Dexmedetomidine as an Adjuvant to Pre-Emptive Caudal Epidural Ropivacaine for Lumbosacral Spine Surgeries
Sandhya Kalappa1, Raghavendra Biligiri Sridhara2, Saraswathi Kumaraswamy3
1 Associate Professor, Department of Anaesthesiology, Bangalore Medical College and Research Institute, Bangalore, India.
2 Assistant Professor, Department of Anaesthesiology, Bangalore Medical College and Research Institute, Bangalore, India.
3 Assistant Professor, Department of Anaesthesiology, Bangalore Medical College and Research Institute, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sandhya Kalappa, 261, I Cross, 12th Block, Nagarabhavi II Stage, Bangalore-560072, Karnataka, India.
E-mail: sr.carenow@gmail.com
Introduction
Pre-emptive caudal epidural is a proven technique for providing analgesia for spinal surgeries. Prolonged pain relief with no motor blockade is desired for early mobilisation.
Aim
Present study aimed to evaluate the effect of addition of Inj dexmedetomidine to caudal ropivacaine on the duration of analgesia, haemodynamic profile and the associated side effects.
Materials and Methods
In this prospective double-blind study a total of 60 patients undergoing lumbosacral spine surgery were randomised to receive 20 cc of pre-emptive caudal epidural injection of either inj ropivacaine 0.2% (Group R, n =30) or a mixture of Inj ropivacaine 0.2% and Inj dexmedetomidine 1 μg/kg (Group RD, n =30) under general anaesthesia after the patient was positioned prone for surgery. VAS scores, heart rate, blood pressures and time to rescue analgesia were recorded at regular intervals for the first 24 hours. Data analysis was carried out using Statistical Package for Social Science (SPSS, V 10.5 package).
Results
Mean VAS scores were significantly lower in the RD group for up to 12 hours following the caudal block. No clinically significant haemodynamic changes were noted in either of the groups. No other side effects were seen in both the groups.
Conclusion
These results suggest that inj dexmedetomidine is an effective additive to inj ropivacaine for pre-emptive caudal epidural analgesia in lumbosacral spine surgeries.
Caudal analgesia, Post-operative period, Spine surgeries
Introduction
Postoperative pain after lumbosacral spine surgeries originates from handling nociceptors and mechanoreceptors from the vertebrae, intervertebral disc, dura and nerve root sleeves, facet joint capsules, muscles, ligaments and fascias. Secondary to inflammatory process [1–3] pain persists long after primary surgical insult.
The average rate of lumbar spine surgeries is 1.7-2.2/1000 U.S Medicare enrolees [4]. Hundreds of thousands of spine surgeries are performed each year, and it is well known that these patients report high-severity postoperative pain [5,6]. Mitigating postoperative pain by the best possible and safest way is of highest priority. Caudal analgesia, when given pre-emptively prevents the establishment of central sensitisation and produces long lasting analgesia by blocking sensory input from both primary insult and secondary inflammatory injury [7]. Ropivacaine 0.2% was the choice of local anesthetic agent as it provides an advantage over bupivacaine with respect to safety index. Its selectivity towards sensory rather than motor blockade [8] also makes it the desirable drug as it allows the surgeons to assess the motor system postoperatively [9].
Single shot caudal block provides analgesia for 2-4 hours [10] but this can be further prolonged by adding adjuvants like opioids, ketamine, alpha2 agonists, adrenaline, etc. [11]. Dexmedetomedine a selective α2-agonist with safe pharmacokinetic profile is a good neuraxial adjuvant [12].
Aim
The aim of this study was to evaluate the role of pre-emptive caudal epidural analgesia for postoperative pain relief in lumbosacral surgeries and to compare the effect of adding 1μg/ kg of dexmedetomidine to Inj ropivacaine 0.2% with respect to duration of analgesia, haemodynamic effects and associated side effects.
Materials and Methods
After ethical committee clearance from the institute, informed consent from all the patients enrolled for the study was obtained. A total of 60 patients of either sex in the age group of 18-65 years belonging to American society of Anaesthesiologists physical status I or II scheduled for elective discectomy/laminectomy of the lumbosacral spine between Jan 2013 and Nov 2013 were included. Based on previous literature on VAS for two group randomised controlled study for the detection of minimum difference of 2.0 VAS score with 90% statistical power and 5% level of significance the sample size required was 58 with 28 in each group. But for better results and to account for any drop outs we chose 60 patients with 30 in each group. Patients with sacral anomaly, known hypersensitivity to local anaesthetics, those on cardiovascular medication, and with conditions contraindicating neuraxial blockade were excluded from the study.
During the preoperative evaluation all patients were familiarised with the linear Visual Analogue Scale (VAS) {0 – no pain and 10–worst imaginable pain}. Two anaesthesiologists and a blinded observer were involved with each patient. The patients were randomly allocated using a computer generated randomisation table into Ropivacaine (R) group and Ropivacaine with Dexmedetomedine (RD) group. After ensuring that all standard monitors like electrocardiogram, non-invasive blood pressure and pulseoximetry were in place anaesthesia was induced with inj fentanyl 2μg/kg, inj propofol 2mg/kg and endotracheal intubation facilitated by inj vecuronium 0.1mg/kg and then turned prone for the surgery. Caudal epidural injection was performed in the prone position under strict aseptic precautions. Position in the epidural space was confirmed using loss of resistance technique. Needle placement was also confirmed by the use of an image intensifier. The anaesthetist blinded to the contents of the syringe injected the same into the epidural space. Patients in the R group were given 20 ml of 0.2% ropivacaine and patients in group RD were given 1μg/kg of inj dexmedetomidine with 0.2% inj ropivacaine. Surgical incision was placed at least 20 minutes after the block giving sufficient time for the drug to get fixed.
Haemodynamic parameters like Heart Rate (HR), Systolic Blood Pressure (SBP), Mean Blood Pressure (MBP) and Diastolic Blood Pressure (DBP) were recorded before the block which was considered as the baseline and at regular intervals intraoperative and postoperatively. Hypotension was defined as 20% reduction in the systolic blood pressure from the baseline value and was treated with 6 mg of inj mephentermine. Inj atropine 0.6 mg iv was administered when the heart rate dropped to less than 20% of baseline or less than 50 beats/min. Anaesthesia was maintained (Minimum Alveolar Concentration- MAC 1 to 1.2) using oxygen, nitrous oxide and isoflurane along with intermittent boluses of vecuronium 1mg and inj fentanyl 25 μg every hour. Intravenous paracetamol 1 gm was given to all patients intraoperatively and the same was continued eight hourly for the first 24 hours. The patients underwent either a discectomy or a single level laminectomy. Injection neostigmine 0.04 mg/kg and inj glycopyrrolate 0.01 mg/kg were used for reversal of neuromuscular blockade. All patients were extubated awake after fulfilment of the extubation criteria. Patients were monitored for postoperative pain after they had completely recovered and regained consciousness from general anaesthesia and subsequently at 30 min, 1, 2, 4, 8, 12 and 24 hours thereafter. Pain was quantified using the VAS at regular intervals. Patients with VAS more than 3 were given the rescue analgesic inj diclofenac 75mg as an infusion. Associated side effects like nausea, vomiting, urinary retention, motor blockade were documented in the first 24 hours.
Statistical Analysis
The results were averaged (mean±SD) for continuous numerical data. The unpaired student t-test and chi-square test was used to determine whether there was a statistical difference between groups in the parameters (VAS and haemodynamics) measured. The ‘p’ < 0.05 was accepted as statistically significant. Sample size was determined by a cross over pilot study of 8 patients in both the groups to detect a projected difference of 35% between the two groups for duration of analgesia for Type 1 error (α) of 0.05 and power of study 0.8. Data analysis was carried out using Statistical Package for Social Science (SPSS, V 10.5 package).
Results
Total of 60 patients were enrolled in our study. No difference in the demographic profile was detected between the two groups as shown in [Table/Fig-1].
Comparison of demographic data between the two groups.
| R group | RD group | p-value |
|---|
| No. | 30 | 30 | |
| AGE(yrs) | 44.13 ± 13.27 | 43.67 ± 13.02 | 0.893 |
| SEX- M/F | 14/16 | 18/12 | |
| WEIGHT(kg) | 60.13 ± 9.57 | 55.90 ± 11.66 | 0.131 |
| HEIGHT(cms) | 158.31 ± 8.79 | 158.32 ± 7.51 | 0.995 |
| DURATION OF ANAESTHESIA (min) | 150 ± 41 | 137± 53 | 0.588 |
The difference between the two groups with regard to the duration of surgery was not statistically significant. The number of patients undergoing laminectomy and discectomy in both the groups were comparable.
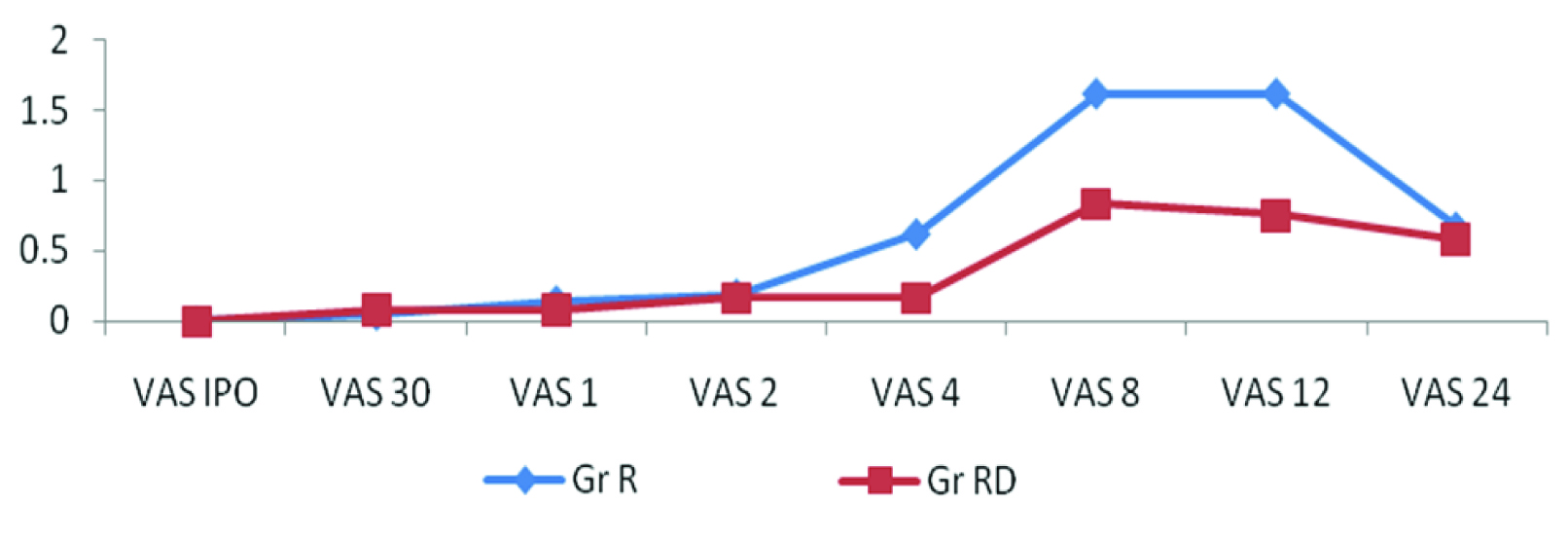
[Table/Fig-2] shows the mean VAS scores of the RD group were statistically lower at 4, 8 and 12 hours (p=0, 0, 0.006) compared to R group.
Mean VAS scores in at different time points between the two groups.
In [Table/Fig-3] heart rate showed a steady decline and the difference between the group reached statistically significant values at 4 hours* (R=81.75±9.89, RD=75.70±8.23, p=0.012) and 12 hours** (79.34±10.27, 74.80±6.66, p=0.046). Two patients in RD group had bradycardia.
Comparison of haemodynamic parameters at different time points between the two groups.
| Heart Rate | Systolic BP | Diastolic B P | Mean BP |
|---|
| Time | R | RD | ‘p’ | R | RD | ‘p’ | R | RD | ‘p’ | R | RD | p’ |
|---|
| Baseline | 88.31± 13.13 | 95.06± 14.53 | 0.065 | 130.96± 17.49 | 130.77 ±18.44 | 0.967 | 77.82± 9.61 | 80.25± 11.58 | 0.382 | 105.82± 15.51 | 103.51± 15.60 | 0.568 |
| 1 min | 82.82± 12.45 | 84.45 ±14.90 | 0.65 | 113.86 ±16.89 | 111.09 ±16.41 | 0.523 | 71.65± 7.51 | 71.35± 13.44 | 0.916 | 97.24 ±16.17 | 89.22± 16.35 | 0.061 |
| 3 min | 78.62 ±12.67 | 78.16 ±14.23 | 0.89 | 106.34± 16.10 | 102.83± 13.9 | 0.37 | 65.34± 8.59 | 67.29± 10.42 | 0.435 | 89.72± 15.39 | 85.80± 13.37 | 0.296 |
| 5 min | 74.37 ±12.77 | 74.90± 11.92 | 0.87 | 102.00± 15.13 | 99.51± 12.24 | 0.486 | 65.68± 8.00 | 64.83 ±9.76 | 0.715 | 86.96± 14.32 | 81.25± 11.01 | 0.088 |
| 10 min | 71.82 ±13.07 | 72.80 ±9.51 | 0.74 | 100.17 ±14.62 | 96.96± 14.59 | 0.399 | 63.79± 7.62 | 62.67± 9.75 | 0.625 | 84.96± 13.01 | 79.67± 11.86 | 0.105 |
| 15 min | 70.86 ±13.48 | 70.41± 9.31 | 0.88 | 100.96 ±14.98 | 96.74± 12.52 | 0.24 | 65.10± 8.73 | 63.03± 9.20 | 0.376 | 85.41± 13.47 | 79.58± 10.17 | 0.062 |
| 30 min | 69.51± 14.38 | 66.70± 7.92 | 0.34 | 99.51± 13.65 | 94.09± 12.25 | 0.111 | 63.55± 9.08 | 60.74± 11.42 | 0.298 | 82.17± 11.75 | 77.67± 11.95 | 0.148 |
| IPO | 87.27± 12.97 | 84.64± 15.27 | 0.47 | 126.37 ±11.76 | 125.77± 14.31 | 0.859 | 75.13± 8.38 | 80.22± 10.91 | 0.049 | 103.35± 14.19 | 102.22 ±14.07 | 0.76 |
| 30 min | 84.68± 11.28 | 80.35 ±12.49 | 0.165 | 123.62 ±10.54 | 121± 13.44 | 0.407 | 73.20± 7.66 | 76.35± 8.99 | 0.151 | 102.07± 11.50 | 98.03± 14.17 | 0.238 |
| 1 h | 83.86 ±9.99 | 79.48± 10.40 | 0.102 | 121.72± 11.26 | 120.41± 11.02 | 0.652 | 72.27± 6.09 | 74.32± 7.59 | 0.256 | 98.67 ±10.27 | 96.16± 12.66 | 0.408 |
| 2 h | 80.79± 10.25 | 76.29± 7.71 | 0.059 | 119.1 ±11.19 | 119.38± 9.54 | 0.916 | 72.24± 6.91 | 73.90± 7.81 | 0.388 | 99.07± 10.95 | 94.74± 12.11 | 0.157 |
| 4 h | 81.75± 9.89 | 75.70± 8.23 | 0.012* | 119.62± 12.16 | 115.90± 11.02 | 0.219 | 73.58± 9.61 | 72.19± 7.49 | 0.533 | 98.78± 13.29 | 93.25± 12.59 | 0.107 |
| 8 h | 79.68 ±9.99 | 75.67± 6.86 | 0.074 | 121 ±11.17 | 118.77 ±10.57 | 0.431 | 73.86± 7.27 | 73.09± 7.39 | 0.688 | 97.82± 12.95 | 95.80± 13.85 | 0.567 |
| 12 h | 79.34± 10.27 | 74.80± 6.66 | 0.046** | 121.24± 11.37 | 119.93± 10.87 | 0.651 | 72.68 ±6.93 | 71.83 ±7.19 | 0.643 | 99.25± 12.06 | 93.93± 12.90 | 0.109 |
| 24 h | 78.89 ±9.27 | 76.09± 6.20 | 0.172 | 123.31± 10.78 | 119.06 ±11.01 | 0.137 | 73.82 ±6.86 | 73.45 ±7.00 | 0.835 | 99.85± 12.48 | 94.80± 12.73 | 0.13 |
Blood pressures were relatively stable in both the groups. Systolic BP and mean BP were comparable between the groups while diastolic BP in RD group at immediate postoperative period was statistically higher compared to the R group (R=75.13±8.38, RD= 80.22±10.91, p=0.049).
Time to rescue analgesic in Group RD ranged from 420-444 min (Avg=432, SD=6.70) and 422-490 min (Avg=456, SD=10.89) in Group R. The p-value was <0.0001.
Discussion
Achieving adequate pain relief in the postoperative period not only ensures patient comfort but also optimises recovery by aiding early ambulation. Following surgeries on the spine the need to assess neurologic function while providing superior analgesia with minimal side effects remains the goal. Caudal epidural block is a simple and effective means of relieving pain after lumbosacral spine surgeries [13]. Pre-emptive caudal analgesia was used in this study as earlier studies have shown good postoperative analgesia and favourable outcome [7,13–16]. Patients are positioned prone for lumbosacral spine surgeries which also facilitated performing a caudal block [17]. Sekar c et al., compared 82 patients receiving pre-emptive caudal single shot 20 cc of bupivacaine and tramadol for lumbosacral spine surgeries. They inferred that the study group had VAS score significantly lower at all the time intervals than control group which received normal saline [7]. Kakiuchi M et al., concluded that pre-incisional caudal injection of bupivacaine and buprenorphine relieves postoperative wound pain on the lumbar spine performed under general anaesthesia [14]. Kundra et al., conducted a study in 60 patients for pain relief after lumbar laminectomies comparing pre-emptive caudal morphine with postoperative caudal morphine and found that VAS at eight hour, time for first postoperative analgesia and postoperative morphine consumption to be much lower and significant with pre-emptive caudal epidural morphine [15]. Ropivacaine 0.2% was the choice of local anaesthesia which provides an advantage over bupivacaine with respect to central nervous system and cardiovascular system safety index [9,18,19] and selectivity towards sensory rather than motor blockade [8]. Hence it is an ideal drug to assess the motor system postoperatively [9] and also helps in early mobilisation of the patient. Though a statistical analysis of the time to mobilisation was not done in our study most of the patients in both the study group were out of the bed by six hours postoperatively.
There is no proper consensus regarding dose of dexmedetomedine to be used for neuraxial blocks [20] and a dose of 1 μg/kg was used in our study which was similar to study conducted by Saravana Babu MS et al., They compared epidural ropivacaine and dexmedetomedine 1μg/kg with ropivacine and clonidine 2μg/kg in 60 patients for spine surgeries given postoperatively and found dexmedetomedine as neuraxial adjuvant is better for prolonging duration of analgesia and for cardio respiratory stability [21]. Fawzi MH et al., also used same dose with good results [13].
The 11 point linear Visual Analogue Scale (VAS) being a reliable validated score for assessing acute postoperative pain was used in our study [22,23]. The mean VAS score at postoperative 4 hour, 8 hour and 12 hour were statistically lower in RD group compared to R group. Though the difference in the score was statistically significant the mean score in both the groups was less than 3 indicating adequate analgesia upto 12 hours. The time to first rescue analgesic was prolonged in the RD group compared to the R group and it was statistically significant. Haemodynamic alterations can occur following caudal block which is attributable to ropivacaine and dexmedetomidine [13,24]. In our study heart rate and blood pressures were in a clinically acceptable range. Two patients in RD group had bradycardia which was treated with atropine 0.6mg stat. So 0.2% of ropivacaine and 1 μg/kg of dexmedetomidine seem to cause no haemodynamic disturbance of clinical significance. No other complications were noted in either of the groups.
Limitation
The limitations of the present study were that the sedation scoring was not done postoperatively which is one of the commonest side-effect of α2 adrenergic agonists. The time to mobilize postoperatively was not studied either considering that the neurosurgical team had a definite protocol in this regard and randomisation was not possible.
Conclusion
Pre-emptively given caudal block with 0.2% ropivacaine and 1 μg /kg dexmedetomidine provides excellent analgesia for prolonged duration in lumbosacral spine surgeries with minimal haemodynamic side effects while preserving good motor function facilitating neurological assessment and early ambulation.
[1]. Waddell G, The back pain revolution 2004 2nd editionEdinburgh (UK)Churchill Livingstone [Google Scholar]
[2]. McMahon S, Wall and Melzack’s textbook of pain 2006 5th editionPhiladelphiaElsevier, Churchill Livingstone [Google Scholar]
[3]. Devereaux MW, Neck and low back painMed Clin North Am 2003 87:643-62. [Google Scholar]
[4]. Weinstein JN, Lurie JD, Olson P, Bronner KK, Fisher ES, Morgan TS, United states trends and regional variations in lumbar spine surgery: 1992–2003Spine (Phila Pa 1976) 2006 31(23):2707-14. [Google Scholar]
[5]. Bianconi M, Ferraro L, Ricci R, The pharmacokinetics and efficacy of ropivacaine continuous wound installation after spine fusion surgeryAnesth Analg 2004 98:166-72. [Google Scholar]
[6]. Cata JP, Noguera EM, Parke E, Patient controlled Epidural Analgesia (PCEA) for postoperative pain control after lumbar spine surgeryJ Neurosurg Anaesthesiol 2008 20(4):256-60. [Google Scholar]
[7]. Sekar C, Rajasekaran S, Kannan R, Reddy S, Shetty TA, Pithwa YK, Pre-emptive analgesia for postoperative pain relief in lumbosacral spine surgeriesSpine J 2004 4(3):26 [Google Scholar]
[8]. Hansen TG, Ropivacaine: a pharmacological reviewExpert Rev Neurother 2004 4:781-91. [Google Scholar]
[9]. Graf BM, Abraham I, Eberbach N, Kunst G, Stowe DF, Martin E, Differences in cardiotoxicity of bupivacaine and ropivacaine are the result of physicochemical and stereoselective propertiesAnesthesiology 2002 96:1427-34. [Google Scholar]
[10]. A Sakarya University Medical SchoolCaudal epidural block in children and infants: Retrospective analysis of 2088 casesAnn Saudi Med 2011 31(5):494-97. [Google Scholar]
[11]. Vetter TR, Carvallo D, Johnson JL, Mazurek MS, Presson RG, A comparison of single-dose caudal clonidine, morphine, or hydromorphone combined with ropivacaine in pediatric patients undergoing ureteral reimplantationAnesth Analg 2007 104:1356-63. [Google Scholar]
[12]. Bajwa SJS, Bajwa SK, Dexmedetomidine and Clonidine in Epidural anaesthesia: A comparative evaluationIndian Journal of Anaesthesia 2011 55:116-21. [Google Scholar]
[13]. Fawzi HM, Almarakbi WA, Effects of pre-emptive caudal dexmedetomedine-bupivacaine mixture in adult patients undergoing single level lumbar laminectomy: A prospective randomized studyAin Shams Journal of Anaesthesiology 2012 5:223-28. [Google Scholar]
[14]. Kakiuchi M, Abe K, Pre-incisional caudal epidural blockade and the relief of pain after lumbar spine operationsInternational Orthopaedics (SICOT) 1997 21:62-66. [Google Scholar]
[15]. Kundra P, Gurnani A, Bhattacharya A, Preemptive epidural morphine for postoperative pain relief after lumbar laminectomyAnesth Analg 1997 85(1):135-58. [Google Scholar]
[16]. Kundra P, Deepalakshmi K, Ravishankar M, Pre-emptive caudal bupivacaine and porphine for postoperative analgesia in childrenAnesth Analg 1998 87:52-56. [Google Scholar]
[17]. Hadzic A, The New York School of Regional Anesthesia: Textbook of Regional Anesthesia and Acute Pain Management 2007 New YorkMcGraw-Hill Medical:269-283.:727-45. [Google Scholar]
[18]. Dony P, Dewinde V, Vanderick B, Cuignet O, Gautier P, Legrand E, The comparative toxicity of ropivacaine and bupivacaine at equipotent doses in ratsAnesth Analg 2000 91:1489-92. [Google Scholar]
[19]. Knudsen K, Beckman Suurküla M, Blomberg S, Sjövall J, Edvardsson N, Central nervous and cardiovascular effects of i.v infusions of ropivacaine, bupivacaine and placebo in volunteersBr J Anaesth 1997 78:507-14. [Google Scholar]
[20]. Sudheesh K, Harsoor SS, Dexmedetomedine in anaesthesia practice: a wonder drug?Indian Journal of Anaesthesia 2011 55:323-24. [Google Scholar]
[21]. Saravana Babu MS, Verma AK, Agarwal A, Tyagi CM, Upadhyay M, Tripathi S, A comparative study in the postoperative spine surgeries: Epidural ropivacaine with dexmedetomidine and ropivacaine with clonidine for Postoperative analgesiaIndian J Anaesth 2013 57:371-76. [Google Scholar]
[22]. DeLoach LJ, Higgins MS, Caplan AB, Stiff JL, The visual analogue scale in the immediate postoperative period: intrasubject variability and correlation with a numeric scaleAnesth Analg 1998 86:102-06. [Google Scholar]
[23]. VAS-Frca.co.uk [Internet]. UK: Assessment of acute and chronic pain, [updated 2009 Jan 12]. [Cited 2011 Oct 3] Available from: www.frca.co.uk/article.aspx?articleid=100549 [Google Scholar]
[24]. Schnaider TB, Vieira AM, Brandao ACA, Lobo MVT, Intraoperative analgesic effect of epidural ketamine, clonidine or dexmedetomidine for upper abdominal surgeryRev Bras Anestesiol 2005 55:525-31. [Google Scholar]