Distal radius fractures constitute one sixth of all fractures that present to the Emergency Department and foster considerable interest and debate in orthopaedic fraternity [1]. The number of distal radius fractures continues to increase as the population ages. Distal radius fractures are the third most common fractures in osteoporotic fractures following vertebral and hip fractures [2]. There are three main peaks of distal radial fracture occurrence. First peak is between ages 5 to 14, the second in males under 50 years of age and the third peak is in females over the age of 40 years [3–5]. There is a growing incidence of these fractures in all the three groups with significant increase in elderly females and younger adult males [4–6]. It is suggested that the two peaks represent two very different injury patterns: 1) An insufficiency fracture in elderly females [7]; 2) Traumatic injury in younger males. There is clear evidence to suggest a higher morbidity and mortality rate after distal radius fractures (osteoporotic fractures) particularly in elderly males akin to osteoporotic hip fractures [8]. The present study was aimed at measuring the effectiveness of external fixator in treating the complex distal end of radius fractures with respect to functional outcome, complications, ease of application and cost effectiveness.
To study osteosynthesis in distal radius fractures by Ligamentotaxis (Bridging External Fixator) and to assess the functional outcome in distal radius fractures treated by ligamentotaxis (Bridging External Fixator) using the parameters like pain, deformity, radiological union and range of movements at wrist.
Materials and Methods
A total of 26 patients who presented with fresh closed/open distal end radius fractures and fulfilling the inclusion/exclusion criteria were included in this prospective study. All the patients between 18-75 years of age with acute (<7 days) closed and open distal radius fractures are included and the patients below 18 years of age with existing deformities of forearm/wrist, patients with co-morbid conditions rendering them unfit for surgery, patients with polytrauma and Barton’s Fracture were excluded.
Data Collection
All the necessary clinical data was recorded using a proforma prepared for the study. After operative treatment, patients were discharged and followed up in our out-patient department at specific intervals for radiological and clinical evaluation.
Fracture Management
Closed distal end radius fractures were preoperatively managed by application of dorsal slab. Open fractures were managed by thorough saline and antiseptic wash followed by debridement. Primary suturing was done in clean open wounds and a plaster slab was applied. Antibiotics covering both aerobic and anaerobic microorganisms were given. Radiographs of forearm with wrist joint in postero-anterior (PA) and lateral view were taken and the fractures were classified according to Frykman’s classification [9] [Table/Fig-1].
Frykman’s Classification [9]
| Fracture | Distal Ulnar Fracture |
|---|
| Absent | Present |
|---|
| Extra articular | I | II |
| Intra articular involving radiocarpal joint | III | IV |
| Intra articular involving distal RU joint | V | VI |
| Intra articular involving both radiocarpal & distal radioulnar joints | VII | VIII |
Instability was judged by Cooney’s criteria [10] namely: a) Marked dorsal comminution of distal end of radius; b) Dorsal angulation more than 20 degrees; c) Fracture involving wrist joint with articular step more than 3 mm; d) Loss of reduction with dorsal angulation more than 10 degrees and 5mm or more radial shortening after closed reduction.
Having concluded the diagnosis pre-anaesthetic check up was done and once the patient is declared fit, operative intervention was contemplated after explaining the details of surgery and written informed consent was taken.
Surgical Approach and Procedure
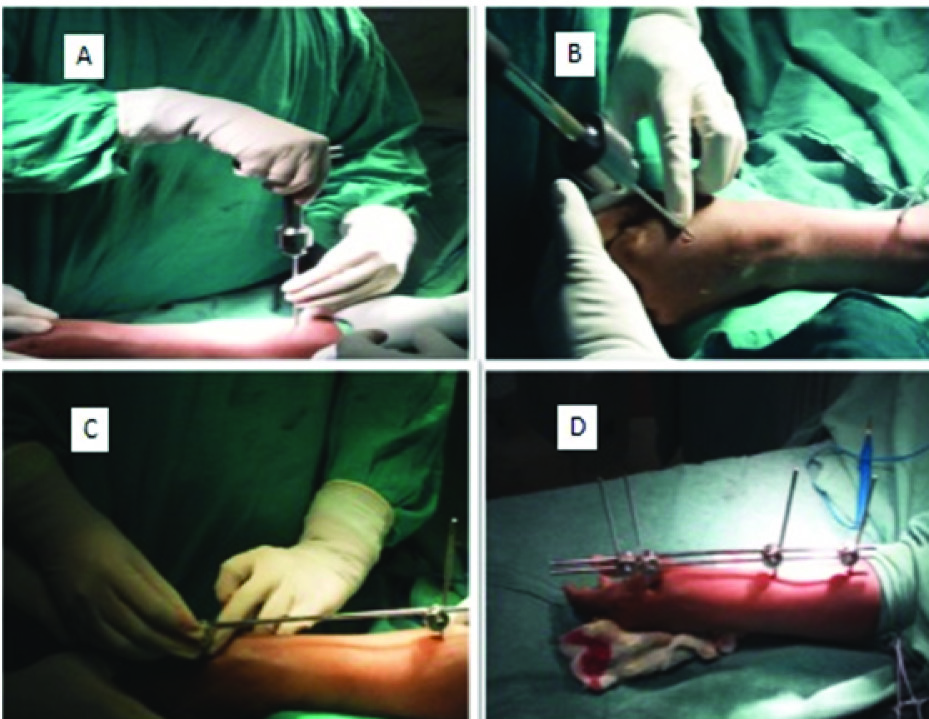
Longitudinal traction is given with elbow in 90 degrees of flexion while the fracture is being reduced with the wrist in flexion and ulnar deviation. Tissues, muscles planes were dissected till the bone is felt and care is taken to protect the radial sensory nerve. Radius is predrilled with 3.5mm drill bit in 20 degrees dorso lateral to longitudinal plane and 3.5mm schanz pins are inserted bicortically with T-handle between extensor carpi radialis longus and brevis. Index metacarpal is approached through a 2cm longitudinal incision over the dorsoradial base. The bone is predrilled with 2.5mm drill bit and then 2.5mm schanz pins are placed bicortically.
Small Ausculap clamps were adjusted over the schanz pins through which interconnecting rods are passed. The clamps on the radial side were tightened. Holding the fracture in the reduced position, the clamps on the metacarpal side were tightened and fixed. The reduction is confirmed by fluoroscopy. K-wires were used for supplementary fixation of distal radio-ulnar instability or for Radial styloid fragment. Criteria for acceptability of fracture reduction as enumerated in [Table/Fig-2] are followed. Suturing and aseptic dressing was done [Table/Fig-3].
Criteria for acceptable reduction.
| Parameter | Normal value | Acceptable limit |
|---|
| Radial inclination | 22 degrees | 15 degrees or more |
| Radial height | 11mm | 6mm (<5 mm shortening) |
| Dorsal/Volar angulation | 11 degrees Volar | 15 degrees dorsal, 20 degrees Volar |
| Articular congruity | Congruous | < 2mm gap or step off |
Source nana AD, Joshi A, Lichtman DM. Plating of the Distal Radius. J Am Acad Orthop Surg 2005;13(3):159-71.
Sequential intra-op clinical photographs showing the procedure of application of bridging external fixator.
Postoperative Protocol
Forearm is kept elevated for 24 hrs and active finger, elbow and shoulder movements were started. I.V antibiotics, antacids and I.M analgesics were given in the immediate postoperative period followed by oral medication for another 5 days. Pin tract care was explained to the patient and his care takers. The patient is encouraged to use the effected hand for daily activities within the permissible limits of pain. Most of the patients were discharged on 2nd or 3rd post-op day. Patients were reviewed after 1 week for suture removal, radiological assessment. In case of any collapse at the fracture site, distraction is adjusted accordingly. Supplemental K-wires were removed at 3 weeks. Assessment for radiological fracture healing was done at 3 and 6 weeks and most of the external fixators were removed at 6th post-op week and monitored physiotherapy was started. Further review was done at 3 and 6 months [Table/Fig 4,5] and all the data was collected using a standard proforma.
(a) Pre-op radiograph showing distal radial fracture; (b) Post –op radiograph showing insitu K wires with external fixator; (c,d) 3 months Post–op clinical photograph showing unrestricted range of motion of left wrist.
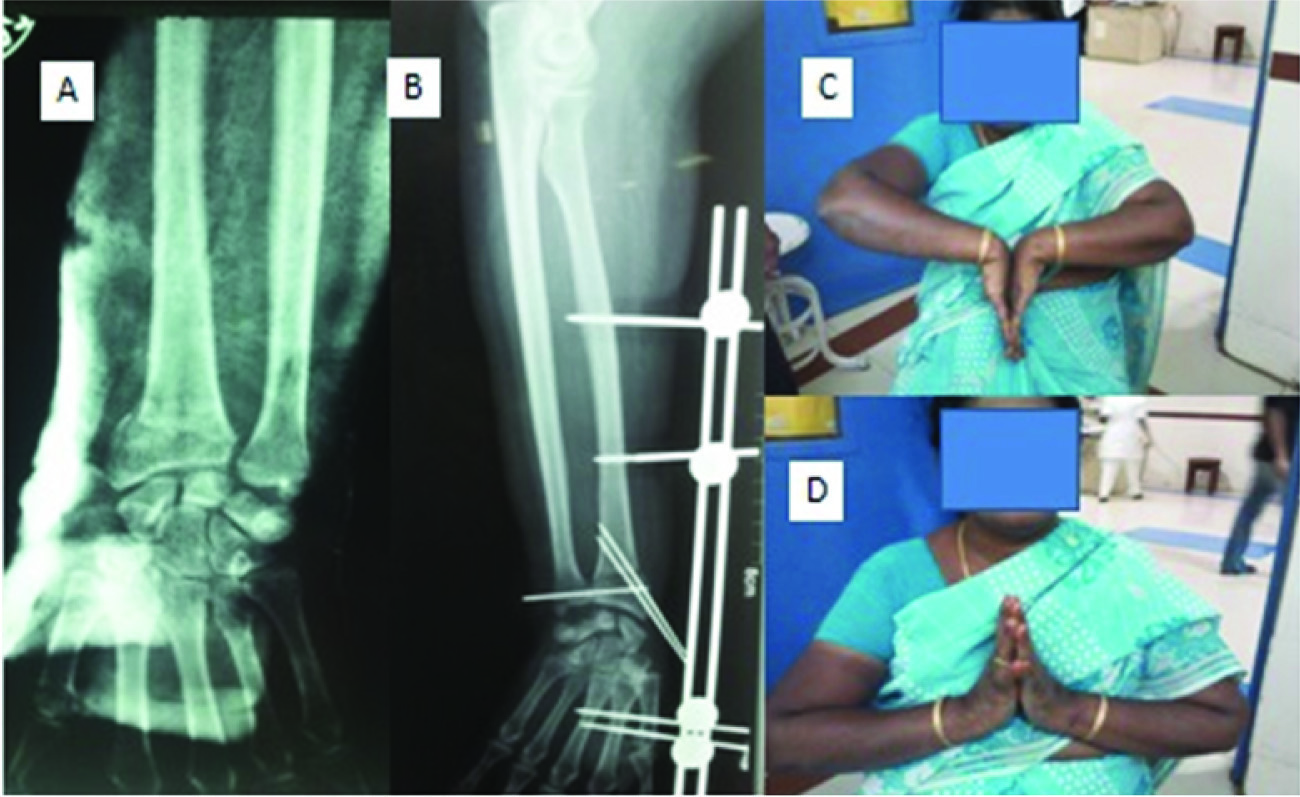
Sequential Pre-op, Intra-op and Post-op pictures of 2 patients: (a,b) showing comminuted distal radial fracture treated by bridging external fixator with acceptable reduction.

Results
In our study 26 cases were included and all of them were followed up for an average period of 9 months. 73% (19 of 26 cases) of patients were above 40 years of age and the mean age of the study population was 47 years (range 18 years to 70 years), 15 (57.69%) were male and 11 (42.31%) were female. The right wrist was involved in 57.69% (15 cases) and the left in 42.30% (11) of our cases, 19 cases (73.07%) were closed and 7 cases (26.92%) were open fractures. 38.4% of our cases were with complex intraarticular fractures i.e. Frykman type VII and VIII and constituted 52% of cases among patients with 40-60 years of age. Number of cases due to road traffic accidents was 61.53% and 34.61% were due to falls.
Most of our cases were treated with external fixator on the day 1 within 8 hours of injury (range 4 hours to 3 days). Fixator was removed after 6 weeks followed by hot paraffin wax bath and physiotherapy. The follow-up period averaged 9 months, highest being 18 months and the least being 6 months. In 80.76% of cases radiological union was noticed in 6-8 weeks. One case had complex regional pain syndrome which resolved in 2 months with rigorous physical therapy and medication. One case had superficial pin tract infection which resolved with local wound care and antibiotics. Three cases (11.53%) had wrist stiffness. Marked improvement was seen after two weeks of physiotherapy. Malunion was seen in 2 cases (7.69%), which was primarily due to inability to correct the dorsal angulation.
Modified demerit point system of Gartland and Werley was used to evaluate the overall functional results {[Table/Fig 6]- Master Chart}[11]. Excellent to good result was achieved in 88.45% of our cases while fair result was achieved in 11.54 % of cases of which 1case had pin tract infection/loosening and the other 2 cases had malunion. There were no cases with Poor results in the present study.
Master chart/functional outcome
| S. No. | Age | Sex | Side | Mode of injury (D-Domestic) | Frykman’s classification | Closed/ Compound Gartland grade- (Gr) | Trauma to treatment time | Treatment used | Duration of external fixator | Complications | Gartland and Werely score | Result |
|---|
| 1 | 60 | F | Left | Fall (D) | II | Closed | 2 days | K-wire + Ex-fix | 6wks | – | 6 | Good |
| 2 | 45 | M | Left | RTA | VII | Gr-I | 12 hours | Ex-fix | 6wks | – | 5 | Good |
| 3 | 29 | M | Left | RTA | III | Gr-I | 5 hours | K-wire + Ex-fix | 6wks | – | 4 | Good |
| 4 | 48 | F | Right | RTA | I | Closed | 10 hours | Ex-fix | 6wks | Stifness-resolved | 6 | Good |
| 5 | 68 | F | Left | Fall (D) | VII | Closed | 3 days | K-wire + Ex-fix | 6wks | – | 5 | Good |
| 6 | 42 | M | Right | RTA | VII | Gr-II | 6 hours | Ex-fix | 6wks | – | 5 | Good |
| 7 | 50 | F | Left | Fall (D) | I | Closed | 10 hours | K-wire + Ex-fix | 6wks | – | 4 | Good |
| 8 | 37 | M | Right | RTA | V | Closed | 6 hours | Ex-fix | 6wks | Malunion | 9 | Fair |
| 9 | 63 | M | Right | RTA | VII | Gr-I | 8 hours | K-wire + Ex-fix | 6wks | RSD, Malunion | 10 | Fair |
| 10 | 64 | F | Right | Fall (D) | III | Closed | 3 days | Ex-fix | 7wks | Stifness-resolved | 6 | Good |
| 11 | 49 | F | Left | Fall (D) | I | Closed | 10 hours | Ex-fix | 6wks | – | 2 | Excellent |
| 12 | 36 | M | Right | Sports injury | VII | Closed | 2 days | K-wire + Ex-fix | 6wks | – | 6 | Good |
| 13 | 52 | F | Right | RTA | VII | Gr-I | 8 hours | Ex-fix | 6wks | – | 2 | Excellent |
| 14 | 54 | M | Right | RTA | VI | Closed | 4 hours | K-wire + Ex-fix | 6wks | – | 4 | Good |
| 15 | 62 | F | Right | Fall (D) | III | Closed | 12 hours | Ex-fix | 6wks | – | 4 | Good |
| 16 | 52 | M | Left | Fall (D) | VII | Closed | 2 days | Ex-fix | 6wks | – | 4 | Good |
| 17 | 23 | M | Right | RTA | VII | Closed | 5 hours | K-wire + Ex-fix | 6wks | – | 2 | Excellent |
| 18 | 53 | F | Right | Fall (D) | VI | Closed | 8 hours | Ex-fix | 6wks | – | 5 | Good |
| 19 | 62 | M | Left | RTA | VIII | Closed | 6 hours | K-wire + Ex-fix | 7wks | Pin infection | 9 | Fair |
| 20 | 52 | F | Right | RTA | VI | Closed | 10 hours | Ex-fix | 6wks | – | 2 | Excellent |
| 21 | 19 | M | Left | RTA | VI | Gr-I | 6 hours | Ex-fix | 6wks | Stifness-resolved | 6 | Good |
| 22 | 70 | M | Right | RTA | II | Closed | 12 hours | K-wire + Ex-fix | 6wks | – | 2 | Excellent |
| 23 | 34 | M | Left | RTA | II | Gr-I | 8 hours | K-wire + Ex-fix | 6wks | – | 5 | Good |
| 24 | 43 | F | Left | Fall (D) | III | Closed | 8 hours | Ex-fix | 6wks | – | 2 | Excellent |
| 25 | 18 | M | Right | RTA | VI | Closed | 6 hours | Ex-fix | 6wks | – | 5 | Good |
| 26 | 40 | M | Right | RTA | VII | Gr-II | 2 days | Ex-fix | 6wks | – | 4 | Good |
Discussion
Distal end of radius fractures are one of the common fractures managed by an orthopaedic surgeon [12]. Treatment outcomes are not uniformly good irrespective of the treatment modality. Number of studies have proved that there is a strong relationship between the quality of anatomical reconstruction and long term functional outcome [13–19].
The small A.O external fixator provides a simple and a reliable means of treating these fractures, especially unstable intraarticular fractures according to the concept of Ligamentotaxis that was proposed by Vidal et al., [20]. It uses the principle of distraction of intact ligaments in a complex comminuted scenario to bring back the fragments in place and hold them in position till the fracture unites.
If adequate closed reduction can be obtained, external fixator maintains the reduction with constant distraction of ligaments which hold the fracture fragments in place until solid union occurs. Biomechanical studies by Nakata et al., revealed that A.O devices resist axial loading better in comparison to most of the other fixators [21]. Brinker et al., showed better resistance to axial loading with two rows of interconnecting bars [22]. In the present study the average time of union was 7.2 weeks which is comparable with other studies. The comparative statistics of functional outcome in distal radial fractures managed by various methods can be seen in [Table/Fig-7].
Comparative statistics of functional outcome.
| S. No | Name of Series | Modality of treatment | No of cases | Functional result (Good to Excellent) | Functional result (Fair to poor) |
|---|
| 1 | Dowling and sawyer [23] | Per cutaneousPinning | 51 | 84% | 16% |
| 2 | Cooney et al., [24] | Roger Anderson frame | 60 | 87% | 13% |
| 3 | Jakim I et al., [25] | Hoff-mann vidal frame | 132 | 83% | 17% |
| 4 | Present study | A.O* | 26 | 88.45 | 11.54% |
*Arbeitsgemeinschaft fur Osteosynthesefragen
Apart from the above, plate osteosynthesis in osteoporotic comminuted fractures (barring Bartons fractures and fracture dislocations) is technically demanding, costly and often demands additional bone grafting with the necessity of second surgery to remove the implants at a later date [26]. In case of difficult intraarticular reductions minimal access fragment reduction and maintenance with K wires augmented with external fixation appears to be advantageous in comparison to the fragment devitalising conventional open plating and 10 times costlier fragment specific plating systems. Bridging external fixator with ligamentotaxis is cost effective and has a distinct advantage over the other modalities mentioned above in complex intraarticular and comminuted extra articular fractures of the distal end of radius.
Satisfactory results in this study may be attributed to the recognition and definition of unstable injury at the initial assessment, careful patient selection, simplicity of the technique, careful postoperative management and aggressive early rehabilitation. It appears that the improved anatomical restoration with early rehabilitation does produce favourable functional outcome and the same is concurrent with the existing literature in this regard. A larger study in this context of indigenization of the bridging external fixator would further add to the existing literature.
Tips and Tricks to Get Them Right
Select proper fracture for Ligamentotaxis external fixator. Once the fixator is removed volar bartons often end up in volar subluxation.
Always position the distal end of forearm on a folded towel to allow ulnar deviation and flexion.
Always fix the fracture in near reduced position i.e. reduce the fracture first and then maintain it by ex.fix.
Hold the position of forearm and hand in reduced position till all the pins are inserted.
Universal principles of external fixation should be strictly adhered to.
Apply distal and proximal pins first, hold them in place with connecting a rod and then insert rest of the pins.
Insert pins in the 2nd metacarpal at an angle so that they become straight on traction which ultimately maintains the radial inclination.
Traction should be given at the base of the pins in 2nd metacarpal before fixation of the construct.
Check radio carpal and intercarpal space to prevent over distraction which usually ends up in dorsiflexion of the distal fragment.
Manipulation with k wires passed through the fracture site may be useful for reduction of impacted fractures fragments.
Supplement the fixation with K-wires when the fracture fragments are unstable including distal radio-ulnar joint.
Donot bend the connecting rods for maintenance of flexion and ulnar deviation.
Brachioradialis may have to be released from the radial styloid fragment by mini incision in certain cases of decreased radial height & inclination despite distraction.
Take prophylactic measures to prevent RSD, elbow and shoulder stiffness.
Use appropriate drill bit and donot drill the shantz pins directly into radius and 2nd metacarpal.
Conclusion
The use of external fixator is an effective method of treating unstable extra-articular and complex intra-articular fractures of the distal end of radius. The small A.O external fixator is a simple device which is easy and safe to use even under regional anaesthesia with the distinct advantage of superior mechanical efficiency and capacity of fracture adjustment during healing period and unimpeded access to wounds in cases of open fractures. The shorter period of surgery, less tourniquet time and minimal exposure are its distinct advantage over plate fixation. It can be performed in emergency with minimum instrumentation and expertise. Complications like pin tract infection are rare. Wrist and finger stiffness can be avoided by appropriate physiotherapy. Hence, properly planned and executed bridging external fixator is an easy, cost-effective and reliable treatment modality in treating intra-articular and unstable extra-articular distal end of Radius fractures by the “Principle of Ligamentotaxis”
*Arbeitsgemeinschaft fur Osteosynthesefragen