:1 |
| Orhan et al., [7] | 1006 | Turkey | 1.88 | 1:1.7 |
| Miloglu et al., [12] | 514 | Turkey | 8 | 1:1.5 |
| Yavuz et al., [13] | 8107 | Turkey | 1.03 | 1:1 |
| Park et al., [6] | 1400 | South Korea | 2.2 | 2.4:1 |
| Zamaninaser et al., [9] | 2600 | Esfehanian | 3.6 % | 1:1.6 | Equal presentation on both sides |
| Gupta et al., [3] | 800 | North Indian | 5.7 | 1.7:1 | 2/3rd Unilateral1/3rd Bilateral | 95.6% Unilocular4.4% Multilocular |
| Carter et al., [4] | 2734 | Buffalo, USA | 1.5 | 1:1 | |
| Balla et al., [11] | 500 | South Indian | 2.8 | 1:2.5 | Equal Occurrence |
According to the present study the prevalence of ZACD is least during the early and elderly ages. It is most prevalent during the second, third and fourth decade of life and as the age increases its prevalence decreases. Although the defect was also noticed before and after the second and fourth decade, the youngest individual being 12 years of age and the oldest being 85 years. The same has been attributed by Park et al., in which they have suggested that the chance of occurrence decreases above the age of 60 years [6].
In the present study nearly 2/3rd of the cases had a unilateral presentation and nearly 1/3rd of the cases had a bilateral presentation which is in agreement with the research carried out by Patil et al., Gupta et al., and Srikanth et al., [1,3,10]. In a study conducted by Yavuz et al., shows a conflicting side to this finding where bilateral presentation is more as compared to unilateral [13]. In case of unilateral presentation, the frequency of occurrence was nearly equal for the left and the right side which goes along the previous study by Zamaninaser et al., where equal presentations was noted on both sides [9]. But this contradicts the research that were carried out by Patil et al., and Srikanth et al., in which the right side was more frequently involved than the left side [1,10] [Table/Fig-6].
Classification of ZACD according to location and appearance.
| TYPE | NATURE |
|---|
| TYPE I | Unilateral presentation (left or right side) with unilocularity |
| TYPE II | Unilateral presentation (left or right side) with multilocularity |
| TYPE III | Bilateral presentation with unilocular defect on both sides |
| TYPE IV | Bilateral presentation with multilocular defect on both sides |
| TYPE V | Bilateral presentation with unilocular defect on one side and multilocular on the other |
On further analysis, multilocular defects were nearly 2/3rd and unilocular defects are nearly 1/3rd which is in conformity with the researches carried out by Patil et al., Orhan et al., Zamaninaser et al., and Yavuz et al., but contradicts the statement given by Gupta et al., and Park et al., which states that unilocular presentation is more common than multilocular [1,3,6,7,9,13]. On the other hand Tyndall and Matterson gave an equal number of both variants in their research [2] [Table/Fig-5].
On analysis of the date from the current research, a classification for ZACD was proposed which is based on appearance, location and occurrence as mentioned in [Table/Fig-6]. Earlier authors had classified this condition only according to its appearance. In the present study it was observed that location i.e. left or right side and occurrence i.e. unilateral or bilateral, are also a key factors in classifying ZACD. While reporting a radiograph it would become easy for a radiologist to just mention the type of lesion, as that would denote the nature, location and occurrence at the same time. Further it would be easy for the operating Surgeon to understand and plan a surgical treatment. The present classification only considers two variants of ZACD i.e. unilocular and multilocular, the trabecular pattern has not been included as it has been previously mentioned that trabecular pattern is a multilocular defect but with internal bony striations.
Limitation
Further studies are advised to be carried out using the latest imaging modalities such as CBCT and also comparative studies need to be undertaken between normal and diseased bone to give a clear picture of the bony changes.
Conclusion
In conclusion, the present study gives a clear picture of prevalence of ZACD among Indian population and also establishes a relationship when compared to that of other countries. The prevalence among Indian population was recorded to be 1.94%, with a male predilection, seen mostly in the second, third and fourth decade with unilateral–unilocular type of presentation being most common type. Also, a new method to classify this defect has also been proposed with a significance of, ease of reporting and identifying this condition which would be helpful for the professionals to understand.