Ameloblastic Fibrodentinoma: Report of a Case in an Infant
Manish Bhargava1, Saloni Sood2, Pallvi Rathore3
1 Professor, Manav Rachna Dental College, Faridabad, Haryana, India.
2 Post Graduate Student, Manav Rachna Dental College, Faridabad, Haryana, India.
3 Post Graduate Student, Manav Rachna Dental College, Faridabad, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Saloni Sood, H No. 130, Block-H, DLF, Sector-10, Faridabad-121006., Haryana, India.
E-mail: salonisood7852@yahoo.com
Ameloblastic fibrodentinoma (AFD) is a debatable neoplasm with respect to its clinical, biological and histopathological diagnosis. The clinical and radiological presentation may mimic ameloblastic fibro odontoma, odontoma, ameloblastic fibroma and cemento-ossifying fibroma. We report an interesting case of AFD occurring in canine region of mandible in a one-year-old infant. From a review of English language literature, to the best of our knowledge this is the first case occurring in an infant. The purpose of this case report is to create awareness among the clinicians to make the best possible management of this controversial pathologic entity.
Ameloblast, Osteodentin, Odontogenic tumour
Case Report
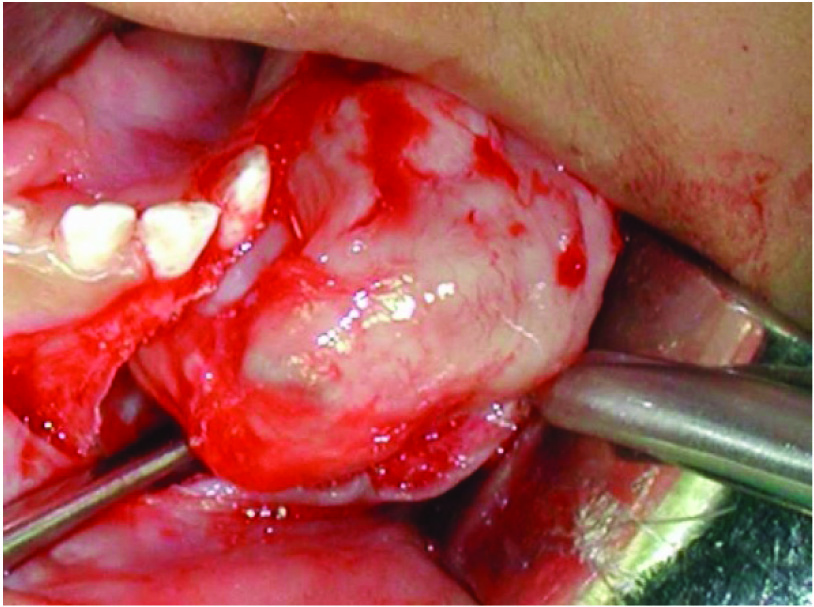
A one-year-old boy parents reported to the Department of Oral Medicine of S.D.M College of Dental Sciences, Dharwad with a chief complaint of swelling in the anterior part of lower jaw since birth which had been gradually increasing to the present size [Table/Fig-1]. Extra oral examination revealed a solitary diffuse, firm swelling measuring about 4X1 cm in size in relation the anterior mandible. Intra orally, a diffuse firm swelling was seen in relation to 71-73 region which was slightly tender on palpation. Radiological examination was not performed as the child was extremely un-cooperative. A provisional diagnosis based on the clinical examination was given as neurofibroma/ benign odontogenic tumour. Biopsy was performed under general anaesthesia, during the operative procedure as the lesional mass appeared to be well encapsulated, the entire mass was removed [Table/Fig-2].
Showing intra oral view of the swelling.

Showing entire lesional mass removed.
The gross tumour specimen was creamy white, lobulated mass. Cut surface showed a smooth translucent slimy surface with scattered dense whitish opaque foci. A tooth resembling 73 with incomplete root formation was also seen. Microscopically, neoplastic proliferation of odontogenic and mesenchymal tissues was seen [Table/Fig-3]. The odontogenic epithelial component consisted of multiple islands of peripheral palisaded ameloblast like columnar cells surrounding central stellate reticulum like cells [Table/Fig-4].
Showing neoplastic proliferation of odontogenic and mesenchymal tissue

Showing peripheral palisaded ameloblast like columnar cells surrounding central stellate reticulum like cells

The mesenchymal component was myxomatous, highly cellular stroma resembling primitive mesenchyme. The mineralized material consisted of strands of osteodentin [Table/Fig-5].
Showing strand of osteodentin

Enamel formation could not be identified on multiple sections. Ultimately a diagnosis of AFD was given. The post operative course was uneventful. The parents were informed of the low recurrence rate, but were made aware of a possibility of a delayed eruption.
Discussion
The diagnosis of oral lesions besides dental caries or periodontal diseases has been a challenge for general dentists. Most dentists usually associate swelling of jaws with dento alvelolar abscess even when there are no signs of inflammation leading to a wrong diagnosis. This in turn can alter the prognosis of cases that are easy to solve when a correct, timely diagnosis is made. Ameloblastic fibrodentinoma is an uncommon odontogenic neoplasm which predominantly presents as a slow growing swelling frequently occurring in posterior part of mandible, may be associated with a single or multiple unerupted teeth. Usually children, adolescents and young adults are affected. There is a male predilection with a male to female ratio of 3:1. Extremely rare but peripheral AFD have also been reported. As the tumour is well encapsulated, treatment of choice is usually enucleation or excision with a very low recurrence rate [1–5].
Since the first reported case of dentinoma was by Straith in 1936 [6]. Till date very few cases had been reported regarding ameloblastic fibrodentinoma in infants. There was a case of AFD in labial gingival of 2and 1/2-year-old female patient which was reported by Chen et al., [2]. This tumour is usually seen in younger age group, mostly below 30 years, however few cases have been reported in the older age group as well [4].
AFD is a rare odontogenic tumour usually associated with an unerupted tooth. In this case the lesion was associated with crown of a unerputed canine. AFD is generally seen in young adults with males more commonly affected than females with a predilection of 3:1 [7]. In the present case the child was just one-year-old. AFD related to primary teeth are usually seen in the anterior area while those related to permanent teeth develop in posterior area. Similar site predilection was present in our case [5].
Radiographically, AFD shows a well circumscribed radiolucent area containing variable amounts of radiopaque material making it virtually indistinguishable from a developing odontoma, therefore careful consideration must be given to the location and age of the patient [8]. According to the World Health organization, AFO is included, along with AF and ameloblastic fibrodentinoma (AFD), in the group of tumours of Odontogenic epithelium with odontogenic ectomesenchyme, with or without dental hard tissue formation [9]. The histological features of AF include odontogenic ectomesenchyme that resembles the dental papilla and strands or islands of odontogenic epithelium that resemble the dental lamina and enamel organ. If there is dentin formation, the lesion should be diagnosed as AFD; if there is also enamel formation, it should be diagnosed as AFO [10]. The nature and relationship between the so-called mixed odontogenic tumours (AF, AFD and AFO) and odontomas, which are regarded as hamartomatous lesions is still not clear. It is argued that mixed tumours are in fact neoplasms or yet different stages of a single pathology [1,5,10]. If that is the case then AF, AFD and AFO would represent different stages of the same lesion, which would eventually mature and develop into an odontoma. As a matter of fact, at different developmental stages, an odontoma may have histological features of AF, AFD or AFO [5]. However, the concept that these lesions represent a continuum of differentiation has been disputed for various reasons, among which lies the fact that patients who are affected by AF are generally older than those affected by AFO [3,4].
In support of this latter suggestion, Slootweg analysed 33 mixed odontogenic tumours and concluded that AF represents a separate specific neoplastic entity that does not transit into a more differentiated odontogenic lesion [5]. Philipsen et al., have suggested that AF and AFD occur in two variants (with indistinguishable histology). The first is a neoplastic lesion, which if left in situ does not appear to mature further. The second variant is a hamartomatous (non-neoplastic) lesion that appears to be able to differentiate into an ameloblastic fibroodontoma and mature further into a complex odontoma [3].
Clinically and pathologically, AFO and AFD are almost identical. But, in the revised version of WHO classification of odontogenic tumours, both these tumours had been considered as separate entities. Presence of tooth germ elements, e.g. enamel and dentin in combination, or only dentin, helps in the differentiation of the two lesions [11,12]. As in AFD, connective tissue resembles the dental papilla with only induction of dentin formation which is frequently preceded by zones of hyalinization [13]. In the present case, a definitive Odontogenic epithelium was seen in a cellular connective tissue stroma, showing dentin like areas, even after extensive sectioning enamel was not seen and so the present diagnosis of AFD was made based on clinical and histopathological correlation.
Thus, occurrence in a one-year-old child appears to be unreported so far, the youngest being case one and a half-year-old. [14] This adds to our knowledge of this interesting odontogenic entity, and is of special relevance to paediatric health-care providers since AFD usually occurs in young children.
Conclusion
Hereby, we present a case of AFD in one-year-old child which seems to be unreported so far. A regular follow up was maintained for 5 years, but patient did not report back to the department. More knowledge is required to understand this distinct controversial neoplasm with a regular follow up for the operated cases as there is a risk of malignant transformation and chances to recur.
[1]. Gardner DG, The mixed odontogenic tumoursOral Surg Oral Med Oral Pathol 1984 58:166-68. [Google Scholar]
[2]. Chen HS, Wang WC, Lin YJ, Chen YK, Lin LM, Gingival ameloblastic fibro-dentinoma – Report of a case in a childInt J Paediatr Otorhinolaryngol 2006 1:15-58. [Google Scholar]
[3]. Philipsen HP, Reichart PA, Praetorius F, Mixed Odontogenic Tumours and Odontomas. Considerations on Interrelationship. Review of the Literature and Presentation of 134 New Cases of OdontomasOral Oncol 1997 33:86-99. [Google Scholar]
[4]. Takyeda Y, Ameloblastic fibroma and related lesions: Current pathological conceptsOral Oncol 1999 35:535-40. [Google Scholar]
[5]. Slootweg PJ, An analysis of the interrelationship of the mixed odontogenic tumour:ameloblastic fibroma, ameloblastic fibroodontoma and the odontomasOral Surg 1981 51:266-76. [Google Scholar]
[6]. Straith FE, Odontoma. A rare type. Report of a caseDent Dig 1936 42:196 [Google Scholar]
[7]. Giraddi GB, Garg V, Aggressive atypical ameloblastic fibrodentinoma: Report of a caseContemp Clin Dent 2012 3:97-102. [Google Scholar]
[8]. Ahmed M, Sadat SM, Rita SN, Ameloblastic fibro-deninoma of mandible: A case reportJ Bangaladesh Coll Phys Surg 2006 24:119-21. [Google Scholar]
[9]. Kramer IR, Pindborg JJ, Shear M, WHO international Histological Classification of tumours 1992 2nd edBerlinSpringer VerlagHistological typing of odontogenic tumours; pp. 16–18 [Google Scholar]
[10]. Cavalcante AS Rodrigues, Anbinder AL, Costa NC Sena, Lima JR Sá, Carvalho YR, Ameloblastic fibro-odontoma: A case reportMed Oral Patol Oral Cir Bucal 2009 14:650-53. [Google Scholar]
[11]. Philipsen HP, Reichart PA, Revision of the 1992-edition of the WHO histological typing of odontogenic tumoursJ Oral Pathol Med 2002 31:253-38. [Google Scholar]
[12]. Barnes L, Eveson JW, Reichart P, Sidransky D, Pathology and genetics of head and neck tumours 2005 Lyon, FranceIARC PressWorld Health Organization classification of tumours; pp. 294–95 [Google Scholar]
[13]. Sangala NB, Munishekar M, Krishna A, Shylaja S, Ameloblastic fibrodentinoma of mandibleJ NTR Univ Health Sci 2014 3:66-69. [Google Scholar]
[14]. Jacob OA, Padmakumar SK, Aloka D, Sooraj S, Ameloblastic Fibrodentinoma: A 12 Years follow-up of a Rare EntityIJSS Case Reports & Reviews 2015 1(10):31-34. [Google Scholar]