Giant left Atrial Myxoma Induces Mitral Valve Obstruction and Pulmonary Hypertension
Deva Japa1, Mahpaekar Mashhadi2, Sanjeeth Peter3
1 Senior Research Scientist, Department of Pathology, DDMM Heart Institute & Senior Research Scientist, GMC Cardiothoracic and Vascular Research Society, Nadiad, Gujarat, India.
2 Senior Research Scientist, Department of Cardiology, DDMM Heart Institute & Senior Research Scientist, GMC Cardiothoracic and Vascular Research Society, Nadiad, Gujarat, India.
3 Senior Research Scientist, Department of Cardiothoracic Surgery, DDMM Heart Institute & Senior Research Scientist, GMC Cardiothoracic and Vascular Research Society, Nadiad, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deva Japa, Senior Research Scientist, Department of Pathology, DDMM Heart Institute, Mission Road, Nadiad, Gujarat, India. E-mail : devajapa@ddmmheart.org
Atrial myxomas are the commonest benign primary tumours of the heart. They are generally 2 to 6 cm in size. Depending on their size and site may result in mitral valve obstruction which may lead to pulmonary hypertension. Clinical symptoms may suggest the presence of a myxoma but echocardiography is the mainstay of diagnosis and confirmation is by histopathology. A well-formed, organized thrombus is a common differential. The report of an unusually large left atrial myxoma that occurred in a 54-year-old male causing mitral valve obstruction and pulmonary hypertension is presented here.
Echocardiography, Myxoma, Primary cardiac tumour, Thrombus
Case Report
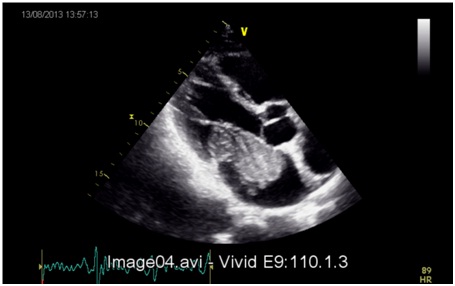
A 54-year-old male presented with complaints of chest pain and intermittent shortness of breath for 1 year, with no familial history of similar complaints. Physical examination revealed blood pressure 130/80 mmHg and heart rate of 94/minute. A ‘tumour plop’ was heard on auscultation of the precordium and routine laboratory investigations were unremarkable. An echocardiography demonstrated a 7.3cm × 3.7cm pedunculated mass in the left atrium that extended into the left ventricle during systole [Table/Fig-1]. Angiography showed normal coronary vessels. The tumour was removed surgically. Recent follow-up showed no evidence of recurrence or thromboembolic complications.
Pathological findings: Gross examination of the specimen showed a partially encapsulated pedunculated polypoidal mass measuring 8.3cm x 4.7cm x 2.7cm and weighing 65 grams. On one side, the mass showed interatrial septal attachment with pedicle [Table/Fig-2]. The mass was greyish yellow to dark brown in colour. Cut section of the mass showed dark brown haemorrhagic areas and gelatinous yellow areas.
Two dimensional echocardiography showing left atrial mass extending into left ventricle
Pedunculated gelatinous mass with interatrial septum

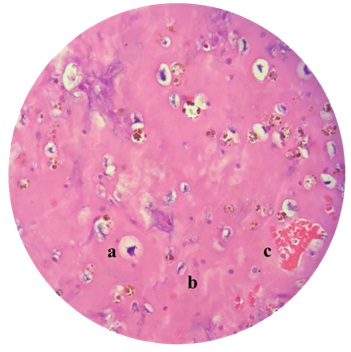
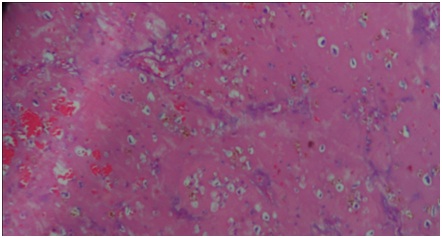
The tumour showed cells which are ovoid to stellate shaped with plump nuclei, open chromatin and indistinct border [Table/Fig-3] in the background of myxoid. The cells were arranged in capillaries, cords, and many were singly placed [Table/Fig-4]. Haemorrhagic areas showed numerous vascular spaces with telangiectasia aspect [Table/Fig-3]. Some areas showed mucoid changes. Stroma showed haemosiderin pigmented macrophages many multinucleated giant cells. No evidence of increase cellularity, plemorphism or mitosis seen. Calretinin is a novel marker to differentiate myxoid cells from mural thrombi. Hence, the positivity of Calretinin established the diagnosis.
Left atrial myxoma showing ovoid cell: (a) stellate cells; and (b) haemorrhagic areas in myxoid stroma (H&E)
Left atrial myxoma (low power- H&E)
Discussion
Primary intracardiac tumour in the site of left ventricle was described in 1559 [1]. Tumours of the heart are rare with varied histological type. Atrial myxomas are the commonest benign primary tumours of the heart and occur in as many as 3 in 1000 patients [1]. Myxomas make up 40-50% of the primary intracardiac tumours [2]. Atrial myxomas are sporadic in origin with unknown aetiology [3]. Most of these lesions, nearly 90%, appears to be solitary and pedunculated with 75-85% seen in left atrial cavity [4]. The symptoms of atrial myxoma is related to location, embolization and propensity to obstruct blood flow through the heart and clinically difficult to diagnose [5,6]. However, the diagnosis was possible only at post-mortem. In 1951, for the first time the diagnosis of left atrial tumour was confirmed by angiocardiography [7]. Now echocardiography is the important diagnostic tool in cases suggestive of intra cardiac tumours which is later confirmed histologically after removal [5,7].
The size of the lesion differs widely among patients but generally ranges from 2 to 6 cm [3]. When the tumour is on the left side of the heart, it can embolize and cause systemic deficits. The tumour may manifest as systemic or constitutional symptoms. There may be no symptoms even if the atrial myxoma develops into a giant mass, hence can be an incidental finding [5,8]. In this case, the tumour of size 7cm presented with breathlessness. Depending on the size and location, it may cause mitral valve obstruction and pulmonary hypertension [7]. The most useful diagnostic tool is the echocardiogram which delineates the site, size and attachment while differentiating from vegetation or a thrombus [9]. While echocardiography is the main diagnostic tool used to detect inrtacardiac masses, discriminating between primary cardiac tumours, such as myxoma, and other cardiac masses is still a challenge. This can only be confirmed by histopathological examination. As literature reveals there is low surgical mortality and good long term results in patients with cardiac myxoma. Our patient made an uneventful recovery and is healthy as revealed by the two year follow up.
Histologically presence of myxoma cells in the background of myxoid stroma is the diagnostic feature. The most challenging differential diagnosis is with mural thrombi showing myxoid changes. According to the reported studies, Immunohistochemistry (IHC) is not particularly helpful in the diagnosis of cardiac myxoma, but Calretinin marker led to the differential diagnosis of myxoma cells from mural myxoid thrombi. Positive expression of Calretinin marker indicates that the myxoma cells may originate from endocardial sensory nerve tissue [10]. In our case few multinucleated cells were seen which were formed by the close apposition and fashion of adjoining cells by means of intermediate junction.
Conclusion
Giant left atrial myxoma is a rare benign lesion of the heart which can be completely cured by surgical removal. Myxomas are usually detected when small. Rarely, it may have an asymptomatic course and present with symptoms only when it becomes a large mass. Such large myxomas frequently have systemic embolization because of which they are detected. In spite of being so large, there were no obvious associated symptoms in our case.
[1]. Centofanti P, Di Rosa E, Deorsola L, Actis Dato G, Patané F, La Torre M, Primary cardiac tumors: early and late results of surgical treatment in 91 patientsThe Annals of Thoracic Surgery 1999 68(4):1236-41. [Google Scholar]
[2]. Bajraktari G, Emini M, Berisha V, Gashi F, Beqiri A, Zahiti B, Giant left atrial myxoma in an elderly patient: Natural history over a 7-year periodJ Clin Ultrasound 2006 34(9):461-63. [Google Scholar]
[3]. Asai Y, Ichimura K, Kaneko M, Abe T, Treatment of life-threatening huge atrial myxoma: Report of two casesSurgery Today 1999 29(8):813-16. [Google Scholar]
[4]. Panagiotou M, Panagopoulos N, Ravazoula P, Kaklamanis L, Koletsis E, Large asymptomatic Left Atrial Myxoma with ossification: case reportJ Cardiothorac Surg 2008 3(1):19 [Google Scholar]
[5]. Rohani A, Akbari V, A colossal atrial myxomaJournal of Cardiovascular Disease Research 2010 1(3):158-60. [Google Scholar]
[6]. Ozeke O, Tufekcioglu O, Selcuk H, Ozdogan O, Sahin O, A giant left atrial myxoma prolapsing to midlevel of the left ventricle causing severe pulmonary hypertensionEuropean Journal of Echocardiography 2005 6(2):144-45. [Google Scholar]
[7]. Rahmanian P, Castillo J, Sanz J, Adams D, Filsoufi F, Cardiac myxoma: preoperative diagnosis using a multimodal imaging approach and surgical outcome in a large contemporary seriesInteractive CardioVascular and Thoracic Surgery 2007 6(4):479-83. [Google Scholar]
[8]. Buyukates M, Aktunc E, Giant left atrial myxoma causing mitral valve obstruction and pulmonary hypertensionCanadian Journal of Surgery 2008 51(4):E97-8. [Google Scholar]
[9]. Swartz M, Lutz C, Chandan V, Landas S, Fink G, Atrial Myxomas: Pathologic Types, Tumor Location, and Presenting SymptomsJournal of Cardiac Surgery 2006 21(4):435-40. [Google Scholar]
[10]. Terracciano LM, Mhawech P, Suess K, D’Armiento M, Lehmann FS, Jundt G, Calretinin as a Marker for Cardiac Myxoma Diagnostic and Histogenetic ConsiderationsAm J Clin Pathol 2000 114(5):754-59. [Google Scholar]