Granulomatous prostatitis is an unusual form of inflammatory condition of the prostate which rarely presents in the urological practice. Granulomatous prostatitis was first described by Tanner and McDonald in 1943 with an incidence of 3.3% of total inflammatory lesions of prostate [1]. Clinically, it presents with hard fixed nodule on digital rectal examination (DRE), elevated serum Prostatic specific antigen (PSA) levels and with hypoechoic shadows on transrectal ultrasound (TRUS) thus mimicking prostatic carcinoma. Hence, histopathology remains the gold standard method for diagnosis of granulomatous prostatitis.
Giving the importance of granulomatous prostatitis in uropathology, the present study was undertaken to diagnose and classify the granulomatous prostatitis on histopathological examination and emphasizing, the distinction between non-specific and infectious granulomatous prostatitis for therapeutic purpose and also to know the prevalence of granulomatous prostatitis at our tertiary care centre.
Materials and Methods
Histopathological records of 1,203 prostatic specimens (TURP chips, needle biopsies) received in the Department of Pathology, ACPM Medical College, Dhule, over a period of five years (2009-2014) were reviewed.
Following inclusion and exclusion criteria were adopted in our study–
Inclusion criteria: All types of prostatic specimens including TURP and needle biopsies were considered in this study.
Exclusion criteria: Inadequate biopsies and poorly preserved prostatic specimens were excluded.
The cases with histopathological diagnosis of granulomatous prostatitis were retrieved and retrospective data was collected from the patient’s record. The data included patient’s clinical information like age, presenting complaints, digital rectal examination (DRE) findings and laboratory investigation like PSA levels and TRUS were recorded.
Sections from each case, of histopathologically diagnosed granulomatous prostatitis on Haematoxylin and Eosin (H&E) were stained with special stains like Gomori’s stain, Periodic acid Schiff (PAS) and Ziehl Neelsen stain (ZN stain) which is helpful in confirming the infectious granulomatous prostatitis. The H&E and special stains were done as per the procedure described by John D Bancroft [2].
Results
A total of 10,587 histopathological specimens were received to the Department of Pathology out of which 1,203 were prostatic specimens accounting for 11.36% of total specimens received. Prostatic specimens included were TURP and needle biopsies for histopathological examination. Among 1,203 prostatic specimens, 17 cases of granulomatous prostatitis were retrieved on histopathology accounting for an incidence of 1.4%. The clinical features, laboratory investigations and histopatological diagnosis of the patients are described in detail [Table/Fig-1]. The common age group encountered in our study ranged between 51-75 years. The most common presenting symptom was increased frequency with/without obstruction. DRE showed firm and nodular mass in 6 cases while 10 cases showed hard fixed nodule. The PSA levels ranged from 2.8ng/ml to 28.8ng/ml with mean PSA levels of 15.8ng/ml. TRUS showed hypoechoic shadows in 6 cases and rest in 11cases, TRUS was within normal limits. None of these cases were suspected as granulomatous prostatitis on clinical basis.
Clinical summary of patients with 17 granulomatous prostatitis.
| Case No. | Age | Clinical features | PSA levels | DRE | TRUS | Clinical diagnosis | Specimen type | Histopathological diagnosis |
|---|
| 1 | 67 | Irritative voiding | 6 | Firm, nodular | NL | BPH | TURP | Xanthogranulomatous prostatitis |
| 2 | 58 | Obstructive voiding | 7.6 | Hard and fixed nodule | NL | BPH | TURP | NSGP |
| 3 | 63 | Irritative and obstructive voiding | 5.5 | Firm, nodular | NL | BPH | TURP | Xanthogranulomatous prostatitis |
| 4 | 81 | Irritative and obstructive voiding | 4.8 | Firm, nodular | NL | BPH | TURP | Xanthogranulomatous prostatitis |
| 5 | 56 | Irritative voiding | 6.2 | Hard and fixed nodule | NL | BPH | TURP | NSGP |
| 6 | 58 | Irritative voiding | 2.8 | Firm, nodular | NL | BPH | TURP | NSGP |
| 7 | 70 | Irritative and obstructive voiding | 6.2 | Hard and fixed nodule | NL | BPH | TURP | NSGP |
| 8 | 67 | Irritative and obstructive voiding with haematuria | 13.6 | Hard and fixed nodule | NL | Carcinoma | NB | NSGP |
| 9 | 51 | Obstructive voiding with fever and haematuria | 25.7 | Hard and fixed nodule | Focal hypoechoic | Carcinoma | NB | NSGP |
| 10 | 65 | Obstructive voiding | 22.3 | Hard and fixed nodule | Focal hypoechoic | Carcinoma | NB | NSGP |
| 11 | 65 | Irritative and obstructive voiding | 5.2 | Hard and fixed nodule | NL | BPH | TURP | xanthogranulomatous prostatitis |
| 12 | 75 | Obstructive voiding | 6.2 | Firm, nodular | NL | BPH | TURP | xanthogranulomatous prostatitis |
| 13 | 55 | Irritative and obstructive voiding with haematuria | 17.7 | Firm, nodular | Focal hypoechoic | Carcinoma | NB | Tubercular prostatitis |
| 14 | 64 | Obstructive voiding with fever | 20.2 | Hard and fixed nodule | Focal hypoechoic | Carcinoma | NB | Tubercular prostatitis |
| 15 | 72 | Irritative and obstructive voiding with fever | 16.8 | Hard and fixed nodule | NL | BPH | TURP | Tubercular prostatitis |
| 16 | 65 | Obstructive voiding | 28.8 | Hard and fixed nodule | Focal hypoechoic | Carcinoma | NB | NSGP |
| 17 | 65 | Irritative and obstructive voiding with fever | 25.1 | Hard and fixed nodule | Focal hypoechoic | Carcinoma | NB | NSGP |
*TURP: Transurethral resection of the prostate NB: Needle biopsy. BPH: Benign prostatic hyperplasia. NSGP: Nonspecific granulomatous prostatitis. NL: Normal limits
Histopathological findings
Out of 17 cases of granulomatous prostatitis, granulomas were focal in 14 cases and diffuse in 3 cases. Distribution of granulomatous prostatitis is given in detail [Table/Fig-2].
Distribution of granulomatous prostatitis.
| Sl. No. | Type of granulomatous | No. of cases | % of cases |
|---|
| 1 | Non-specific granulomatous prostatitis | 9 | 53% |
| 2 | Xanthogranulomatous Prostatitis | 5 | 29.4% |
| 3 | Tubercular prostatitis | 3 | 17.6% |
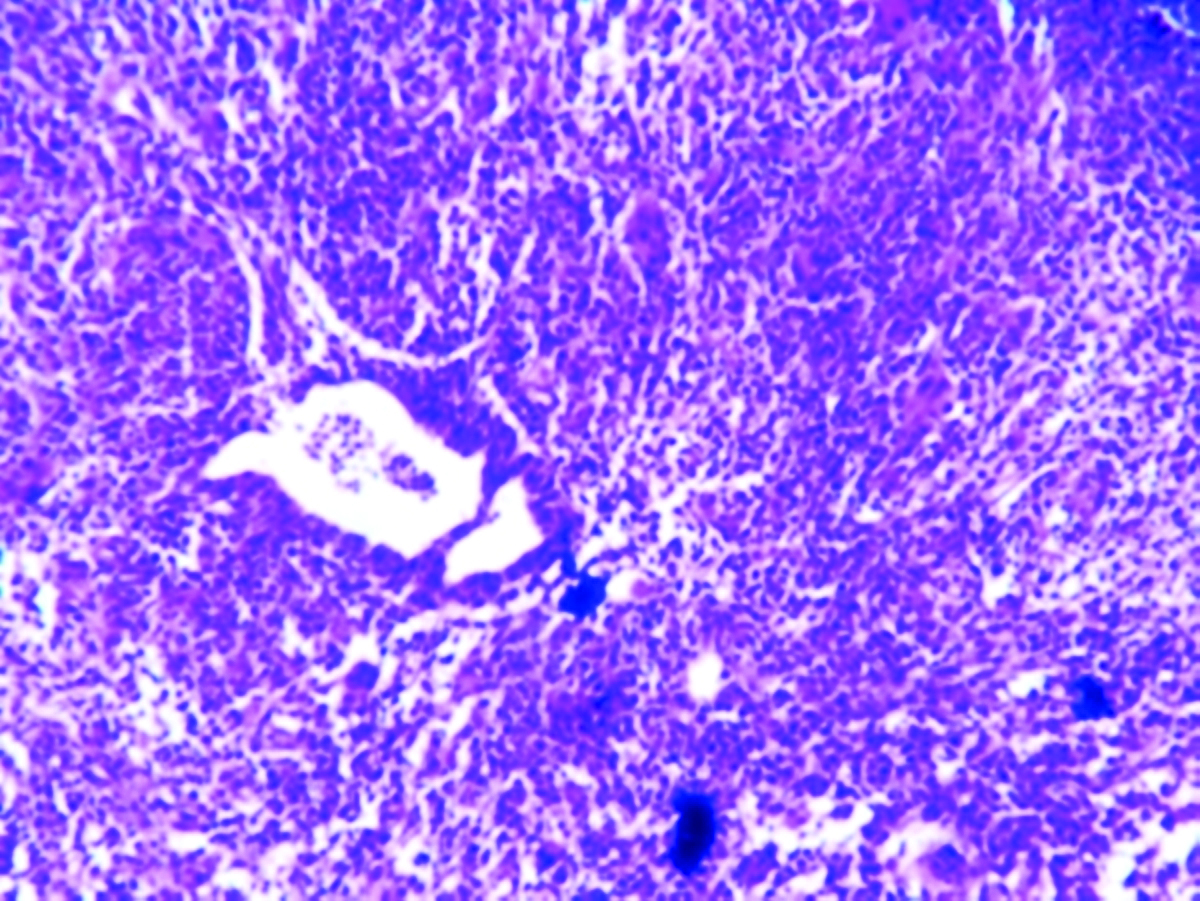
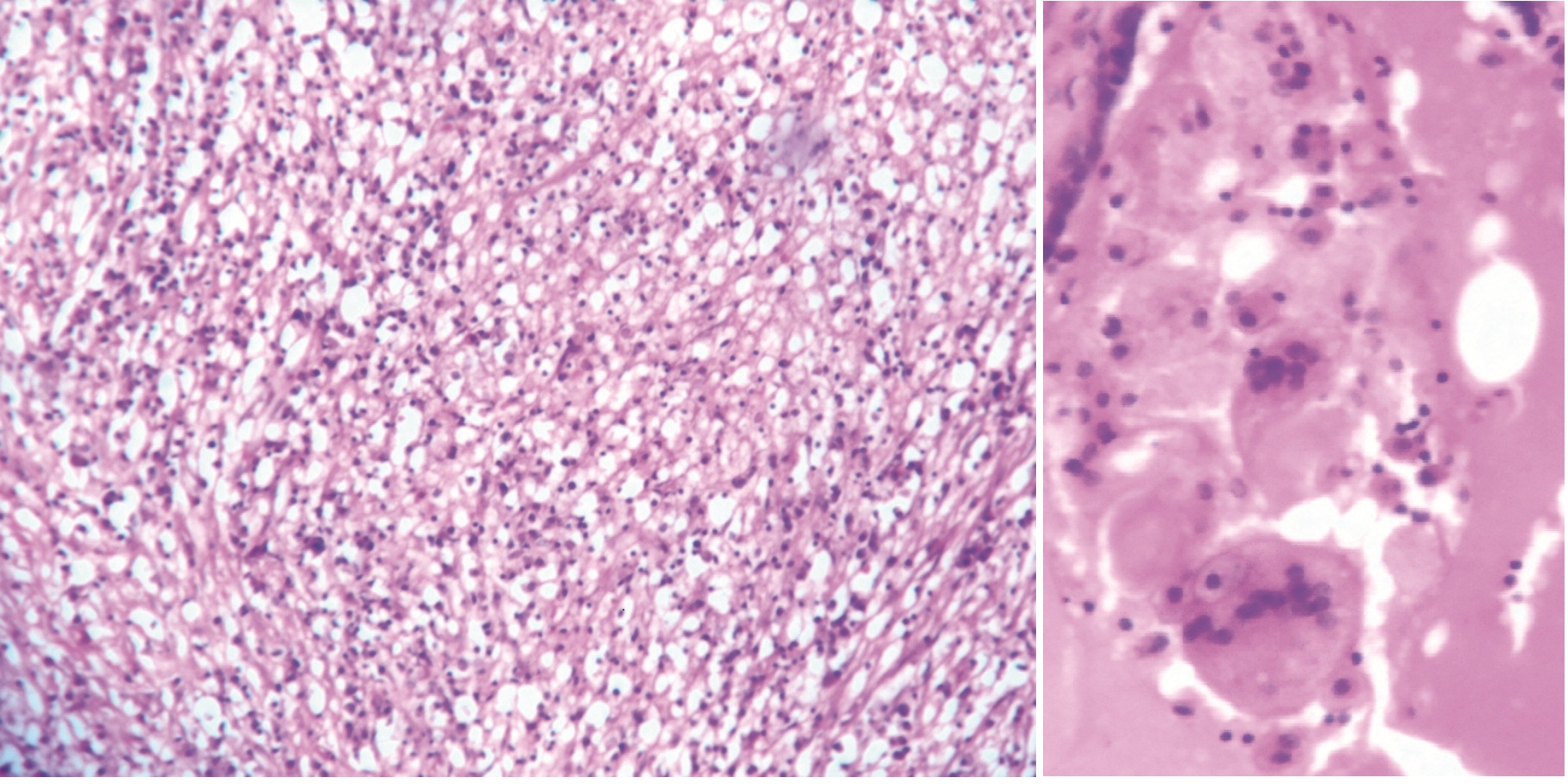
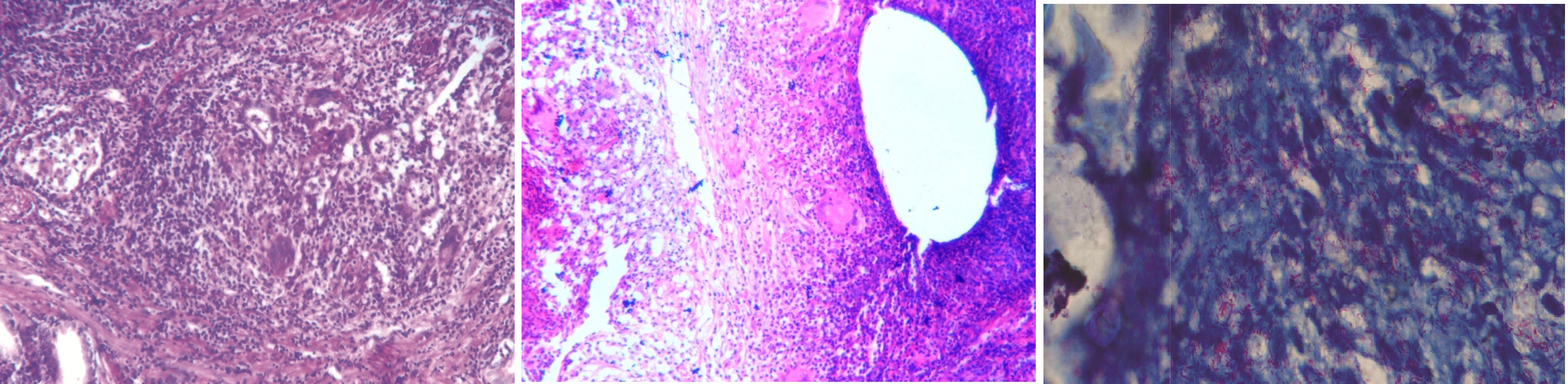
In 9 cases of non-specific granulomatous prostatitis, there are periglandular granulomas consisting of epithelioid cells, histiocytes, lymphocytes and foreign body type of giant cells as shown in [Table/Fig-3]. In 5 cases of xanthogranulomatous prostatitis showed granulomas consisting of focal diffuse infiltration of foamy macrophages, histiocytes, lymphocytes and foreign body type of giant cells [Table/Fig-4a&b]. In 3 cases of tubercular prostatitis, revealed multiple well formed granulomas consisting of epithelioid cells, histiocytes, lymphocytes and Langhans type of giant cells with focal areas of caseous necrosis as shown in [Table/Fig-5a-c]. Details of histomorphological features of granuloma are given [Table/Fig-6].
Non-specific granulomatous prostatitis (NSGP) showing granulomas causing destruction of the acini. (H&E, X100).
(a) Xanthogranulomatous prostatitis showing diffuse sheet of foamy macrophages. (H&E, X100). (b) Xanthogranulomatous prostatitis showing touton body gaint cell with foamy cytoplasm. (H&E, X400).
(a) Granulomatous prostatitis showing well formed epithelioid granulomas with Langhan’s type of giant cell. (H&E, X100). (b) Granulomatous prostatitis showing well formed epithelioid granulomas with Langhan’s type of giant cell. (H&E, X100). (c) Acid fast bacilli positivity (Ziehl Neelsen stain, X1000).
Histomorphological features of granulomatous prostatitis.
| Features | Number of cases |
|---|
| Distribution |
| Focal | 14 |
| Diffuse | 3 |
| Composition |
| Lymphocytes | 17 |
| Histiocytes | 17 |
| Plasma cells | 16 |
| Foamy cells | 7 |
| Epithelioid cells | 10 |
| Neutrophils | 14 |
| Giant cells(foreign body and langhans type) | 3 |
| Necrosis | 2 |
Discussion
Granulomatous prostatitis is an unusual entity. Epstein and Hutchin [1,3,4] classified briefly the granulomatous prostatitis based on aetiology and histopathology into following types, idiopathic (non specific), infective, iatrogenic (post surgery), malakoplakia, cases associated with systemic granulomatous diseases and allergy.
Classification of granulomatous prostatitis [5]:
1) Idiopathic (non-specific)
Typical nonspecific granulomatous prostatitis.
Xanthoma – xanthogranulomatous prostatitis.
2) Infectious
Bacterial: Tuberculosis, Brucellosis, Syphilis
Fungal: Coccididiomycosis, Cryptococcosis, Blastomy-cosis, Histoplasmosis, Paracoccidioidomycosis.
Parasitic: Schistosomiasis, Echinococcosis, Enterobiasis.
Viral: Herpes simplex virus.
3) Malakoplakia
4) Iatrogenic
Post surgical.
After radiation therapy.
BCG associated.
5) Systemic diseases: Sarcoidosis, Rheumatoid arthritis, Wegener’s granulomatosis, Polyarteritis nodosa, Churg- Strauss syndrome.
In granulomatous prostatitis exact aetiology is unclear but in most of the cases it is idiopathic and it has been thought to result from foreign body response to colloidal substances, bacterial products, refluxed urine or from an immunological response to extra ductal prostatic secretions arising from ducts obstructed by hyperplasia [1,6]. Literatures have mentioned various aetiology of granulomatous prostatitis like repeated urinary tract infections (73%), surgical interventions include TURP/open prostatectomy, needle biopsy and instillation of BCG into the bladder can result in granulomatous prostatitis [1,7,8]. Granulomatous prostatitis can occur in normal gland or nodular hyperplastic gland or in carcinomatous prostate [9]. In majority of the cases, the focus of granulomatous prostatitis is placed periglandular, with glandular destruction [10].
In granulomatous prostatitis grossly the gland is firm to stony hard. Cut section shows obliteration of architecture with formation of yellow granular nodules. Histopathological examination shows large nodular aggregates of histiocytes, epithelioid cells, multinucleated gaint cells and plasma cells are seen [11].
Stillwell et al., [12] reported 0.8% incidence of granulomatous prostatitis [1] and K Shanggar et al., showed an incidence of 0.65% of granulomatous prostatitis [9]. H Mohan et al., revealed 1.5% incidence of granulomatous prostatitis [1]. In the present study an incidence of 1.4% of granulomatous prostatitis was found and the results are in concordance with H Mohan et al., study [1].
Non-specific granulomatous prostatitis is the most common granulomatous lesion of the prostate accounting for 53% of the cases. Among the nine cases of non-specific granulomatous prostatitis five cases, clinically mimicked as carcinoma. Stillwell et al., [12] and Oppenheimer et al., [6] observed 69% and 77.7% of the cases respectively, of non-specific granulomatous prostatitis in their study and our finding is in consistent with Stillwell et al., [12].
In majority of the cases non-specific granulomatous prostatitis is an incidental finding with an incidence of 3.4% [13]. It is reported that an incidence of non-specific granulomatous prostatitis of 0.44% in routine prostectomy specimens, 0.29% in needle biopsies and 0.77% of TURP, simple prostatectomy and needle biopsy [7].
The age incidence ranges from 18-86 years with a mean of 62 years. Common symptoms include irritative and obstructive voiding symptoms, fever and chills.
The cause of this lesion may be due to a reaction to bacterial toxins, cell debris, and secretions spilling into the stroma from blocked ducts. The initial presentation of the lesion consists of dilated ducts and acini filled with neutrophils, foamy histiocytes, and desquamated epithelial cells. Rupture of these ducts and acini result in a localized granulomatous and chronic inflammatory reaction. Surrounding the ruptured acini are multinucleated giant cells, lymphocytes, plasma cells, epithelioid histiocytes and eosinophils. These dense nodules of inflammatory infiltrate obscure and efface ductal and acinar elements [13].
In the present study, the prevalence of non-specific granulomatous prostatitis account for 0.87% which is lower than reported by Sorenson FB et al., [9]. It is important to differentiate non-specific granulomatous prostatitis from other granulomatous prostatitis as it is self limiting while other specific granulomatous lesion needs treatment for causative aetiology. In our study, all the nine cases were self limiting and had uneventful follow-up period.
Xanthogranulomatous prostatitis was first described in 1943 by Tanner Mc Donald [1]. The exact aetiology and pathogenesis is unclear/ unknown. Possible aetiology suggested were due to release of altered prostatic secretions from obstructed ducts [14], recurrent urinary tract infection, repeated E-coli infections and other causes include autoimmune diseases [10] and hyperlipidaemia [1]. Xanthograulomatous prostatitis is well known in kidney, gallbladder but less known in prostate [14]. Clinically xanthograulomatous prostatitis mimics carcinoma on DRE and TRUS with raised PSA levels. Histopathologically xanthograulomatous prostatitis is confused with clear cell prostatic carcinoma. Microscopic examination reveals focal diffuse foamy macrophages with dark eccentric nuclei or localized collection of cholesterol laden histiocytes. It is a solitary microscopic lesion in the peripheral zone or transition zone [15]. Management of xanthograulomatous prostatitis is not very different from unlike xanthograulomatous of the kidney. Thus xanthograulomatous prostatitis is managed initially by conservative treatment and later by surgery if conservative treatment is ineffective. In the present study, we report 5 cases of xanthograulomatous prostatitis out of 1,023 prostatic specimens accounting 0.4% incidence of xanthograulomatous prostatitis. In our study all the cases of xanthograulomatous prostatitis were managed by conservative treatment with uneventful follow-up period till the date of review of the case.
Infectious Granulomatous prostatitis can be caused due to mycobacterium tuberculosis, treponema pallidum, viruses, fungi or due to intravesical Bacillus Calmette-Guerin (BCG) therapy for bladder cancer [1,16]. The prostate, epididymis and testis are the organs most commonly involved in tuberculosis of the male genital system [11]. Grossly the lesions are usually bilateral. Early lesions are seldom detected on palpation; it shows confluent caseous zones with liquefaction, cavitation and sinus tracts into rectum, perineum and peritoneal cavity. In late stages of tubercular prostatitis the gland is shrunken, fibrotic and hard simulating carcinoma on palpation. Microscopically, the initial lesion of the tubercular prostatitis occurs in the stroma and quickly spreads to acini. Well developed lesions show confluent foci of caseation with incomplete fibrous encapsulation [17]. Histochemical stain such as Periodic acid Schiff (PAS), Gomori’s stain and Ziehl Neelsen (ZN) stain are helful in confirming infectious granulomatous prostatitis. Tubercular prostatitis is common in people treated with intravesical bacillus Calmette- Guerin (BCG) therapy for bladder cancer. Histopathologically these type of granulomas may be caseating or noncaseating commonly located along the periurethral or transitional zone or involve the gland diffusely [17]. Tubercular prostatitis occurs in 1.3% of patient after intravesicle BCG treatment [18]. Prostatic involvement in systemic tuberculosis ranges from 3%-12%. In >90% of cases of tubercular prostatitis there is co-exsisting pulmonary tuberculosis. In patient with urogenital tuberculosis, 75-95% of cases show tuberculosis of prostate [9]. Most cases of tuberculosis of prostate arise from haematogenous dissemination rather than infected urine. In the present study the prevalence of 0.29% of tuberculosis of prostate was found. In our study all the three cases had associated with pulmonary tuberculosis. Out of three cases one case showed AFB positive with bacterial index 1+ on ZN stain.
All the three cases of tubercular prostatitis were started with anti-tuberculous therapy comprised of triple drug regimen of rifampicin, ethambutal and isonaizid for six months. Post treatment patient doing well till the date of review of the case. In most of the cases of granulomatous prostatitis surgical management is avoided as it leads to complications such as vesical neck contracture and requires repeat resection [1].
Literatures have shown that the screening of tubercular prostatitis can be done by detection of acid fast bacilli in the culture of serial urine, prostatic secretion and semen culture. Studies have revealed that the sensitivity of acid fast bacilli identification in prostatic secretion is higher (52%) than the serial urine and semen culture (50%) [19,20].
In recent days there is increase in the prevalence of iatrogenic granulomatous prostatitis due to various surgical interventions like TURP and needle biopsies. These surgical techniques causes reaction to the altered glandular epithelium and stroma caused due to trauma or surgery, resulting in formation of multiple granulomas in the prostate. In most of these cases it resolves spontaneously [21].
Studies have revealed the co-existence of carcinoma in 10-14% of patient with clinically diagnosed granulomatous prostatitis [9,13] but in our study, we did not find any record of such case. This is due to increased awareness of pathologist of usage special staining technique for confirmation.
Limitations
The present study has its own inherent limitations as it lacks the inter observer variation of the clinician and the histopathologist. Our study did not consider the correlation between the various surgical techniques performed and the histopathological diagnosis done and no comments were made on the usefulness of total and free PSA level assay in the histopathological diagnosis. Various scientific literatures reveal, that the histological absence of caseation necrosis and granulomas, does not rule out the diagnosis of tuberculosis. The present study fails to use the modern diagnostic methods of tuberculosis and to highlight the recent diagnostic modalities of tuberculosis with its limitations. The study being reterospective the above mentioned limitations were behind our control.
Conclusion
There is no specific pattern of clinical, biochemical and ultrasound findings which allows the diagnosis of granulomatous prostatitis and also its differentiation from prostatic carcinoma. Hence histopathology remains the gold standard test for diagnosis of granulomatous prostatitis, inspite of various diagnostic tests like TRUS, DRE and serum PSA levels. The histopathological pattern of granulomatous prostatitis is essential to mention in the reports as the mode of therapeutic management differs with the sub type of granulomatous prostatitis.
*TURP: Transurethral resection of the prostate NB: Needle biopsy. BPH: Benign prostatic hyperplasia. NSGP: Nonspecific granulomatous prostatitis. NL: Normal limits