Meningiomas are primary central nervous system (CNS) tumours attached to the duramater that arise from the meningothelial cells of the arachnoid. They constitute 30% of primary intracranial tumours [1]. They are generally slow growing benign tumours with predilection for women [2]. Meningiomas are classified into three grades according to World Health Organization (WHO) 2007 criteria [2]. This grading is particularly helpful to identify subtypes of otherwise benign meningiomas with potentially aggressive behaviour. For instance, certain histological subtypes like meningothelial, fibroblastic, transitional and psammomatous meningiomas are sometimes associated with an aggressive behaviour [3]. The grading has important implications for patient management and has been shown to correlate with prognosis. Grade I tumours are treated with surgery alone whereas Grade II and III are treated with surgery, radiotherapy and chemotherapy [4,5].
Hydroxyurea have been used for treatment of recurrent high grade non-resectable meningiomas, but with no complete response [6].
Proliferation markers include p53, Ki-67 (MIB-I), argyrophilic nucleolar organizer regions (AgNOR), 5-bromo-2′-deoxyuridine (BrdU) and proliferating cell nuclear-antigen (PCNA) [7]. Among these proliferation markers Ki67 labeling index is more valuable as it is expressed in all active phases of cell cycle (G1, S, G2 & M) except Go phase [8].
Mutation of TP53 gene, that regulates cell cycle progression, DNA repair and apoptosis, interacts with p53 and acts as a tumour suppressor gene. Meningiomas of grade II and grade III with 1p/14q co-deletion express p53 immunoreactivity [9].
Hence, we undertook this study to correlate the histologic subtype and determine the usefulness of proliferative markers (p53, Ki-67) in the grading of intracranial meningiomas, so as to objectively predict the biological behaviour.
Materials and Methods
This was a prospective and retrospective study of patients with primary intracranial and intraspinal meningiomas operated at our institute, diagnosed at the Department of Pathology during the period January 1995–October 2011. The study was approved by the institutional ethics committee (IEC No.132). The details of the each patient were taken from medical records i.e. age, gender, clinical presentation, radiological evaluation, location, brain infiltration and recurrence were noted. The histological sections were reviewed and all tumours were graded according to WHO 2007 criteria.
For all prospective cases, the specimens received following surgery were fixed in 10 percent buffered neutral formalin for 24 hours. If the resected tissue was received as fragmented bits, all the tissues were submitted for processing. If the tumour was removed in toto and exceeded 6-8cms, representative sections were taken. These tissue blocks were processed and embedded in paraffin wax. The paraffin embedded blocks were cut into 4-5 micron sections and stained with routine Haematoxylin and Eosin stain (H&E). Subtyping and grading was done according to WHO (2007) grading system [Table/Fig-1]. Immunohistochemical (IHC) staining was performed on all prospective and recent retrospective cases for proliferative markers p53 and Ki-67 on 3μm thick, formalin fixed, paraffin embedded tissue sections mounted on 3-3AminoPropylTriethoxySilane (APES) pre-coated slides by Polymer-Horse radish Peroxidase (HRP) Method which uses a non-biotin polymeric technology wherein the secondary antibody conjugated to Poly-HRP reagent is bound to the primary antibody and is visualized by the diaminobenzidine (DAB) chromogen. Heat induced antigen retrieval using pressure cooker – 3 whistles in TRIS EDTA pH 9.0 was applied.
WHO 2007 [2] Histomorphologic criteria for grading of meningioma.
| WHO grade | Criteria |
|---|
| I | Mitosis <4/10 high power field (HPF) |
| II | a) Mitosis 4 - 19/10 HPForb) 3 or more of the following five features: |
| 1. Increased cellularity |
| 2. Uninterrupted patternless or sheet-like growth |
| 3. Small cells with a high nuclear/cytoplasmic ratio |
| 4. Prominent nucleoli |
| 5. Foci of ‘spontaneous’ or ‘geographic’ necrosis |
| III | a) Mitosis ≥20/10 HPForb) Exhibiting loss of differentiated features resulting in carcinoma, melanoma or sarcoma like appearances. |
For retrospective cases, stored slides were taken out and reviewed for subtyping and grading. Wherever necessary blocks were cut and fresh slides prepared. One of the representative blocks were selected for IHC staining.
For Ki-67 and p53, cells with brown nuclear staining were considered positive. Ki-67 labelling index (Ki-67 LI) was recorded as percentage of positively stained tumour nuclei per 1000 tumour cells. The cell counts were performed in regions of maximum immunoreactivity under high power objective [10].
Section of invasive ductal carcinoma of breast was used as positive control for p53. Sections of tonsil and lymph node were used as positive control for Ki-67.
Statistical Analysis
The statistical analysis done in this study was proportion test for p53 using STATA 13.1; Mann Whitney-U test and Kruskall-Wallis test for Ki-67 LI. The p-value of <0.05 is considered to be statistically significant.
Results
Among the total 224 meningioma cases, which included 43 prospective cases and 181 retrospective cases, the mean age was 48.9 years (range: 5 to 85 years) and the common age group for all grades of meningioma was 5th - 6th decade and declining thereafter. There were 78 males and 146 females. In all cases of meningiomas including aggressive variants there was a female predominance (F:M=1.9:1). Most common intracranial location was cerebral convexity followed by parasagittal region [Table/Fig-2]. Most spinal meningiomas occured in the thoracic region. Based on WHO 2007 grading criteria, Grade I meningiomas [Table/Fig-3] were most common (86.6%) followed by grade II (10.7%) and grade III (2.7%) [Table/Fig-4]. Meningothelial (26.3%) meningioma was the commonest subtype followed by psammomatous (25.4%), transitional (19.2%), fibroblastic (14.3%), angiomatous (5.8%), metaplastic (2.7%) and others. Grade II meningiomas included atypical (3 cases), clear cell (3 cases), meningothelial (9 cases), psammomatous (5 cases), transitional (2 cases), fibroblastic(1 case) and angiomatous (1 case) whereas grade III included all the cases of papillary (5 cases) and anaplastic (1case) meningiomas. A total of 18 cases (8%) showed evidence of brain invasion on histology [Table/Fig-4]. Five cases each of meningothelial and papillary meningiomas had brain invasion. A total of 7 (3.1%) cases recurred during 17 years period with slight male predominance (M:F=1:0.75). Recurrence was most common with psammomatous subtype (3/7=42.8%) followed by angiomatous meningioma (2/7=28.6%) while transitional and papillary meningioma constituted one case each. Most of the cases recurred were histologically grade I (n=4) followed by grade II (n=2) and grade III (n=1).
Base line characteristics of subjects according to grade and brain invasion.
| Variables | Total(n = 224) (%) | Grade | Brain invasion |
|---|
| I(n = 193)(%) | II(n = 24)(%) | III(n = 7)(%) | Total(n = 18)(%) |
|---|
| Age in mean(range in yrs) | 48.9 (5-71) | 45.0(5-75) | 44.2 (12-68) | 50.6 (10-71) | 68.2 (10-75) |
| Sex |
| Female | 146 (65.18) | 126 (65.28) | 15(62.5) | 5(71.43) | 14(77.77) |
| Male | 78 (34.82) | 67(34.72) | 9(37.5) | 2(28.57) | 4(22.22) |
| Location |
| Convex/cerebral | 94 (41.96) | 74(38.14) | 16(66.67) | 4(66.67) | 12(66.66) |
| Spinal | 40 (17.86) | 39(20.1) | 1(4.17) | 0(0) | 0(0) |
| Parasagittal | 23 (10.27) | 21(10.82) | 2(8.33) | 0(0) | 0(0) |
| Sphenoid | 10 (4.46) | 9(4.64) | 0(0) | 1(16.67) | 1(5.55) |
| Falx/falcine | 9 (4.02) | 8(4.12) | 1(4.17) | 0(0) | 1(5.55) |
| Tentorial | 7 (3.13) | 6(3.09) | 0(0) | 1(16.67) | 1(5.55) |
| Miscellaneous | 41 (18.30) | 37(19.17) | 4(16.67) | 0(0) | 3(16.66) |
| Subtype |
| MM | 53(23.66) | 44(22.79) | 9(37.5) | 0(0) | 5(27.77) |
| TM | 40(17.85) | 38(19.68) | 2(8.33) | 0(0) | 2(11.11) |
| PsM | 32(14.28) | 27(13.98) | 5(20.83) | 0(0) | 3(16.66) |
| FM | 28(12.5) | 27(13.98) | 1(4.16) | 0(0) | 0(0) |
| AM | 11(4.91) | 10(5.18) | 1(4.16) | 0(0) | 0(0) |
| MeM | 6(2.67) | 6(3.10) | 0(0) | 0(0) | 0(0) |
| SM | 1(0.44) | 1(0.51) | 0(0) | 0(0) | 0(0) |
| ATY M | 3(1.33) | 0(0) | 3(12.5) | 0(0) | 2(11.11) |
| CLM | 3(1.33) | 0(0) | 3(12.5) | 0(0) | 1(5.55) |
| ANA M | 1 (0.52) | 0(0) | 0(0) | 1(16.66) | 1(5.55) |
| PA M | 5(2.23) | 0(0) | 0(0) | 5(83.33) | 4(22.22) |
CP - Cerebellopontine; MM - Meningothelial meningioma; TM - Transitional meningioma; PsM – Psammomatous meningioma; FM – Fibroblastic meningioma; AM – Angiomatous meningioma; MeM - Metaplastic meningioma; SM - Secretary meningioma; ATY M - Atypical meningioma; CLM - Clear cell meningioma; ANA M - Anaplastic meningioma; PA M - Papillary meningioma.
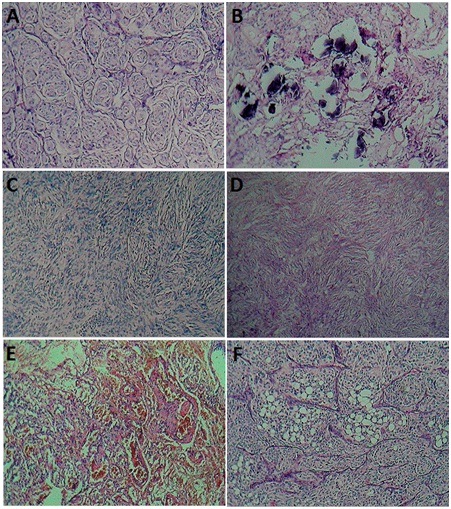
Photomicrograph showing grade I meningiomas: (a)Meningothelial; (b)psammomatous; (c)transitional; (d)fibroblastic; (e)angiomatous; and (f)metaplastic meningioma (H&E, x100).
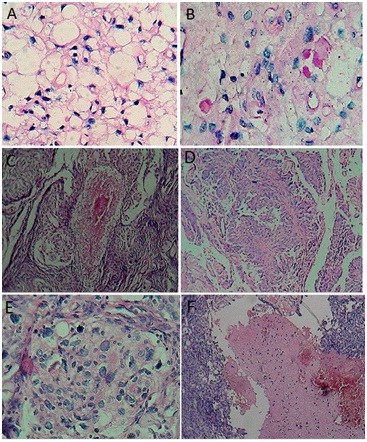
Photomicrograph showing grade II, grade III and brain invasive meningiomas: (a) Clear cell meningioma (H&E, x400)
With; (b)Periodic acid Schiff(PASx400); (c) atypical meningioma (H&Ex100); (d) papillary meningioma (H&Ex100); (e) anaplastic meningioma (H&Ex400); and (f) meningioma with brain invasion (H&Ex100).
Among the 100 patients studied by immunohistochemistry, 80 cases were grade I, 18 were grade II and 2 cases were grade III meningiomas. All the cases of anaplastic, papillary and atypical meningiomas showed p53 positivity. Majority of the cases with p53 positivity were grade III (100%) [Table/Fig-5] followed by grade II meningiomas (83.3%). [Table/Fig-6] shows the distribution of grade and subtype with p53. Proportion test was used to test the difference between the proportions of p53 in grade and subtypes. Borderline significant association was found in the subtype transitional meningioma and p53. Statistical significant association was not found in any other variables at 5% level of significance.
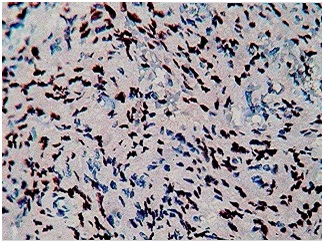
Photomicrograph showing immunohistochemical staining for p53 in grade III meningioma (IHCx400).
Correlation of grade and subtype with p53.
| Variables | p53 | p-value |
|---|
| Positive | Negative |
|---|
| Grade |
| I | 57(77.03) | 23(88.46) | 0.209 |
| II | 15(20.27) | 3(11.54) | 0.319 |
| III | 2(2.7) | 0(0) | 0.397 |
| Subtypes |
| A | 1(1.35) | 0(0) | 0.551 |
| Ang | 4(5.41) | 3(11.54) | 0.292 |
| Aty | 2(2.7) | 0(0) | 0.397 |
| Cl | 2(2.7) | 1(3.85) | 0.769 |
| Fb | 12(16.22) | 5(19.23) | 0.725 |
| Men | 16(21.62) | 5(19.23) | 0.797 |
| Met | 3(4.05) | 0(0) | 0.297 |
| Pap | 1(1.35) | 0(0) | 0.551 |
| Psa | 18(24.32) | 10(38.46) | 0.167 |
| Se | 0(0) | 1(3.85) | 0.090 |
| T | 15(20.27) | 1(3.85) | 0.049 |
Ki-67 Labelling index (Ki-67 LI): Ki-67 was positive in all the cases of anaplastic, papillary, atypical and metaplastic meningiomas. Ki-67 was mostly positive in grade III (100%) followed by grade II meningiomas (77.7%) [Table/Fig-7].
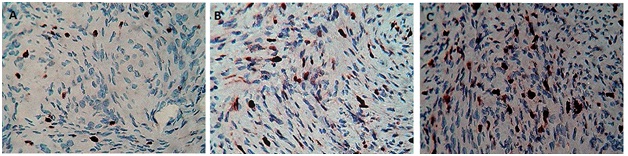
Photomicrograph showing immunohistochemical staining for various grades of meningioma: Ki-67 labelling index in (a) grade I; (b) grade II; (c) grade III meningioma (IHCx400).
Most of the benign meningioma (grade I) expressed low Ki-67 LI, in contrast to grade III meningioma, which had a high Ki-67 LI. Meningiomas were distributed according to the grade at arbitrary cut-off levels of Ki-67 LI [Table/Fig-8]. Most of the grade I meningiomas have Ki-67 LI ≤7 in contrast to grade II and grade III meningiomas that have LI ≥7. Ki-67 LI for grade I, grade II and grade III meningiomas were 3.1%, 7% and 14.2% respectively. The anaplastic meningioma showed Ki-67 LI of 15.6%. Ki-67 LI in meningioma with brain invasion, irrespective of histology was 9.6 % and in non- brain invasive meningioma was 3.3%.
Distribution of tumours according to grade at arbitrary cut-offs of Ki-67 LI [9].
| Ki-67 LI | Grade I | Grade II | Grade III |
|---|
| 0-4 % | 46 | 5 | 0 |
| 4.1-7 % | 30 | 3 | 0 |
| 7.1-11% | 4 | 5 | 0 |
| >11 % | 0 | 5 | 2 |
| Total | 80 | 18 | 2 |
[Table/Fig-9] shows correlation of Ki-67 LI with grade, subtype and brain invasion. Grade III has been excluded in the analysis, since only 2 patients were in the group. Values of KI-67 LI were statistically different in grade I and grade II. Ki-67 LI values were statistically significant in brain invasion. Statistical significant difference of ki-67 LI between the subtypes was not found.
Correlation of grade, brain invasion and subtype with Ki-67 LI.
| Variables | Ki67 LIMedian (IQR)c | p-valuea |
|---|
| Grade | | <0.001 |
| I | 3.5 (0,6) |
| II | 9 (5, 14) |
| Brain invasion | | <0.001 |
| Yes | 10 (8,15) |
| No | 4 (0,6) |
| Subtypes | | 0.197b |
| Fb | 4 (0,5) |
| Men | 6 (1,8) |
| Psa | 2.5 (0,5) |
| T | 3 (1.5,5.5) |
| Others | 6 (0,10) |
aMann Whitney-U test and b Kruskall-Wallis test were used to compare between the groups and ki67 cInter-quartlie range
Discussion
The biological nature of meningiomas cannot be predicted based on histomorphological appearances alone [3]. In the study by Perry A et al., [11], tumour recurrence rates were 7-20% of benign (Grade I), 29-40% of atypical (Grade II), 50-78% of anaplastic (Grade III) meningiomas. In contrast, all the seven recurrent cases in our study were initially operated in outside hospitals and comprised six cases of grade I and one case of grade III meningioma. The probable reason could be incomplete removal of the primary tumour. Two cases (28.5%) of recurrent meningiomas showed brain invasion, one each of grade I and grade III.
In our study p53 was mostly positive in grade III meningiomas (100%) followed by grade II meningiomas (83.3%).
Kumar et al., observed p53 immunopositivity of 0%, 19% and 23.1% in grade I, grade II and grade III meningiomas respectively [9]. Twenty percent of grade II and 25% of grade III meningiomas with co-deletion of 1p/14q showed p53 immunopositivity. This study also stated that p53 mutation have no role in the pathogenesis of meningiomas.
In the study by H Cho et al., p53 immunoreactivity demonstrated in grade I, grade II and grade III meningiomas were 9.5%, 72.7% and 88.9% [12]. This showed that immunoreactivity of p53 was significantly higher as histological grade increased. p53 immunoreactivity was expressed in 71.4% of recurrent meningiomas but only in 10.5% of nonrecurrent meningiomas in their study, indicating its high immunoreactivity in recurrent meningiomas. p53 gene mutation was observed in 62.5% of grade II, 25% of grade III meningiomas and none of the grade I meningiomas.
H Cho et al., pointed out that p53 immunopositivity and TP53 gene mutation were associated with prognosis of meningiomas and serve as markers of progression of meningiomas [12].
Wahda et al., reported th at the mean Ki-67LI was 10.6±6.4 in three anaplastic meningiomas and that of atypical & benign meningiomas were 5.4±2.8 and 1.8±3.5 respectively [13]. Kolles et al., reported that Ki-67 (MIB-1) LI is the most important criterion for distinguishing anaplastic meningiomas (WHO grade III) (mean Ki-67 LI: 11%) from those of common type (WHO grade I) (mean Ki-67 LI: 0.7%) [14]. The atypical meningiomas (WHO grade II) are characterized by a mean Ki-67 LI of 2.1%. Akyildiz et al., found a significant statistical relationship between Ki-67 LI and mitotic activity, necrosis, pattern loss, small cell change and brain invasion [15]. No relationship was found between Ki-67 PI and dura or bone invasion. Recently Roser et al., reported a large retrospective study of 600 resected meningiomas in which histological grading revealed 91% WHO grade I meningioma (mean MIB-1 LI: 3.88%), 7% grade II meningioma (mean MIB-1 LI: 9.95%) and 2% grade III meningioma (mean MIB-1 LI: 12.18%) [16]. In their study, immunohistochemistry was performed in 580 cases and Ki-67 LI increased in recurrent meningiomas when compared to primary initial meningiomas with significant correlation between high tumour vascularity, high Ki-67 LI and negative progesteron receptor status.
In our study, mean Ki-67 LI in grade I, grade II and grade III meningiomas were 3.1%, 7 % & 14.2% respectively. Mean Ki-67 LI in brain invasive meningiomas was 9.56 % and in non-brain invasive meningiomas was 3.88 %. Ki-67 LI between grade I and grade II, and brain invasive and non-invasive meningiomas was statistically significant similar to the observations by Babu et al., [17].
Some authors have found a higher mean MIB-1 LI in meningioma that ultimately recurred, while others have obtained different result. In our study, Ki-67 LI and p53 expression correlated with grade of meningioma from grade I to grade III displaying their aggressive nature similar to the observations by Amatya et al., & Devaprasath A et al., [10,18].
In the study, there were an increasing mean Ki-67 LI with increase in grades of meningiomas. Amatya et al., reported that p53, as an apoptosis-related protein, is likely to be imported in not tumourigenesis but malignant progression or recurrence [18]. S-Y Yang et al., reported that p53 overexpression was an independent prognostic factor associated with malignant progression, tumour recurrence, increased proliferation marker Ki-67 and a positive correlation with the histologic grades of meningiomas [19]. Grade I tumours are treated with surgery alone whereas Grade II and III are treated with surgery, radiotherapy and chemotherapy.
Chamberlain MC et al., studied utilisation of Hydroxyurea in meningioma and concluded that Hydroxyurea could not cause complete or partial response in any case of meningioma and 43% revealed stable disease in his study [6]. Benign meningiomas have very good prognosis with approximately 100% 5 year survival. Malignant meningiomas have poor prognosis with median survival of 1 to 3 years even with recommended management.
Limitations
Immunohistochemistry was performed in only 100 cases because of cost effectiveness. Probably a larger study may be taken up in the future.
Immunohistochemistry could not be done on recurrent tumours, where initial surgery was done in outside hospitals and blocks were not available, which would have provided us valuable information on proliferative status of recurrent tumours, especially those of grade I meningioma cases.
Another limitation is poor follow up of the patients. As most of the patients were from poor socioeconomic status, so usually they don’t report for follow up visits unless they have some major problem like recurrence.
Conclusion
Majority of the patients in our study were in 5th-6th decade with mean age of 48.9 years (range: 5-85 years) and showed female preponderance irrespective of grade. The biological behaviour and aggressiveness of meningioma correlate well with the WHO 2007 grading system. Anaplastic, papillary, clear cell & atypical subtypes of meningioma are usually of higher grade. p53 and Ki-67 markers correlate well with the proliferative activity of meningioma & show high positivity in aggressive high grade cases. Ki-67 LI is the most important criterion for distinguishing anaplastic meningioma from those of benign meningioma. Brain invasive meningioma has high Ki-67 LI than non-invasive meningioma.
CP - Cerebellopontine; MM - Meningothelial meningioma; TM - Transitional meningioma; PsM – Psammomatous meningioma; FM – Fibroblastic meningioma; AM – Angiomatous meningioma; MeM - Metaplastic meningioma; SM - Secretary meningioma; ATY M - Atypical meningioma; CLM - Clear cell meningioma; ANA M - Anaplastic meningioma; PA M - Papillary meningioma.
aMann Whitney-U test and b Kruskall-Wallis test were used to compare between the groups and ki67 cInter-quartlie range