The symphysis pubis which in Greek means “growing together.” is formed at the confluence of the pubic bones. Each pubic bone consists of a body and two rami; the superior ramus is joined with the ilium and the inferior ramus with the ischium. The two bones meet in the midline at the pubic symphysis, a secondary cartilaginous joint. The two inferior rami at the lower border of pubic symphysis subtends the subpubic angle or the subpubic arch. In Gynecoid pelves the subpubic arch is more than 900 and is called Norman type. In Android pelves this angle is acute i.e. less than 900 and is called Gothic type [1]. Enormous reports on pubic symphyseal region in different races made the region unique from research point of view [2–5]. Researchers were also engaged in finding out the mystery of pubic symphyseal anatomy from developmental point of view both during prenatal and postnatal periods [6,7]. Materials used for this purpose were animals as well as human beings [8–10]. Khomiakov et al., authentically used X-ray films of pelvis to measure subpubic angle for sexual dimorphism in young boys and girls [2], while Dihlmann and Heinrichs, performed pelvic roentgenometry for determination of age and sex in adulthood [11]. Luo highlighted the importance of subpubic angle for sexing the individuals and showed that sex could be determined with 100% accuracy [5]. Msamati et al., documented the importance of subpubic angle in terms of geographical variation [3]. According to him sex could be assigned with the help of subpubic angle with an accuracy of 67.12% in males and 63.04% in females. Nwoha concluded that the value of subpubic angle in female was obtuse but overlapped between acute and obtuse in males [12]. Igbigbi and Nanono-Igbigbi showed that 31.82% of Ugandan men and 10.53% of Ugandan female could be accurately sexed utilizing the subpubic angle [13]. They showed that the subpubic angle was significantly wider in women than men. Differentiation and steps in development had been thoroughly investigated during early embryology but changes involving organogenesis and fetal anatomy seemed to be deprived of adequate scientific attention [14]. Major informations relevant to embryology were based on animal experimentation. Most of the previous studies on the subpubic angle have been in children or adults, therefore data on fetuses did merit.
(1) To measure the subpubic angle in human fetuses.
(2) To find out the change in subpubic angle in different fetal age groups.
(3) To find out sexual dimorphism in subpubic angle in fetuses.
(4) To compare the result in fetuses with that in the adults.
Materials and Methods
A cross-sectional study conducted in the Department of Anatomy J.N. Medical College. AMU Aligarh over a period of two years between October 2004 to August 2006, after taking institutional ethical committee clearance. A total of 41 fetuses immersion fixed in 10% formalin were obtained from the anatomy department museum.
Fetuses of all age groups mainly of north Indian origin without congenital craniovertebral anomalies were selected for the study. Gestational age of the fetuses was determined using fetal foot length. Fair correlation between foot length and gestational age had been documented [15]. Sexes of the fetuses were determined by observing the external genitalia. For the purpose of study fetuses were divided into five groups, according to gestational age with each group having male and female fetuses. Group I comprised fetuses of 14–18 weeks (5males & 5females), group II- 19–22 weeks (5 males & 5 females), group III- 23–26 weeks (3males & 4females), group IV- 27–30weeks (4males & 3females) and groupV >30weeks (3males & 4females).
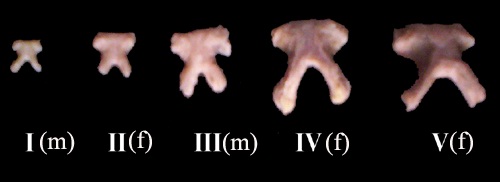
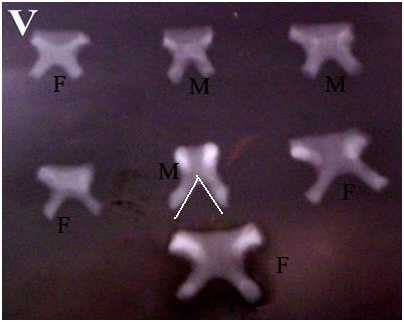
The pubic symphyses were dissected out and cleaned of all the adhering tissues, under a dissecting microscope to expose the subpubic angle clearly [Table/Fig-1]. The isolated symphyses thus obtained were subjected to radiological examination in the anteroposterior plane. The radiographs were put on a view box. A tangential line was drawn along the medial border of the inferior pubic ramus on both the sides which contribute to the formation of pubic arch. The angle formed by convergence of these two lines at the symphysis was measured with the help of a protractor [Table/Fig-2]. The readings obtained were analysed statistically using student t-test.
Ventral aspect of isolated pubic symphysis region, one from each group I-V. (m-male, f-female).
X- ray of group V (>30 weeks gestation) pubic symphyseal region and measurement of subpubic angle. (M=male, F=female).
Results
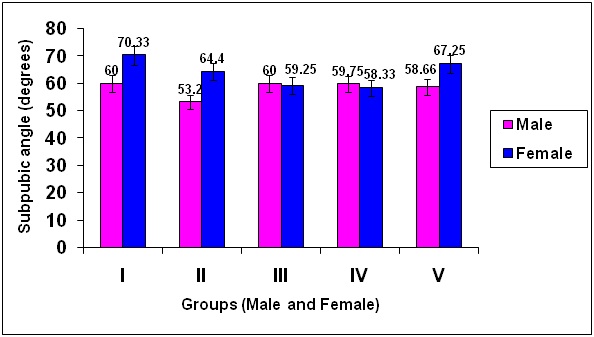
The subpubic angle ranged between 58°- 64° throughout intrauterine life. Maximum angle (63°- 64°) was observed in group I and V and in the rest of the groups it was always less than 60° [Table/Fig-3]. Sexual dimorphism was observed in the subpubic angle in group I and II fetuses where p-value was highly significant (< 0.001) and in group V with p-value < 0.02 [Table/Fig-3,4]. It was noted that the subpubic angle was more in females during the first half of gestation i.e.14–22 weeks, (p-value < 0.001) which gradually reduced to become almost equal to the males in the later stages of intrauterine life i.e. 23– 30 weeks and then increased thereafter i.e. beyond 30 weeks, with p-value<0.02 [Table/Fig-3].
Subpubic angle (degrees) in different groups and sexual dimorphism.
| FetalGroup | I | II | III | IV | V |
|---|
| No. of cases (n) | T(10) | M(5) | F(5) | T(10) | M(5) | F(5) | T(7) | M(3) | F(4) | T(7) | M(4) | F(3) | T(7) | M(3) | F(4) |
|---|
| Mean± SD | 64.27±11.44 | 60.00±9.57 | 70.33 ±9.37 | 58.45±7.09 | 53.20 ±4.12 | 64.40 ±5.31 | 59.57±9.88 | 60.00 ±9.42 | 59.25 ±10.21 | 59.14 ±7.64 | 59.75 ±9.28 | 58.33±4.50 | 63.57 ±7.29 | 58.66 ±6.65 | 67.25 ±5.31 |
| p-value | - | <0.001 | <0.05 | <0.001 | <0.50 | <0.50 | <0.8 | <0.50 | <0.001 | <0.02 |
| %difference | - | 15 | 9 | 17 | 2 | 1 | 0 | | 7 | 13 |
T-total, M-male, F-female
Sexual dimorphism in subpubic angle.
Discussion
Size and shape of the skeleton can be utilized for sex determination which starts to manifest as early as fetal life. The degree of sexual dimorphism varies between populations, and it can decrease within a population as a result of environmental stresses [16], it has an ethnic variation as well [17]. Many authors have done morphometry of fetal long bones to determine age and sex of the fetus [18] as well as fetuses at risk of Down’s syndrome [19].
Complete cartilaginous pelvis is present by the beginning of the second month of development, the centre of chondrification arise in the primitive scleroblastema on either side, grow together in the midline forming the precursor of the pubic symphysis [9]. Symphysis pubis is formed at about the beginning of the third month of development [20]. Primary centres of ossification for ilium appear in ninth week, ischial centre in fourth month, and the pubic centre during fifth month. Secondary centres appear at about puberty and fuse between 15th and 25th years forming the hip bone, the unossified cartilage forming the symphysis pubis. Differential growth of the pubis is expressed in the subpubic angle below the symphysis and between the two inferior pubic rami. It is more angular in males, being 50°–60° while in females it is rounded, less easy to measure and usually 80°–85° [21].
Fetal pelvic bones has been utilized as a marker for predicting fetuses at risk of trisomy of chromosome 21 during the second trimester of pregnancy [22,23] and gender differentiation. Morphometric study of greater sciatic notch by Boucher and Schutkowski revealed that it is wider in females while depth of the notch is more in males [17,24]. According to Biwasaka et al., sex could be correctly identified in 89.1% of cases utilizing curvature of great sciatic notch and in 94.7% of cases by determining the pubic arch [25].
Pubic symphysis which subtends the subpubic arch below it, exhibit features which can be authentically utilized during fetal life for sex determination as well as for prediction of congenital diseases such as urinary bladder exstrophy and risk of Down’s syndrome.
In the present study the mean subpubic angle ranged between 58°-64° throughout intrauterine life. Maximum angle of 64.27°±11.44° was observed in group I fetuses. Immediately in the next group II there was a drop (-9%difference) in the angle, mean value being 58.45°±7.09°, thereafter in group III and IV there was minimal increase in the angle, with spurt (+7%difference) in the last group V, mean angle 63.57° ±7.29° [Table/Fig-3]. No data on fetal subpubic angle is available in literature for comparison. Most of the studies are in children and in adults. When the results were compared with those of the adult [13] it is obvious, the values of our findings in intrauterine life are quite low (70° or less). Therefore the change in morphology of subpubic angle is a continuous process even after birth. The widening of subpubic angle making it obtuse in nature therefore seemed to be a postnatal phenomenon, may be post pubertal as suggested by Boucher [17]. Nwoha found that subpubic angle was significantly greater in older age group than in younger age group [12]. If we correlate the widening of subpubic angle with aging then the highly significant increase (p-value < 0.001) in the last group of fetus is a striking feature. Not necessarily the subpubic angle undergoes widening but narrowing may also be noted in later age groups. The view was supported by the findings of Tague who showed that the subpubic angle narrowed with advancing age in both sexes [4]. This narrowing was observed in group II fetuses and near static growth in group III (+2%difference) and group IV (0% difference). May be after initial appearance of primary ossification centres the skeletal growth slows down naturally or because of the nutritional status of the population group studied.
When the subpubic angle was compared between the sexes, sexual dimorphism was observed in group I and II where p-value was highly significant (<0.001) and in group V (p-value<0.02) fetuses. In group III (+1%difference) and IV (+2%difference) fetuses the subpubic angle was almost equal in both sexes.
Subpubic angle was invariably considered by scientists to determine the sex which can be observed even in fetal life. Fazekas and Kosa after studying human fetuses, pointed out that subpubic angle is larger in females as compared to males however we observed this phenomenon only in group I, II and in group V fetuses [26]. In group III and IV the subpubic angle was almost equal in both sexes. A highly significant p-value in group I indicates sexual dimorphism as early as 14-18 weeks of gestation.
Khomiakov et al., investigated subpubic angle in children and adolescent whose age ranged from 11-16 years [2]. They classified three forms of subpubic angle in boys i.e. right (most often occurring), obtuse and acute (seldom occurring) in order of preference and two forms in females i.e. obtuse and right with definitive predominance of obtuse angle. They concluded that formation of feminine type of subpubic angle takes a longer period of time than the masculine type. We observed maximum difference (+17%) in the subpubic angle between the two sexes quite early in fetal life, at 19-22 weeks of gestation (group II).
Most of the studies related to sexual dimorphism of the subpubic angle have been done in adults. Ubi et al., using radiographic films of adults between 18 -80 years of age from Cross River and Akwa Ibom States Indigenes, Nigeria found statistically significant sex difference in the sub-pubic angle with a range of 80°-144° in males and 96°-142° in females [27]. Daniel et al., has suggested that subpubic angle can contribute significantly to sex discrimination with accuracy rates between 81.2% and 100% [28], while it is 90.8% according to Karakas et al., [29]. According to Small et al., who measured subpubic angle from the digital images of the pelves, concluded that significant difference exists between the sexes which also have a regional variation [30].
All these studies indicate towards a sexual discrimination according to the subpubic angle in adults which is also obvious in this study on fetuses although not throughout the fetal life.
Conclusion
Subpubic angle remained acute throughout the intrauterine life. Marked sexual dimorphism was noticed for subpubic angle in fetuses of 14–22 weeks of gestation, although the values were invariably less than 90° (acute) in both the sexes but in females towards the higher side as in adults.
Determining the subpubic angle of the fetuses during routine antenatal ultrasonography of pregnant women can be done to diagnose congenital widening of the symphysis or absence of symphysis altogether leading to postnatal pelvic instability or congenital exposure of urinary bladder alone and or part of a syndrome like cliedo cranial dysostosis. However, the visualization of pubic symphysis and the symphyseal arch is not easy and it requires a very experienced ultrasonologist.
T-total, M-male, F-female