Multiple Isolated Enteric Duplication Cysts in an Infant - A Diagnostic Dilemma
Alok Kumar Udiya1, Gurucharan S Shetty2, Udit Chauhan3, Shweta Singhal4, Shailesh M Prabhu5
1 Senior Resident, Department of Radiodiagnosis, Institute of Liver and Bilary Sciences, New Delhi, India.
2 Senior Resident, Department of Radiodiagnosis, All India Institute of Medical Sciences, New Delhi, India.
3 Senior Resident, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
4 Senior Resident, Department of Radiodiagnosis, Lady Hardinge Medical College and assoc. SSK and KSC hospitals, Connaught Place, New Delhi, India.
5 Senior Resident, Department of Radiodiagnosis, CMC, Vellore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Alok Kumar Udiya, Senior Resident, Department of Radiodiagnosis, Lady Hardinge Medical College, New Delhi
E-mail: alok.udiya@gmail.com
Completely isolated enteric duplication cysts are a rare variety of enteric duplication cysts having an independent blood supply with no communication with any part of the adjacent bowel segment. We report a case showing two completely isolated enteric duplication cysts originating in the greater omentum and transverse mesocolon in an infant. Multiple isolated enteric duplication cysts involving non-contiguous bowel segments have not been previously reported in the literature. In addition the transverse mesocolon duplication cyst was infected showing septations and loss of double wall sign resulting in difficulty in imaging diagnosis. Both the cysts were excised and confirmed on histopathology.
Complicated, Isolated enteric duplication cysts, Omental, Transverse mesocolon
Case Report
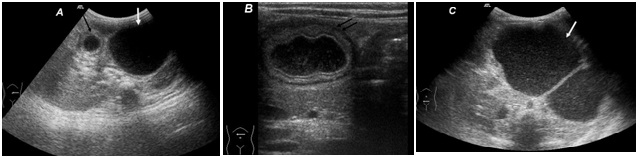
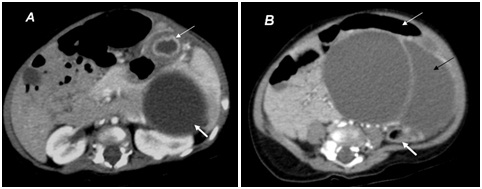
A seven-month-old male infant presented with progressively increasing abdominal distension of 2 month duration. No history of fever, vomiting or altered bowel habit was noted. Antenatal and perinatal history was insignificant and infant was exclusively breast fed. On clinical examination a large soft non tender mass was palpable on left side of abdomen. Plain X-ray revealed a soft tissue haze in left upper abdomen displacing the bowel loops. Initially ultrasound abdomen was done which revealed two separate cystic lesions in abdomen [Table/Fig-1a]. The smaller cystic lesion (3x3 cm) was thick walled and noted in relation to greater curvature of stomach and it showed the characteristic “double wall” sign (muscular rim sign) [Table/Fig-1b]. The larger cystic lesion (10x12cm) was located in the left lower abdomen inferior to the stomach extending across the midline and showed septations and internal echoes [Table/Fig-1c]. However, ultrasound revealed no continuity or connection between the cysts and adjacent bowel loops. Subsequently contrast enhanced CT of the abdomen was done to completely delineate the extent of lesions. The smaller thick walled cystic lesion seen on ultrasound showed enhancing inner and outer wall on CT [Table/Fig-2a] and was located in relation to the greater curvature of stomach. Another large well defined cystic lesion was noted in the left side of abdomen with enhancing septa, extending from lower pole of spleen to pelvis. This lesion was draped anteriorly by the transverse colon while the descending colon was displaced laterally [Table/Fig-2b]. An imaging diagnosis of transverse mesocolon lymphangioma with gastric duplication cyst was suggested. Surgical excision of both cystic lesions was done.
Ultrasound abdomen images showing: (a) two separate cystic lesions (white and black arrows); (b) Smaller cystic lesion showing double wall sign (black arrows) was seen in relation to greater curvature of stomach with no communication with wall; (c) A Large well defined cystic lesion (white arrow) with internal echoes and septations, pushing the left kidney posteriorly. Larger cystic lesion did not show double wall sign and it was misdiagnosed as transverse mesocolon lymphangioma but histopathologically this was diagnosed as infected colonic duplication cyst
Contrast enhanced CT images demonstrate: (a) two separate cystic lesions (thin and thick white arrow) with the smaller cystic lesion (thin white arrow) showing enhancing inner and outer wall and in relation to greater curvature of stomach; (b) The larger well defined cystic lesion (black arrow) shows thin wall with enhancing internal septa displacing the transverse colon (thin white arrow) anteriorly over the cyst and descending colon (thick white arrow) posteriorly
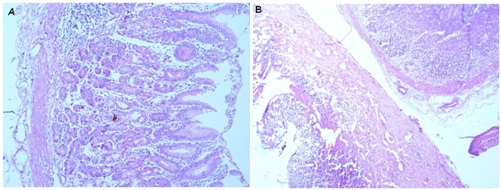
Per-operatively the large cystic lesion was lying in the transverse mesocolon while the smaller cystic lesion was seen attached to the greater omentum of stomach by a narrow stalk and had no communication with the gastric wall. Both lesions were excised without sacrificing any surrounding bowel. Histopathological examination of both cystic lesions was done. The examination revealed both the lesions as enteric duplication cysts, the smaller cystic lesion showed lining of gastric mucosa [Table/Fig-3a] and larger cyst showed inflammatory exudates, granulation tissues and an eroded epithelial lining with spared islands of colonic mucosa [Table/Fig-3b].
(a) High power photomicrograph of the smaller omental cyst showing stomach mucosa comprising of two epithelial compartments, depicting both foveolar and glandular arrangements and part of smooth muscle layer;(b) Low power photomicrograph of resected larger mesocolon cyst shows part of normal glandular mucosa and segment of partially necrosed cyst wall lined by fragmented mucosal epithelium
Discussion
Enteric duplication cyst is a rare congenital anomaly that occurs anywhere from the oral cavity to rectum [1]. Isolated enteric duplication cysts are characterised by the presence of the typical histopathological features of a duplication cyst with no connection with the adjacent alimentary tract [2].
Enteric duplication cysts can occur anywhere along the gastrointestinal tract commonly on mesenteric side of bowel [1]. Most of the enteric duplication cysts up to 75% are located in abdominal cavity, 20 % are intra-thoracic and 5% are thoraco-abdominal [3]. The small bowel is the most common site of involvement with terminal ileum being the most common location [4].
Several different theories have been proposed for embryological occurrence of duplication cyst in different locations which includes persistent of fetal gut diverticula, defect in solid stage of recanalization of primitive gut and partial twinning of the primitive gut [5].
Congenital anomalies like double bladder, double external genitals, double urethra, spinal deformities like hemivertebra, omphalocele, separation of pubic symphysis and cardiac anomalies have been reported with colonic duplication cyst [5]. Our patient did not have any of these reported congenital anomalies.
Multiple enteric duplication cysts have been reported previously in the literature with oesophageal duplication cyst associated with small bowel duplication being the most common combination. Other varieties of multiple enteric duplication cysts generally involve contiguous segments of bowel loops such as gastroduodenal and illeocaecal segments [6]. Completely isolated enteric duplication cysts are a rare variety of enteric duplication cysts having an independent blood supply with no communication with any part of the adjacent bowel segment [2]. On histopathology they show gastrointestinal lining epithelium and smooth muscle wall. Multiple isolated duplication cysts involving non contiguous bowel as in our case has not been previously reported in the literature. Both the cysts in our case were completely isolated from the adjacent bowel wall and were enclosed in peritoneal reflections of omentum and transverse mesocolon.
Most common imaging modalities used for the diagnosis of duplication cysts is barium studies and ultrasonography. The utility of barium studies are limited with few cases showing mass effect or extraluminal impression. Ultrasound is particularly useful in diagnosing enteric duplication cyst by demonstration of the double wall sign or muscular rim sign (Gut signature sign). “Double wall” represents an echogenic inner rim which corresponds to mucosa surrounded by a hypoechoic rim representing the smooth muscle layer. However, double wall sign is not specific for duplication cyst as it can be seen in cases of mesenteric cyst and cystic teratoma in which inner hyper echoic layer represents dystrophic calcification and outer layer represents fibrous layer which is termed as pseudo gut signature sign (false positive) [7].
In addition double wall sign may not be visible in all cases of enteric duplication cyst. Double wall sign may be lost in cases of infected duplication cyst (false negative) as in our case or due to enzymatic destruction of mucosal lining by ectopic rest of pancreatic tissue [7]. In presence of infection there may be ulceration of mucosal lining, septations and internal echoes within the cyst resulting in loss of characteristic appearance of a duplication cyst. The isolated nature and position of cyst in mesocolon with superadded infection as in our case resulted in an error of imaging diagnosis preoperatively.
Another imaging appearance of isolated enteric duplication cyst on ultrasonography is that of the pseudo kidney sign as described by Peng et al., [2]. This imaging appearance is a result of severe congestion of the wall resulting in complete circumferential loss of typical gut wall layers producing a thick hypoechoic rim while the opposition of the luminal surfaces resulted in the hyperechoic central layer.
CT scan and MRI have a role in cases in which multiplanar approach helps in the assessment of the anatomical relations of the cyst and associated anomalies. Tc 99 pertechnate scan has a role in detection of ectopic gastric mucosa with sensitivity of up to 75% [8].
Inoue Y et al., reviewed 18 cases of malignancy arising in duplication cyst and reported that frequency of malignancy is highest in colonic duplication cysts and most occur in adults [9]. Though the association of mesenteric lymphangioma with volvulus is well known few case reports also point to association of volvulus with duplication cyst [10]. These cases lend support to the hypothesis that a mass lesion like lymphangioma or duplication cyst may predispose the patient to volvulus.
Since isolated duplication cysts are rare, awareness of imaging appearances in presence of complications is essential for correct preoperative diagnosis. Once detected these lesions are better excised to prevent further complications.
The combined occurrence of multiple isolated duplication cysts in a single individual has been rarely reported in literature [11] and to our best knowledge the combined occurrence of gastric omental and transverse mesocolon duplication cyst has not been reported.
Conclusion
The presence of double wall sign helps in a confident diagnosis but its absence may not help rule out the possibility of duplication cyst entirely. Awareness of the varied imaging findings of isolated enteric duplications cysts may help in correct imaging diagnosis and appropriate management.
[1]. Menon P, Rao KL, Vaiphei K, Isolated enteric duplication cystsJ Paediatr sur 2004 39:5-7. [Google Scholar]
[2]. Peng HL, Su CT, Chang CY, Lau BH, Lee CC, Unusual imaging features of completely isolated enteric duplication in a childPediatr Radiol 2012 42:1142-44. [Google Scholar]
[3]. Stern LE, Warner BW, Gastrointestinal duplicationsSeminars in Pediatric Surgery 2000 9:135-40. [Google Scholar]
[4]. Pruksapong C, Donovan RJ, Pinit A, Heldrich FJ, Gastric duplicationJ Paediatr sur 1979 14:83-85. [Google Scholar]
[5]. Blickman JG, Rieu PHM, Buonomo C, Hoogeveen YL, Boetes C, Colonic duplications: Clinical presentation and radiologic features of five casesEuropean Journal of Radiology 2006 59:14-19. [Google Scholar]
[6]. Hur J, Yoon CS, Kim MJ, Kim OH, Imaging features of gastrointestinal tract duplications in infants and children: from ooesophagus to rectumPediatr Radiol 2007 37:691-99. [Google Scholar]
[7]. Cheng G, Soboleski D, Daneman A, Poenaru D, Hurl D, Sonographic Pitfalls in the Diagnosis of Enteric Duplication CystsAJR 2005 184:521-25. [Google Scholar]
[8]. Tong SC, Pitman M, Anupindi SA, Ileocecal Enteric Duplication Cyst: Radiologic-Pathologic CorrelationRadioGraphics 2002 22:1217-22. [Google Scholar]
[9]. Inoue Y, Nakamura H, Adenocarcinoma arising in colonic duplication cysts with calcification: CT findings of two casesAbdom Imaging 1998 23:135-37. [Google Scholar]
[10]. Okoro PE, Obiorah C, Duplication cyst of the bowel causing ileal volvulus. A case reportNiger J Med 2010 19:230-32. [Google Scholar]
[11]. Pant N, Grover JK, Madan NK, Chadha R, Agarwal K, Choudhury SR, Completely isolated enteric duplication cyst associated with a classic enterogenous duplication cystJournal of Indian Association of Pediatric Surgeons 2012 17(2):68-70. [Google Scholar]