Mystery of Sciatica Resolved - A Rare Case Report
Jayanth Kumar Bangalore Chikkanna1, Surendra Gopal2, Deepak Sampath3
1 Senior Consultant and Unit Chief, Department of Orthopaedics, St Martha’s Hospital, Bengaluru, Karnataka, India.
2 Resident, Deparment of Orthopaedics, St Martha’s Hospital, Bengaluru, Karnataka, India.
3 Consultant, Department of Orthopaedics, St Martha’s Hospital, Bengaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jayanth Kumar No 26, 2 Cross, C R Layout Sarakki Main Road, 1st Phase J.P Nagar, Bangalore-560078, Karnataka, India. E-mail : jkbcortho@gmail.com
Schwannomas are common, benign, slow growing tumours of peripheral nerve sheath arising from the schwann cells of the neuroectoderm. They do not transverse the nerve but remain within the sheath on top of the nerve. They rarely present in the sciatic nerve. Sciatic schwannomas may mimic symptoms of herniated disc, usually with radiation of pain to buttocks and thigh region with inability to walk for long distances and sometimes may present with claudication. In the absence of low back pain and with a normal Lumbo-Sacral MRI study, causes intrinsic to sciatic nerve needs to be thought off, which often delays the diagnosis. Rarity in our case-patient presented with tingling sensation and inability to squat on hard surface for more than 10 minutes with a normal x-ray and MRI study of lumbosacral spine.
Schwannomas, Sciatic neuroma
Case Report
A 40-year-old obese male presented to us with persistent left thigh pain, difficulty in squatting on hard surfaces and an h/o tingling sensation and radiating pain in the left lower limb. History for tinnitus, hearing loss, vestibular problems and family h/o neurofibromatosis were negative. He had consulted more than five orthopaedic and neurosurgeons for the same issue. Since the radiological investigations were normal, he had been then subjected to nerve root blocks in lumbar region at L3, L4 and L5 on left side, exercises and local infiltration which were not at all fruitful. Since patient found no relief with the usual recommended remedies for sciatica and was consistent in complaining when he presented to us he was examined in detail for other causes.
On examination- Patient was found to be obese with unremarkable gait. No Motor or sensory deficits. Higher Mental Function and Deep Tendon Reflex of the lower limbs were normal. Upper Motor Neuron lesion signs and Lasegue’s test were negative. No exacerbation of the symptoms with spine movements or coughing. Both the Hip joints were clinically normal. No Café au lait spots were found and slit lamp examination was negative for any lisch nodules. Tinel’s sign was negative. On deep palpation of gluteal region, at the junction of left gluteus and upper third of the thigh a small discrete mass was palpable, which on pressure patient complained of a similar sensation which he was experiencing all these days. This encouraged us to get MRI study of the gluteal and upper thigh region done.
MRI report showed schwannoma of the left sciatic nerve, single large swelling of the left sciatic nerve in the upper part of the thigh with no muscle involvement and to consider benign lesion [Table/Fig-1].
MRI images of swelling in upper thigh.

Surgical technique
Extensive literature search was done, common tumour in sciatic nerve was schwannomas which could be excised without residual nerve damage, and we decided to excise the swelling.
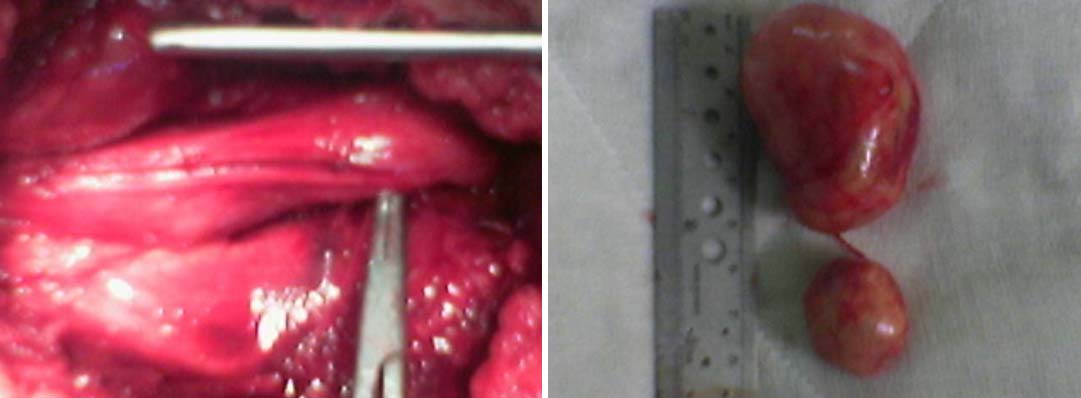
After pre-op investigations, patient was operated in semi-prone position with left side up under spinal anaesthesia through posterior Moore’s approach. As the muscles were divided we found a large clearly encapsulated mass measuring 4x5 cm arising from the sciatic nerve. The nerve was exposed clearly both proximally and distally and was removed en bloc leaving the sciatic nerve intact. But to our surprise another small swelling measuring 1x1 cm separate from the big swelling was noted, which was also enucleated from sciatic nerve [Table/Fig-2] and sent for histopathological examination. Wound was closed over a suction drain, with no postoperative morbidity.
Intraoperative pictures showing two swellings arising from sciatic nerve.

Intraoperative pic showing lax nerve after resection and excised specimens.
The histopathological examination of the swellings confirmed the diagnosis of schwanomma. Postoperatively, he was symptom-free and there were no neurological deficits [Table/Fig-3]. Patient has been followed-up for a period of one year now with no recurrence of old or appearance of new symptoms, no trophic disturbances and has been symptom- free since the time of surgery.
Follow-up X- ray showing unaffected sciatic function in the form of active dorsi flexion of ankle.

Discussion
Specific clinical examination along the course of sciatic nerve, to find sciatic nerve causes in constant symptoms, with normal radiological investigations of lumbosacral spine, clinched us the aetiology for patient’s symptoms.
Schawannoma of the sciatic nerve is rare arising from the sheath of peripheral nerve contributes to around 1%. Schwannomas, generally affect the main trunk of the sciatic nerve [1]. They are generally solitary in nature and occurrence of multiple schwannomas is rare. Malignant transformation of benign is unusual, approximately 5%. Sciatic nerve schwannomas can be purely intrapelvic, purely extrapelvic or intraextrapelvic dumbbell-shaped masses [2]. They have a long sub-clinical course and their clinical presentation is usually misleading. Patients with long standing symptoms of radicular pain not responding to physical therapy, rest, anti inflammatory drugs with negative Lasegue test should raise the suspicion of non-discogenic cause of sciatica like other sciatic nerve pathologies. EMG and Ultrasound may also be useful in establishing the diagnosis. Schwannoma of the sciatic nerve is rarely diagnosed as the cause of sciatica [3–6].
Schwannomas most commonly occur in adults between 20 and 50 years without gender distinction, generally appear as solitary and not necessarily correlated with neurofibromatosis, which has precise chromosomal alterations. Motor and sensory deficits are more common with tumours larger than 4cm.
Main lesion to be considered in the differential diagnosis is neurofibromas. Preoperatively schwannomas can be differentiated from neurofibromas with the characteristic MRI features as neurofibromas appear more heterogenous on T1 and T2-weighted MR images however definitive diagnosis is possible with histological examination. Solitary schwannomas are well circumscribed, encapsulated, eccentric tumours arising from the proximal nerve roots. Schwannomas arise from a single fascicle and grow circumferentially displacing other fascicles in nerve sheath. They are densely packed spindle cells Antoni type A or the loosely textured stroma as in Antoni type B is the characteristics of histopathological examination. Multiple schwannomas can be seen in neurofibromatosis type 2 [6].
Neurofibromas on the other hand are multiple, lack a tumour capsule, originate from distal nerves, fusiform swellings of nerves are common, arise from perineural fibrocytes and mainly from motor parts of a mixed nerve with fascicles intimately involved. Surgical resection of neurofibromas usually results in neurological deficits while resection of schwannomas which arise within the nerve sheath and have a true capsule result in no residual deficit.
Other differential diagnoses to be considered are neurofibrolipoma, intranervous lipoma and haemangioma of sheath. Sciatic nerve can entrap along its course within in the pelvis or the lower limb due to compartment syndrome, heterotrophic ossification, myofascial bands in the thigh, misplaced intramuscular injection, post traumatic or anticoagulant induced haematomas and bone and soft tissues tumours can cause sciatica [7].
Conclusion
In refractory case of radicular pain, with persistent symptoms and negative radiological investigations to suggest spinal pathology as a cause ENMG, ultrasound scanning along the sciatic nerve course or MRI imaging of part suspicious of pathology may be useful to detect sciatic schwannomas. Preserving the integrity of the nerve together with the fascicles which are not infiltrated by the tumour assures favourable outcome without additional neurological deficits.
Conflict of Interest
No benefits in any form have been received or will be received from commercial party related directly or indirectly to the subject of this article.
[1]. Rhanim A, El Zanati R, Mahfoud M, Berrada MS, El Yaacoubi M, A rare cause of chronic sciatic pain: Schwannoma of the sciatic nerveJ Clin Orthop Trauma 2013 4(2):89-92. [Google Scholar]
[2]. Spinner RJ, Endo T, Amrami KK, Dozois EJ, Babovic-Vuksanovic D, Sim FH, Resection of benign sciatic notch dumbbell-shaped tumoursJ Neurosurg 2006 105(6):873-80. [Google Scholar]
[3]. Pilavaki M, Chourmouzi D, Kiziridou A, Skordalaki A, Zarampoukas T, Drevelengas A, Imaging of peripheral nerve sheath tumours with patholiic correlation: Pictorial reviewEur J Radiol 2004 52:229-39. [Google Scholar]
[4]. Sawada T, Sano M, Ogihara H, Omura T, Miura K, Nagano A, The relationship between pre-operative symptoms, operative findings and postoperative complications in schwannomasJ Hand Surg Br 2006 31:629-34. [Google Scholar]
[5]. Hamdi MF, Aloui I, Ennouri KH, Sciatica secondary to sciatic nerve schwannomaNeurol India 2009 57:685-86. [Google Scholar]
[6]. Kralick F, Koenigsberg R, Sciatica in a patient with unusual peripheral nerve sheath tumoursSurg Neurol 2006 66:634-37. [Google Scholar]
[7]. Haspolat Y, Ozkan FU, Turkmen I, Kemah B, Turhan Y, Sarar S, Ozkan K, Sciatica due to Schwannoma at the Sciatic NotchCase Rep Orthop 2013 10(1155) [Google Scholar]