Clinico-Radiologic Perspective of a Case of Hemifacial Microsomia
Mandakini Subhash Mandale1, Jyoti Dilip Bhavthankar2, Jayanti Govind Humbe3, Pritam Kumar Mankapure4
1 Assistant Professor, Department of Oral Pathology and Microbiology, Government Dental College and Hospital, Aurangabad, Maharashtra, India.
2 Associate Professor, Department of Oral Pathology and Microbiology, Government Dental College and Hospital, Aurangabad, Maharashtra, India.
3 Assistant Professor, Department of Oral Pathology and Microbiology, Government Dental College and Hospital, Aurangabad, Maharashtra, India.
4 Assistant Professor, Department of Oral Pathology and Microbiology, Government Dental College and Hospital, Aurangabad, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pritam Kumar Mankapure, Assistant Professor, Department of Oral Pathology, Government Dental College & Hospital, Dhanvantari Nagar, Aurangabad-431001, Maharashtra, India.
E-mail: pritammankapure@gmail.com
Congenital abnormalities, Craniofacial abnormalities, Facial asymmetry, Teratogens
The term hemifacial microsomia (HFM) was coined by Gorlin and Pindborg (1964) [1]. The spectrum of hemifacial microsomia involves malformation of ear with presence of preauricular skin tags, hypoplasia of mandibular ramus, condyle, maxilla, zygomatic and temporal bones, hypoplasia of facial muscles with soft tissue deficiency and orbital deformity [2]. We report a case of hemifacial microsomia with emphasis on its clinico-radiological features.
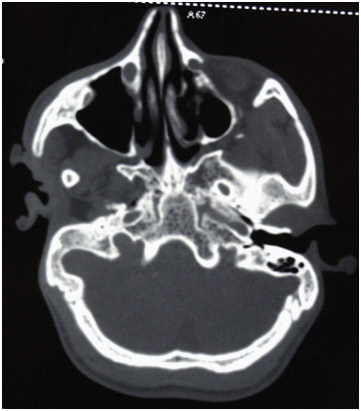
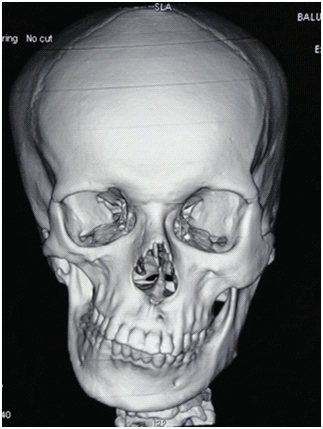
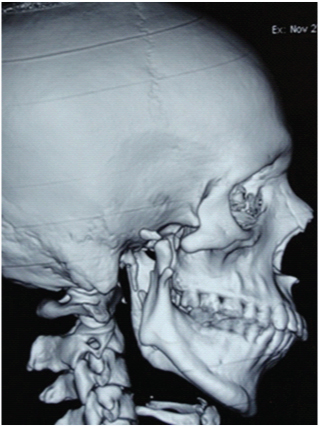
A 25-year-old male patient presented with complaint of facial asymmetry and difficulty in hearing since birth. The medical, dental, and family history was non-contributory. Extra oral examination revealed obvious facial asymmetry [Table/Fig-1], deviated chin, deformed and low set auricle with large preauricular skin tag [Table/Fig-2], and posteriorly placed corner of mouth resulting in macrostomia on right side of face. Intraorally posterior cross bite, and upward displacement of occlusal cant on right side was seen. The patient was clinically diagnosed as HFM of the right side of the face. Conventional CT scan in axial view revealed malformed condyle and coronoid process with absence of zygomatic arch on right side. Malformed right auditory meatus was seen with the presence of soft tissue mass [Table/Fig-3]. A 3D reconstruction of CT scan in frontal view revealed facial asymmetry in form of hypoplastic zygomatic complex, midline shift and upward occlusal cant on right side. The right mandibular ramus was displaced medially relative to contralateral side and exhibited rudimentary coronoid process [Table/Fig-4]. In right lateral view, hypoplastic and malformed zygomatic arch, ramus and condylar head was seen with rudimentary coronoid process and absence of glenoid fossa [Table/Fig-5]. Based on these clinico-radiologic features, diagnosis of HFM was confirmed.
Gross facial asymmetry and arrested growth of the right side of the face with macrostomia

Small, malformed right pinna and the presence of preauricular skin tag

Axial view of CT shows hypoplastic condylar head and zygomatic arch, malformed right internal and external ear components with absence of mastoid air cells
3D reconstruction of CT scan (Frontal view) shows midline shift, hypoplastic maxilla and zygomatic bone, and upward occlusal cant towards right side. Medially deviated right mandibular ramus with rudimentary coronoid process was seen
A 3D reconstruction of CT scan (Lateral view) shows hypoplastic zygomatic arch, ramus, condylar head, rudimentary coronoid process and absence of glenoid fossa
HFM is considered as second most common craniofacial malformation after facial clefts with an estimated prevalence of between 1:5600 and 1:26,550 live births [3,4]. The male to female ratio is 3:2 while ratio of right side to left side involvement is 3:2 [2]. HFM is characterised by extreme variability of expression of the disease. The embryonic “developmental field” of first and second branchial arch responds as a single functioning unit in a similar manner to different insults such as vascular disruption, teratogens and chromosome abnormalities which may be responsible for spectrum of anomalies seen in HFM [3]. Minimal diagnostic criteria for HFM include asymmetric hypoplasia of facial structures with preauricular tags or microtia with or without preauricular skin tags. A 30–50% of the patients have auditory problems as a result of malformations in the middle ear [3,4]. The OMENS classification is the most commonly used classification system. The acronym OMENS designates each of the five major areas of involvement: O = orbital, M = mandibular, E = ear, N = facial nerve, and S = soft tissue [5]. Accordingly present case was classified as O0M2E2N0S2. Multidisciplinary treatment approach is required to manage patients with HFM. Decision about need and type of surgical correction depends upon age and growth status of patient and severity of the skeletal deformity and soft tissue deficiency [2].
[1]. Gorlin RJ, Cohen MM, Hennekam RCM, Syndromes of the Head and Neck 2001 4th edOxfordOxford University Press [Google Scholar]
[2]. Wang RR, Andres CJ, Hemifacial microsomia and treatment options for auricular replacement: A review of the literatureJ Prosthet Dent 1999 82:197-204. [Google Scholar]
[3]. Heike CL, Luquetti DV, Hing AV, Craniofacial Microsomia Overview. 2009 Mar 19 [Updated 2014 Oct 9]. In: Pagon RA, Adam MP, Ardinger HH, et al., editorsGene Reviews® [Internet]Seattle (WA)University of Washington, Seattle:1993-2015. [Google Scholar]
[4]. Mielnik-Błaszczak M, Olszewska M, Hemifacial Microsomia – Review of the LiteratureDent Med Probl 2011 48:80-85. [Google Scholar]
[5]. Vento AR, LaBrie RA, Mulliken JB, The O.M.E.N.S. classification of hemifacial microsomiaCleft Palate Craniofac J 1991 28:68-76. [Google Scholar]