Molar Pregnancy Presents as Tubal Ectopic Pregnancy: A Rare Case Report
Devi Beena1, S Teerthanath2, Varsha Jose3, Jayaprakash Shetty4
1 Post Graduate, Department of Pathology, K S Hegde Medical Academy, Nitte University, Deralakattae, Mangalore, India.
2 Professor, Department of Pathology, K S Hegde Medical Academy, Nitte University, Deralakattae, Mangalore, India.
3 Post Graduate, Department of Pathology, K S Hegde Medical Academy, Nitte University, Deralakattae, Mangalore, India.
4 Professor and Head of Department, Department of Pathology, K S Hegde Medical Academy, Nitte University, Deralakattae, Mangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Devi Beena, Post Graduate, Department of Pathology, K S Hegde Medical Academy, Nitte University, Deralakattae, Mangalore-575018, India.
E-mail: devibeena1987@gmail.com
The incidence of hydatidiform mole is 1 per 1000 pregnancies. The occurrence of hydatidiform mole in ruptured tubal pregnancy is very rare. We report an unusual case of molar pregnancy in the right fallopian tube which presented as an adherent adnexal mass. The present case conveys the importance of histological examination of products of conception which helps the pathologist to provide an appropriate diagnosis, thereby the clinician can offer appropriate counseling and follow up to the patient.
Fallopian tube, Gestational trophoblastic disease, Hydatidiform mole
Case Report
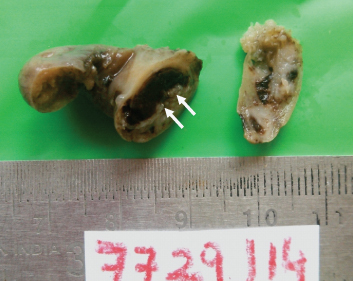
A 32-year-old female with obstetric score of G3P2L2 came to obstetric outpatient department with complaints of amenorrhea since one and half months, pain abdomen and spotting per vaginum since one day. There were no complaints of vomiting or febrile illness. Past obstetric history was normal. Urine pregnancy test was done and was positive. Clinical examination revealed soft abdomen with mild tenderness in the hypogastrium and right iliac fossa. Per vaginal examination revealed bulky uterus and right cervical tenderness was positive. There was no evidence of mass lesion. Ultrasonography of the pelvis showed right adnexal mass 4x3cm adjacent to right ovary and uterus height was corresponding to 5weeks 1 day. Haemoperitoneum with minimal fluid was noted in Morison’s pouch. Routine haematological and biochemical examinations were within normal limits. Explorative laprotomy was performed. Intraoperatively, there was ruptured right tubal mass measuring 3x2 cm with moderate haemoperitoneum. Right salphingectomy was done. The specimen was sent for histopathological evaluation. The right fallopian tube measured 4cm in length and was dilated and ruptured near fimbrial end. Two tiny parafimbrial cyst seen each measuring <0.5 cm. Cut surface along the dilated segment of the fallopian tube showed thinned out wall and the lumen contained blood clot with pale glistening tiny cyst (m) <0.5 cm [Table/Fig-1].
Cut surface of the fallopian tube showing dilated lumen containing small tiny glistening cyst (arrow)
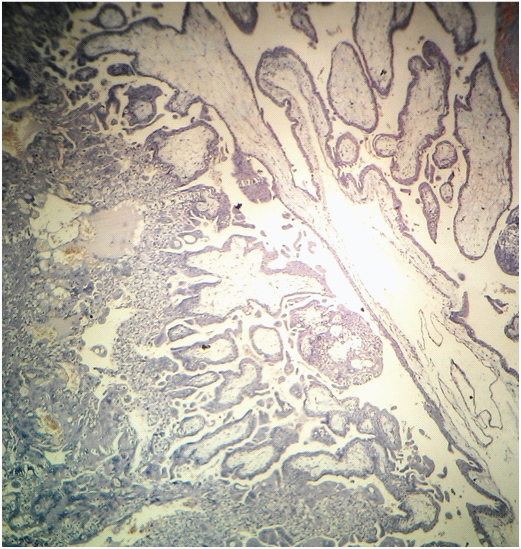
Histological examination revealed ruptured fallopian tube. The lumen contained blood clot with branching, avascular villi with marked edematous stroma. Proliferation of cytotrophoblast and syncitiotrophoblast was seen with moderate degree of atypia. The villous structures were seen penetrating the muscularis layer of fallopian tube along with haemorrhage [Table/Fig-2].
Microscopy showing branching avascular villi and proliferated trophoblast showing nuclear atypia
The patient was followed weekly quantitative beta HCG titers until three successive beta HCG levels were negative (HCG<5mI u/ml). The Beta HCG values were 134 mIU/ml, 4.19 mIU/ml and 2.68 mIU/ml consecutively.
Discussion
Ectopic gestation is a common phenomenon with an incidence rate of 4.5- 16.8/1000 pregnancies. Tubal ectopic hydatidiform moles are quiet rare lesions, and 132 cases have been reported in the world literature [1]. GTD can be preceded by any type of pregnancy, including a term pregnancy, abortion, molar gestation, or rarely by tubal gestation. The median maternal age is 31 (range, 15-54) years and median gestational age is10 (range, 5-27) weeks [2]. Hydatidiform moles occurs due to a placental malformation; due to genetic aberration of the villous trophoblast. This is characterized by cystic swelling and trophoblastic proliferation. Molar gestation commonly develops within the uterus but may also occur in sites of ectopic pregnancy [3].
Burton et al., studied the incidence of tubal ectopic hydatidiform moles for a period of ten years and concluded that this is a rare entity and is usually over diagnosed [4].
Hydatidiform moles arise due to abnormal fertilization. The chromosomal pattern in a complete mole is 46, XX with paternal genome origin. This is due to the fertilization of an empty ovum by a haploid spermatozoon, which later divides. Partial moles usually arise from dispermic fertilization of a haploid ovum, resulting in a triploid genome [5]. Clinically patients with hydatidiform mole complain of abdominal pain; some have vaginal bleeding. Ultrasonography in hydatidiform mole, a placental site trophoblastic tumour, and choriocarcinoma will be like heterogeneous, hypo-echoic, solid mass with cystic vascular spaces. In comparison with partial moles, complete mole is easily detectable. Hence, histopathological examination of products of conception remains the current gold standard for identification [6]. Pathologists face a difficult challenge on histologically discriminating partial mole, complete mole and hydropic abortion. Molar pregnancies should only be diagnosed when there is circumferential proliferation of trophoblast, hydrops, scalloped villi, and stromal karyohexis. Flow-cytometric DNA analysis may also be performed [7].
Sebire et al., also state that compared with evacuated uterine products of conception the pathologist must keep in mind that the degree of extra villous trophoblastic proliferation may appear more florid in ectopic gestation [8]. Histological examination of the tubes is mandatory in all ectopic pregnancies [9]. Laproscopy is the main mode of treatment in cases of ectopic pregnancy. Pasic et al., have suggested the surgical treatment for the majority of women should be salpingotomy [10].
Appropriate monitoring of beta-hCG titers of suspected ectopic pregnancy is important. It helps to diagnose persistent ectopic gestation and to rule out the presence of malignant trophoblastic disease [11]. However, one single undetectable HCG level after evacuation is sufficient [3]. In our case the HCG levels progressively decreased and later undetectable during the follow up. There was no evidence of reccurence in our case after 6 months of follow up.
Conclusion
The indexed case shares the relevance of the histological examination of conceptus in ectopic pregnancies for the correct diagnosis and appropriate followup to the patient. It is important that the clinicians consider the possibility of a hydatidiform mole in the extra-uterine cavity in patients with clinical scenario similar to ectopic pregnancy.
[1]. Sebire NJ, Lindsay I, Fisher RA, Savage P, Seckl MJ, Overdiagnosis of complete and partial hydatidiform mole in tubal ectopic pregnanciesInt J Gynecol Pathol 2005 24(3):260-64. [Google Scholar]
[2]. Husain N, Mishra S, Pradeep Y, Ectopic Molar Pregnancy Mimicking ChoriocarcinomaThe Internet Journal of Gynecology and Obstetrics 2008 :12 [Google Scholar]
[3]. Samaila MO, Adesiyun AG, Bifam C, Ruptured tubal hydatidiform moleJ Turkish-German Gynecol Assoc 2009 10:172-74. [Google Scholar]
[4]. Burton JL, Lidbury EA, Gillespif AM, Tidy JA, Smith O, Lawry J, Over-diagnosis of hydatidiform in early tubal ectopic pregnancyHistopathology 2001 38:320-21. [Google Scholar]
[5]. Slimani O, A case of tubal hydatidiform moleOpen Journal of Obstetrics and Gynecology 2013 3:625-27. [Google Scholar]
[6]. Sherer DM, Stimphil R, Hellman M, Transvaginal sonographic findings of isolated intramural uterine choriocarcinoma mimicking an interstitial pregnancyJ ultrasound Med 2006 25:791-94. [Google Scholar]
[7]. Tanha FD, Molar Pregnancy Presents as Tubal Ectopic Pregnancy RoyanInstitute International Journal of Fertility and Sterility 2011 4:184-86. [Google Scholar]
[8]. Sebire NJ, Makrydimas G, Agnantis NJ, Zagorianakou N, Rees H, Fisher RA, Updated diagnostic criteria for partial and complete hydatidiform mole in early pregnancyAnti-cancer Res 2003 23:1723-28. [Google Scholar]
[9]. Gavez CR, Fernandez VC, Jaén MM, Teruel RG, Primary tubal choriocarcinomaInt Gynecol Cancer 2004 14:1040-04. [Google Scholar]
[10]. Pasic RP, Hammons G, Gardner JS, Hainer M, Laparoscopic treatment of cornual heterotopic pregnancyJ AM Assoc Gynecol Laparosc 2000 9:372-75. [Google Scholar]
[11]. Rotas M, Khulpateea N, Binder D, Gestational choriocarcinoma arising from a cornual ectopic pregnancy: a case report and review of the literatureArch Gynecol Obstet 2007 276:645-47. [Google Scholar]