Introduction
Atherosclerosis is derived from the Greek words athero (meaning gruel or paste) and sclerosis (hardness) [1]. Atherosclerosis results into ischemic heart disease, cerebrovascular accidents and peripheral vascular diseases [2,3]. Progressive atherosclerotic disease results into pathological intimal thickening, fibrous cap atheroma and plaque formation. Early detection helps to control the disease in patients who are at risk [4].
It is the leading cause of morbidity and mortality all over the world. Modifiable risk factors associated with the disease include diabetes mellitus (DM), hypercholesterolaemia, hypertension and smoking. Non modifiable risk factors are gender, race and family history [5].
Carotid ultrasound is presently used as an adjunct to evaluate the risk of coronary disease. B-mode ultrasound has been considered as the modatily of choice for the evaluation of carotid intima media thickness. So, the present study was conducted to evaluate the prevalence of atherosclerosis, haemodynamic and morphological changes that take place in extra cranial portion of carotid arteries in patients with risk factors of atherosclerosis (Diabetes Mellitus, Hypertension, Smoking, Stroke, Coronary Artery Disease, Hyper-cholesterolaemia) and determine the association of risk factors with carotid abnormalities.
Materials and Methods
This is a prospective analytical study done from June 2013 to May 2015 in our institution. All patients above 60 years of age presenting with risk factors of atherosclerosis (Diabetes Mellitus, Hypertension, Smoking, Stroke, Coronary Artery Disease, Hypercholesterolaemia) were included in this study and the prevalence of atherosclerosis, haemodynamic and morphological changes that take place in extracranial carotid arteries was evaluated. Also, the association of risk factors with carotid abnormalities was assessed. Patients who did not give consent for examination were excluded.
Technique: An informed consent was obtained prior to study after explaining the procedure of the examination to the patient. Study was carried out using real time ultrasound equipment capable of B-mode imaging, pulsed–wave duplex scanning, and colour Doppler flow imaging and power Doppler imaging GE LOGIQ P5 PRO Ultrasound system with 8-12 MHz. The patient was placed in supine or semisupine with head slightly hyper-extended and rotated 45° away from the side being examined. Scan was done in both transverse and longitudinal plane and common carotid artery, bulb, external carotid artery (ECA) and internal carotid artery were examined bilaterally.
Interpretation of images: In all cases B-mode imaging, colour Doppler and spectral analysis were done for determination of the presence and extent of plaque.
Evaluation of IMT
The normal carotid wall exhibits two nearly parallel echogenic lines, separated by an anechoic region. The echogenic lines are created by lumen intima interface and media-adventitia interface. The distance between the two lines constitutes the intima-media thickness [Table/Fig-1].
B mode ultrasound images of common carotid artery for assessment of intima media thickness represented by calipers.

The maximum wall thickness of the common and internal carotid artery was defined as the mean of the maximum (m) wall thicknesses for near (N) and far (F) wall (W) on both the left (L) and right (R) sides: mLNW + mLFW + mRNW + mRFW/4 [6]. The values >0.8mm were considered abnormal [7,8].
Evaluation of Plaques
Plaque was defined as the intima media thickness more than 1.2mm [9]. The extent, location, and characteristics (low echogenic, moderately echogenic, highly echogenic and calcified) of atherosclerotic plaque in the carotid vessels were documented with gray-scale imaging. Colour Doppler imaging was performed to detect areas of abnormal blood flow that require Doppler spectral analysis. Images of the plaque were taken in two directions- short axis and long axis views of the blood vessel.
Pulsed wave Doppler spectral analysis was performed, and the velocity of blood flow in the mid-CCA and proximal ICA as well as proximal to, at, and immediately distal to the diseased areas was measured.
Calculation of Percent Stenosis
NASCET method [10] was used for evaluation of stenosis at the origin of the internal carotid artery, which is more likely to develop stenosis [11]. With NASCET method, the criterion vascular diameter is the diameter of the intact area of the ICA distal to the stenosed area where the diameter is stable. The ICA stenosis was graded according to criteria suggested by Society of Radiologists in Ultrasound Consensus Conference [12]. ICA PSV (cm/sec) and additionally ICA/CCA PSV Ratio were calculated.
Spectral Waveform Analysis
Common carotid artery has moderately broad systolic peaks and a moderate amount of flow throughout diastole. Normal ICA demonstrated low resistance flow, whereas a normal ECA showed high resistance flow.
Statistical Analysis
The results were presented in number and percentage for the data in table and figures.
Relationship of association of risk factors with wall thickness & stenosis was established using multiple regression analysis, variance analysis & mean study using SPSS 17.0. Also, inference study was done for relations of risk factors and their association with age and sex of the cases observed. In multiple linear regression analysis, values of p<0.05 were considered statistically significant.
Results
Amongst all the observed risk factors, diabetes, smoking and history of stroke showed positive correlation with maximum mean wall thickness of common carotid arteries. For internal carotid arteries wall thickness, hypertension, diabetes, hypercholesterolaemia and history of heart disease showed significant positive correlation. Risk factors such as obesity, left ventricular hypertrophy and major electrocardiographic abnormality did not show much significant correlation with any of the carotid artery measures.
Maximum percent stenosis increased with an increase in age. It was more prevalent in men than women (42% men compared to 26.79% women). Across men, numbers of cases with stenosis observed in age group of 65-70 were 20% more than in age group of 60-65. No significant trend was observed in women. Cases with risk factors of diabetes, smoking, high cholesterol levels, heart disease and stroke showed maximum mean values. Smoking (0.1685) and heart disease (0.1628) showed maximum positive correlation with stenosis, this was evaluated using multiple logistic regressions using SPSS 17.0 [Table/Fig-2]. Among 1043 cases, stenosis was observed in 354(33.9%) patients. Number of patients with significant stenosis, i.e., stenosis >50% were 63(17.8%) and cases with mild stenosis were 291(82.20%). Maximum percentage of population showed mild stenosis. Maximum percent stenosis increases with the increase in age and it was more in men than women [Table/Fig-3].
Association of risk factors with common and internal carotid IMT and stenosis using multiple logistic regression analysis.
| Risk Factor | Common IMT- Adjusted R2 | Internal IMT- Adjusted R2 | Stenosis-Adjusted R2 |
|---|
| Hypertension | 0.1285 | 0.2930 | 0.1340 |
| Smoking | 0.1518 | 0.1077 | 0.1685 |
| Diabetes | 0.1516 | 0.1962 | 0.1447 |
| Obesity | 0.0076 | 0.0207 | 0.0035 |
| LVH On ECG | 0.0292 | 0.0533 | 0.0155 |
| Major ECG Abnormality | 0.0065 | 0.0088 | 0.0062 |
| Hypercholesterolaemia | 0.1005 | 0.1823 | 0.1372 |
| H/O Heart Disease | 0.1180 | 0.2156 | 0.1628 |
| H/O Stroke | 0.1123 | 0.0107 | 0.0712 |
Correlation of max. Stenosis with age and sex
| Stenosis % | 60-64 Years | 65-70 Years | 70-74 Years | 75+ Years | Total |
|---|
| Female | Male | Female | Male | Female | Male | Female | Male | Female | Male |
|---|
| NORMAL | 156 (38.23%) | 74(26.52%) | 162(39.70%) | 92(32.97%) | 68(16.67%) | 59(21.14%) | 22(5.39%) | 54(19.35%) | 408 | 279 |
| MILD <50% | 27 (21.09%) | 39(23.63%) | 60(47.61%) | 60 (35.92%) | 30(23.43%) | 39 (23.35%) | 10 (7.81%) | 27(16.36%) | 126 | 165 |
| MODERATE50-69% | 8 (42.10%) | 5 (17.24%) | 7(36.84%) | 10 (34.48%) | 3(15.78%) | 7(24.13 %) | 1 (5.26%) | 7(24.13%) | 19 | 29 |
| SEVERE>/= 70 | 0 | 1 (14.28%) | 0 | 4 (57.14%) | 1 (100%) | 1 (14.28%) | 0 | 1 (14.28%) | 1 | 7 |
Severe stenosis i.e. ≥ 70% was found in 7 males (3.4%) and 1 woman (0.6%). Near occlusion was observed in 2 men and one woman. Same was observed for total occlusion. The commonest lesion was atherosclerotic plaque. Majority of the plaques were low echogenic 142 (40%), followed by calcified plaque 99 (28%), moderately echogenic 24 (7%) and 89 (25%) hyperechogenic plaque. Maximum cases of plaque were observed on the right side (44%) followed by bilateral (30%) and left side (26%). Analysis of the site of involvement showed maximum plaque at bifurcation (35% on right side and 41% on left side). No significant pattern was observed for involvement of CCA, ICA and ECA across left and right side.
Correlation between percentage stenosis and spectral velocity changes was evaluated. Peak systolic velocity (PSV) range also increased in proportion to stenosis. Highest PSV was found at the point of most severe stenosis. There were 63 cases (17.8%) with PSV >125 cm/sec. Additionally ICA/CCA PSV ratio was also calculated which showed proportional increase with the increase in PSV.
Discussion
The study was done to evaluate the extracranial carotid arterial system by carotid Doppler in the population who presented with risk factors of atherosclerosis (diabetes mellitus, hypertension, smoking, obesity, coronary artery disease, and stroke).
Angiography as the “Gold Standard” has amply been replaced by duplex ultrasonography in most diagnostic circumstances. Positive experience with carotid duplex ultrasonography scanning unassisted by angiography in the setting of an impending surgical intervention has been embraced by many doctors [13].
Carotid Doppler examination aids in determining the occlusive lesions in the carotid vessels. Patients with severe stenosis (≥ 70%), are at increased risk of developing cerebral infarction.
From the total 1043 patients studied, there were 556 females (53.3%) and 487 males (46.7%). The prevalence and severity of carotid atherosclerosis continued to increase with age among the elderly, and more disease was found in men than in women at all ages. This corresponds to study by Tegos et al., [14].
The commonest lesion was atherosclerotic plaque. Of the 1043 patients examined, 354 patients (33.94%) had plaque. The plaques were classified according to their anatomical location. The right side was affected more than the left side. This finding is similar to Sehrawat et al., [13]. In our study, 155 patients (44%) had right side involvement as compared to 92 on left side (26%), 106 patients had bilateral involvement i.e. both right and left side.
Sethi et al., and Rajagopal et al., found that the carotid bifurcation was commonly involved by the atherosclerotic plaque followed by ICA and intracranial portions of ICA [7,15]. In our study also, the bifurcation was the commonest site affected by the plaque followed by ICA. Out of 262 plaques on right side, 92 plaques (35%) were present at bifurcation, 84 (32%) plaques in ICA followed by 21(8%) in ECA. Out of total 198 plaques on left side, 82 (41%) plaques were present at bifurcation, 23 (12%) in ECA and 58 (29%) involved ICA. Plaques are more common at bifurcation due to transient reversal of flow, flow separation and eddy formation in these areas [16].
Plaques were also categorized according to their echotexture as low echogenic, moderately echogenic, hyperechogenic and calcified plaques. Plaque characterization is important as low echogenic plaques (either homogenous or heterogeneous) are prone to dislodge into cerebral circulation and cause transient ischemic attack [17]. In our study, out of total 354 who had plaque, 142 patients (40%) had low echogenic plaques [Table/Fig-4]. Any intra plaque haemorrhage could not be appreciated. Sehrawat et al., [13] found the maximum (45%) of low echogenic plaques.
Colour Doppler image in a 70-year-old male patient who presented with history of stroke, diabetes mellitus and hypertension, showing low echogenic plaque at proximal right ICA, shown by calipers
George Howard [18] suggested that risk factors show their association with development of atherosclerosis with progression in age. Correlation between risk factors of atherosclerosis, wall thickness of common carotid and internal carotid and stenosis was studied using multiple logistic regression analysis and analysis of variance (p<0.05). In our study, Hypertension showed strongest positive correlation with carotid artery disease. Risk factors like smoking, diabetes mellitus, hypercholesterolaemia, cardiovascular disease also showed association with all three measures (common carotid intima-media thickness, internal carotid intima-media thickness and maximum percent stenosis).
In a study by O’Leary et al., maximum stenosis and maximum wall thickness measurements increased with age and were uniformly greater at all ages in men than in women (p<0.00001) [6]. Also, in their study, established risk factors for atherosclerosis (hypertension, smoking, diabetes) and indications of vascular disease (left ventricular hypertrophy, major electrocardiographic abnormality, bruits, and history of heart disease or stroke) were related to all three carotid artery measures in the elderly. Our findings correlate with this study.
Out of 354 cases who had stenosis, the prevalence of mild stenosis (<50%) was quite large, 291 (82.20%) cases [Table/Fig-5,6]. However, the prevalence of severe stenosis (>50%) was quite low, 13.42% in women and 17.56% in men. This correlates with study by O’Leary et al., in 5201 men and women, the prevalence of severe stenosis (>50%) was low, 7% in men and 5% in women [6]. Out of 1043 cases studied, 3 had near occlusion and 3 cases showed complete occlusion of the vessel.
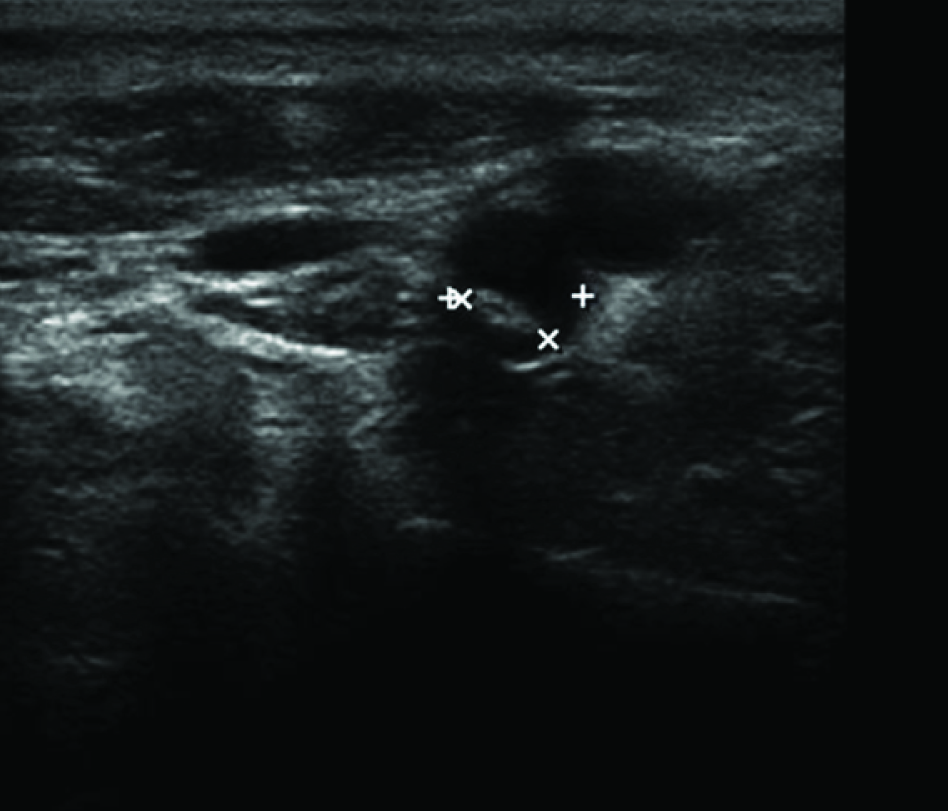
Transverse ultrasound image shows Hyperechogenic Plaque in the Right ICA causing 28.4% diameter stenosis.

In a 65-year-old male presented with History of Heart disease. He had history of smoking since 15 years and his laboratory investigations showed increased LDL-C levels (greater than 240mg/dl) and fasting glucose levels (>126mg/dl). Transverse and Longitudinal ultrasound image shows hypoechoic plaque in Left CCA Bifurcation causing 47% diameter stenosis.

A study by Robinson et al., states that the imaging characteristics of complete carotid occlusion include absence of arterial pulsation [19], presence of an echogenic material filling the lumen, subnormal vessel size which suggests chronic occlusion and Doppler flow showing absence of signals or weak signals. In our study, all the cases of complete carotid stenosis showed the above features.
Analysis of spectral waveform of the stenosed vessel was also done to determine the associated changes [Table/Fig-7]. According to the criteria mentioned by Grant et al., (PSV >140 cm/sec in > 70% stenosis), in our study, PSV showed an increase with an increase in stenosis [12]. PSV is considered the best parameter since it is easy to measure and due to the increase in specificity with increase in stenosis. Grant et al., also found that mean PSV increased with increased stenosis level [20]. As stated by Tahmasebpour et al., if the degree of stenosis is indeterminate according to the primary parameters, the ICA/CCA PSV ratio to be taken as an additional parameter [21].
In a 65-year-old male patient presented with history of stroke, diabetes mellitus and hypertension. Image showing plaque in the right ICA, haemodynamic changes (PSV >51cm/s) and Parvus tardus waveform on spectral analysis

Grant et al., stated the criteria for the ICA/CCA PSV ratio, which quotes, the values in the range of 2.0- 4.0 when the degree of stenosis for ICA is in the range of 50- 69 % and values are more than 4.0 when the degree of stenosis for ICA is >70 % (but less than near occlusion) [12].
According to this criteria, we found the maximum number of patients, 291 cases (82.20%) with stenosis, had ICA/CCA PSV ratio less than <2.0, corresponding to mild stenosis (<50%). The prevalence of ICA/CCA PSV ratio >2.0 was quite low (17.8%). This parameter thus confirmed the degree of stenosis.
Limitations
There are few limitations in our study, on duplex sonography; calcified plaque in a carotid artery obscured the area of examination due to its posterior acoustic shadowing. However, the change in position to postero-lateral view was helpful in some cases, especially those involving the smaller segment of vessels (<1cm) but those involving the larger segment of vessel were difficult to examine. Also, patients with short neck, tortuous vessels and those with high carotid bifurcation, limited the field of examination.
Conclusion
Maximum mean IMT for Common and Internal carotid arteries was increased in patients with risk factors as compared to those who did not. Maximum mean wall thickness of common carotid artery was predominantly found to be associated with risk factors of diabetes mellitus, smoking and hypertension. Maximum mean wall thickness of Internal Carotid Artery showed strong positive association with Hypertension, history of Heart Disease.
Percent stenosis increased with an increase in age and was more prevalent in men than women. Smoking and heart disease showed maximum positive correlation with Stenosis. Prevalence of severe stenosis (>70%) was low while the prevalence of mild stenosis (<50%) was quite high. Stenosis was more profound in terms of frequency and severity in men at all ages than women. Atherosclerotic plaques were mostly found at the site of carotid bifurcation. Peak systolic velocity (PSV) range increased with an increase in severity of stenosis. ICA/CCA PSV ratio showed proportional increase with the increase in PSV.
[1]. Mitchell RN, Schoen FJ, Blood Vessels. In : Kumar V, Abbas AK, Fausto N, Aster J, editorsPathologic Basis of Disease 2013 8th edPhiladelphiaElsevier:487-52. [Google Scholar]
[2]. Ross R, Atherosclerosis-an inflammatory diseaseN Engl J Med 1999 340:115-25. [Google Scholar]
[3]. Butt MU, Zakaria M, Association of common carotid intimal medial thickness (CCA-IMT) with risk factors of atherosclerosis in patients with type 2 diabetes mellitusJ Pak Med Assoc 2009 59:590-93. [Google Scholar]
[4]. Touboul PJ, Labreuche J, Vicaut E, Amarenco P, Genic Investigators. Carotid intima-media thickness, plaques, and Framingham risk score as independent determinants of stroke riskStroke 2005 36:1741-45. [Google Scholar]
[5]. Davies MJ, Woolf N, Atherosclerosis: what is it and why doesitoccur?BrHeart J 1993 69(1 Suppl):S3-11. [Google Scholar]
[6]. O’Leary DH, Polak JF, Kronmal RA, Distribution and correlates of sonographically detected carotid artery disease in the Cardiovascular Health Study. The CHS Collaborative Research GroupStroke 1992 23:1752 [Google Scholar]
[7]. Sethi SK, Solanki RS, Gupta H, Colour and duplex doppler imaging evaluation of extracranial carotid artery in patients presenting with transient ischaemic attack and stroke : a clinical and radiological correlationIndian J Radiol Imaging 2005 5:91-98. [Google Scholar]
[8]. Jadhav UM, Kadam NN, Carotid Intima-Media thickness as an independent predictor of coronary artery diseaseIndian Heart J 2001 53(4):458-62. [Google Scholar]
[9]. Bathala L, Mehndiratta MM, Sharma VK, Cerebrovascular ultrasonography: Technique and common pitfallsAnn Indian Acad Neurol 2013 16(1):121-27. [Google Scholar]
[10]. North American Symtomatic Carotid Endarterectomy Trial Collaborators: Beneficial effect of carotid stenosisN Engl J Med 1991 325:445-53. [Google Scholar]
[11]. Terminology and Diagnostic Criteria Committee. Japan Society of Ultrasonics in MedicineStandard method for ultrasound evaluation of carotid artery lesionsJpn J Med Ultrason 2009 36:510-18. [Google Scholar]
[12]. Grant EG, Benson CB, Moneta GL, Alexandrov AV, Baker JD, Bluth EI, Carotid artery stenosis: gray-scale and Doppler US diagnosis— Society of Radiologists in Ultrasound Consensus ConferenceRadiology 2003 229(2):340-46. [Google Scholar]
[13]. Sehrawat S, Thind SS, Singh V, Rajesh R, Naware S, Shrotri H, Colour Doppler evaluation of extracranial carotid artery in patients presenting with features of cerebrovascular disease: A clinical and radiological correlationMedJ DY PatilUniv 2012 5:137-43. [Google Scholar]
[14]. Tegos TT, Kalodiki E, Sabetai MM, Nicolaides AN, The genesis of atherosclerosis and risk factors - A reviewAngiology 2001 52(2):89-98. [Google Scholar]
[15]. Rajagopal KV, Lakhkar BN, Banavali S, Singh NK, Pictorial essay- colour duplex evaluation of carotid occlusive lesionsInd J Radiol Imag 2000 10(4):221-26. [Google Scholar]
[16]. Philips DJ, Green FM Jr, Langlois Y, Roederer GO, Strandness DE, Flow velocities in carotid bifurcation of young presumed normal subjectsUltrasound Med Biol 1983 9:399 [Google Scholar]
[17]. Seeger JM, Barratt E, Lawson GA, Klingman N, The relationship between carotid plaque composition, plaque morphology, and neurologic symptomsJ Surg Res 1995 58:330-36. [Google Scholar]
[18]. Howard G, Manolio TA, Burke GL, Does the association of risk factors and atherosclerosis change with age? An analysis of the combined ARIC and CHS cohorts. The Atherosclerosis Risk in Communities (ARIC) and Cardiovascular Health Study (CHS) investigatorsStroke 1997 28:1693-701. [Google Scholar]
[19]. Robinson ML, Sacks D, Perlmutter GS, Marinelli DL, Diagnostic criteria for carotid duplex sonographyAJR Am J Roentgenol 1988 151:1045-49. [Google Scholar]
[20]. Grant EG, Duerinckx AJ, El Saden AM, Ability to use duplex US to quantify internal carotid arterial stenoses: fact or fiction?Radiology 2000 214:247-52. [Google Scholar]
[21]. Tahmasebpour HR, Buckley AR, Cooperberg PL, Sonographic Examination of the carotid arteriesRadiographics 2005 25:1561-75. [Google Scholar]